BEYOND SHYNESS Evidence Based Assessment and Intervention for

BEYOND SHYNESS: Evidence Based Assessment and Intervention for Selective Mutism Katelyn Reed, MS, LLP Taylor Hicks-Hoste, Ph. D. , LP, NCSP
 • Specific anxiety disorder • Consistent, ongoing failure to speak")
Definition of SM (DSM-V) • Specific anxiety disorder • Consistent, ongoing failure to speak in specific social situations, especially school • Not due to a primary language disorder • Other disorders (e. g. , stuttering, autism) have been ruled out • At least one month in duration (not limited to the first month of school) • Behavior is deliberate self-protection, not deliberate oppositionality

Common Traits Mutism Blank facial expression, freezing, poor eye contact Difficulty responding and/or initiating nonverbally Heightened sensitivity Excessive worries Oppositional/bossy/ inflexible behavior at home Intelligent Slow to respond Bilingual

Shyness vs. Selective Mutism Shyness • Slow warm up period • Can often respond with a nod or small smile • Same demeanor everywhere – quiet and reserved Selective Mutism • Warm-up time MUCH longer than expected • Cannot respond at all may appear frozen • Dual personality – restrained at school and talkative at home

Where Does SM Originate? • NO evidence of causal relationship to abuse, neglect, or trauma • Genetic predisposition model (genetic loading) • Biological indicators Decreased threshold of excitability in amygdala • Amygdala reacts more and takes longer to return to normal •

Conceptualizing Selective Mutism Child is prompted to speak or engage Increased likelihood of avoidance Child gets too anxious and avoids Negative reinforcement of behavior Adult rescues Decreased anxiety (child and adult)

Common Comorbidities • Other anxiety diagnoses • • • Social Anxiety Separation Anxiety Generalized Anxiety OCD Specific Phobias • Speech and language disorders/delays (Manassis, 2003; Klein et al, 2012) • Oppositional behavior

Prevalence Statistics • Most recent stats show approximately 1%. . and growing? • 1. 5 -2. 6 / 1 female / male Garcia et al (2004)
 to assess skills • Risk")
School Implications • Academic implications Difficulty (if not inability) to assess skills • Risk of falling behind due to less practice than their peers • High state of anxiety during the school day may contribute to attention concerns • Children with SM are often unable to ask clarifying questions • • Behavioral implications Participation (partnered work, small group, full class) • Bathroom accidents • Often need additional assistance to get needs met in school • • Social Implications Social skill dyfluencies (due to lack of practice) • Decreased chances for engagement, resulting in fewer opportunities for practice of social problem solving skills •

ASSESSMENT AND INTERVENTION
 • School Speech Questionnaire (SSQ) • Videos")
Evaluative Tools • Selective Mutism Questionnaire (SMQ) • School Speech Questionnaire (SSQ) • Videos from home • And…. • • • BASC SCARED (Self-Report for Childhood Anxiety Related Disorders) for 8+ Autism Diagnostic Observation Schedule (ADOS-2) Speech/language evaluation IQ (nonverbal) Etc…

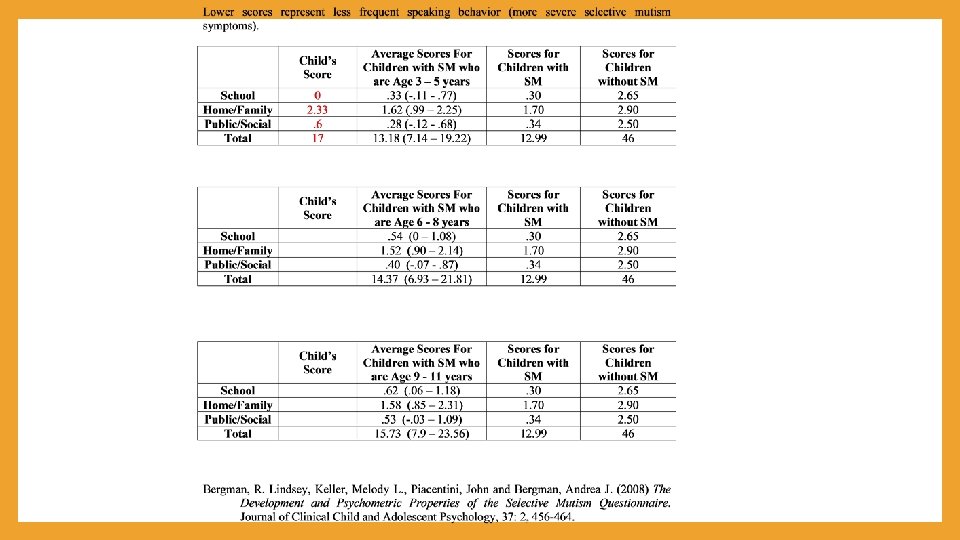
Scoring 1. Add totals in each section 2. Divide by number of items in section 3. For total score, add up totals in each section – DO NOT divide 0+0+0+0=0/ 6=School=0 3+2+2+3+2+2=1 4/6= Family=2. 33 0+1+2+0+0=3/5 = Other=. 6 Total 0+14+3=17

