Beta lactam antibiotics These are antibiotics having a

Beta lactam antibiotics

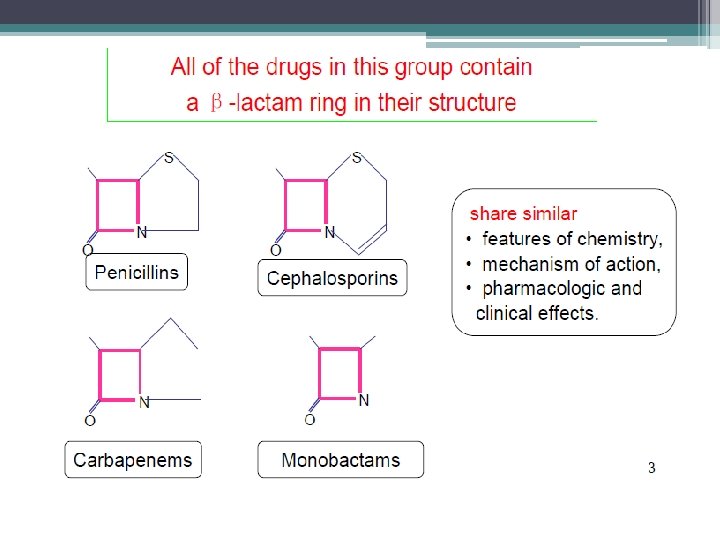
• These are antibiotics having a Beta-lactam ring. • The two major groups are penicillins and cephalosporins. • Monobactams and carbapenems are relatively newer additions.

BETA LACTAM CHARACTERISTICS • Same Mechanism of Action : Inhibit cell wall synthesis • Bactericidal (except against Enterococcus sp. ); time-dependent killers • Short elimination half-life • Primarily renally eliminated • Cross-allergenicity - except AZTREONAM