Behavioral Observation Condition Comments: Who did s/he communicate to? Parent Sibling Novel person What did s/he say? How did s/he communicate? Respond Nonverbal Initiate Whisper Altered Voice/ Appearance One word 2 -3 words Longer utterance Track: Open-ended: Forced Choice: Nod/Shake: Point: “Counting” with fingers: Other: Strategies utilized or suggested:

Testing Accommodations • Nonverbal testing methods, when possible • Parents trained to administer, clinician monitors administration and scores (work of Klein, Armstrong and colleagues) • Rapport and speech building session to be conducted before testing • Limitations to validity is assumed Children with SM more likely to provide 1 word or other short responses for professionallyadministered measures (Gray, Jordan, Ziegler, & Livingston, 2002) • Children with SM may be unable to take “educated guess” for items approaching their individual ceiling • May be unable to ask clarifying questions • All data likely under-estimate true ability •

Research on Behavioral Treatment • Most supported treatment per research (Kratochwill, 1981; Krohn et al, 1992; Leonard & • Effective in increasing production of speech in social situations ( Stone & Kratochwill, • RCT: 75% of children in the behavior therapy condition responded to treatment (e. g. , showed increased functional speaking) while children in the waitlist condition did not show significant change (Bergman et al. 2013) • Even more effective when combined with behavioral school and home-based exposure program (Bergman, 2005) • Exposure-based practice may be more effective than parent-focused contingency management (Vecchio & Kearney, 2008) • Gains made in school-based intervention plans maintained in 5 year follow-up studies (Oerbeck et al, 2018) Topol, 1993; Tancer, 2002, etc. ) 2002)

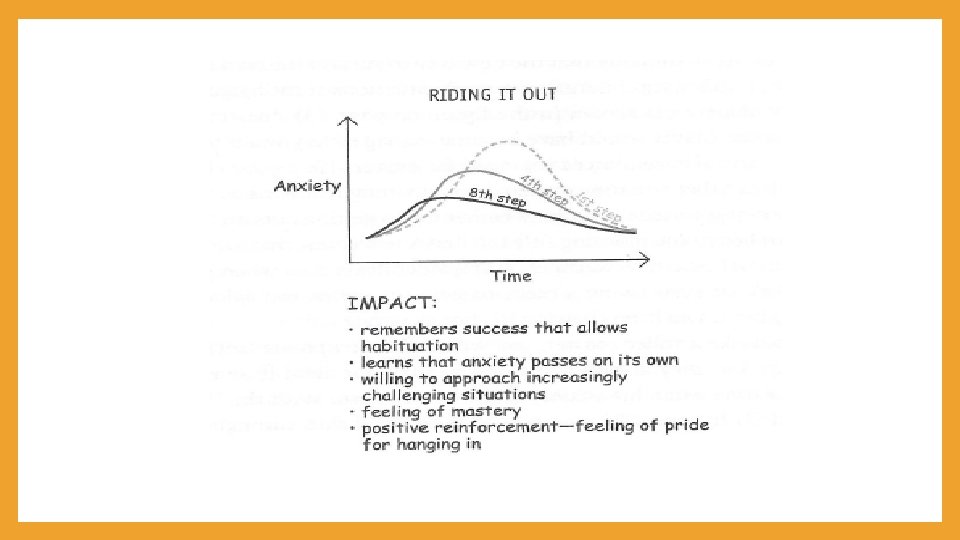
Psychoeducation • Brain “tricks” us and tells us things are very scary when they are uncomfortable but manageable • Need to boss back our brains and try being BRAVE • Sour candy metaphor • Using Subjective Units of Distress Scale 1 -5 or 1 -10 • Easy/Medium/Hard •

Exposure Model • Face fears at a reasonable pace • Scaffold verbal demands such that they move from easier to harder • Build bravery with each practice (reduce anxiety with each practice) • Practice repeatedly • • Shorter, but more frequent sessions, if possible Offer reinforcement for task completion • Stickers, points, weekly log that is communicated to parents

0 1 -2 times more Goal: 1. 2. 3. 4. 5. Bonus!! Did something really awesome!! 3 -4 5 or times

Avoid Accidental Rescuing

Child Directed Interaction Skills • PRIDE skills • • • P- Praise R- Reflection I- Imitate D- Describe E- Enthuasiasm

Verbal Directed Interaction Skills Do Don’t Ask Forced Choice Questions Ask yes/no questions Offer verbal scripts of what to say “Mind read” Find a Plan B to get a response Allow avoidance of speaking Encourage appropriate volume Encourage whispering Direct questions and expectations for speaking Indirect questions Wait 5 -7 seconds for responses Moving on quickly Patience Seeming anxious/stressed also

Teacher Question Verbal Response Non-verbal Response Labeled Praise Wait 5 sec, repeat question Wait 5 sec, probe for verbal Verbal response No response or nonverbal Labeled praise Wait 5 sec, reduce expectations

Time to practice!

Shaping • Slowly increasing to full speech from current ability level Spontaneous Initiation Scripted Initiation Full sentence responding 2 -3 word responding 1 word responding Yes/no responding Sound combinations Letter sounds

Setting Appropriate Goals/ Shaping Highest goals Greetings, social niceties, specials’ classes, performances, etc. Large group Full class speaking, raising hand/initiating, presentations Small group Reading group, speech at assigned table, social skills group, lunch bunch 1: 1 speech Parents to assist child in speaking to teacher or interventionist, introduce new adults or new peers 1 by 1

Stimulus Fading • Gradually increasing the number of different people the child speaks to and settings the child speaks in Gradually introducing new people into conversations • Speaking in new settings with the help of stimulus associated with speaking (e. g. , communication ladders with speaking partner or keyworker) • https: //drive. google. com/file/d/0 B 0 FTys. H_x-MPX 1 Nra. Ets. WVl. Mak. E/view? ts=58 ab 611 f Can fade in: Adults Peers Groups

Time to practice!

Video Self-Modeling • Researched as stand alone intervention, whereas many other CBT techniques have been researched in a package. • Behavioral procedure wherein video splicing is used to create a recording of child with SM “talking” to a teacher or another person in the school • Shows child what it would be like to speak to the NCP • Can be discrete words spliced together to create full sentences. • Can be whole sentences spliced together to replicate a conversation

Predictors of Treatment Effectiveness • Age • Severity • Parent involvement • School involvement • Professional involvement

School-based Supports: 504 Accommodation Plan • Extra time to answer questions, during instruction and on • Seat assignment next to comfortable peer; away from assessments door; back of the classroom Student should be included in all classroom activities; • Assigned schedule times for bathroom breaks participation should be encouraged (e. g. , assigning nonverbal jobs/responsibilities such as cleanup, line leader) • Parents/student notified of changes in routine and/or special large group activities (e. g. , substitutes, fire drills, • Access to small-group instruction schedule changes, field trips) • • Access to small-group test taking • Extended time on tests • Allow student and parents to access school environment outside school hours (e. g. , arrive early, stay late, summer hours if possible) Alternative methods for oral assignments (e. g. , 1: 1 setting, • Opportunity to meet teacher prior to school year pre-recorded video) • Participation in social skills group • Access to nonverbal assessments when possible • • Opportunities for exposure-based practice, 3 -5 x per week for 15 -30 minute sessions with a key worker • Home-school communication provided daily/weekly

School-based Supports: Individualized Education Plan • A student may qualify for an IEP under the category of • Other Health Impairment (OHI) • *would require diagnosis of SM from a medical professional (MD or DO) Speech & Language Impairment (SLI) • Emotional Impairment (EI) • • An IEP may include the aforementioned accommodations, as well as direct/consultation service time with a special education provider (e. g. , SLP, SSW)

How to decide between a 504 vs. IEP? • Does child require accommodations and/or specialized instruction? • Most important component of school-based support is providing opportunities for brave work within the school setting • • In your district, which document will guarantee the student opportunities to work with a keyworker? Also consider additional services/supports student may need: Academic supports? • Speech and Language supports? • Social skill supports? •
 are")
Brave Work in the Schools • Brave work (i. e. , exposurebased practices) are facilitated by a key worker • Any adult who consistently has time to work with the student • e. g. , Paraprofessional, classroom assistant, interventionist, special education team member, specials teacher, custodian • Having 1 person serve as a key worker is ideal • Remember, only change 1 variable at a time Setting Practice Ideas • • 1: 1 Small Group Large Group • Responding to, and initiating speech, in context of a game with key worker Maintaining speech across settings (e. g. , lunch room, play ground, walking down the hall) Initiating/responding with NCP (e. g. , lunch aide, bus driver, office secretary, paraprofessional, specials teacher) • • • Playing game with peers Participating in an academic- or social skills intervention group Participating in small group lesson within the classroom, facilitated by teacher • • • Sharing idea in front of the whole class Raising hand asking a question Giving a presentation

Take-Home Points • Children aren’t mute because they WON’T speak but because they CAN’T speak. • Early behavioral intervention is key. • Treatment can be VERY effective in treating Selective Mutism. • A team approach to treatment is essential.

Questions?
- Slides: 37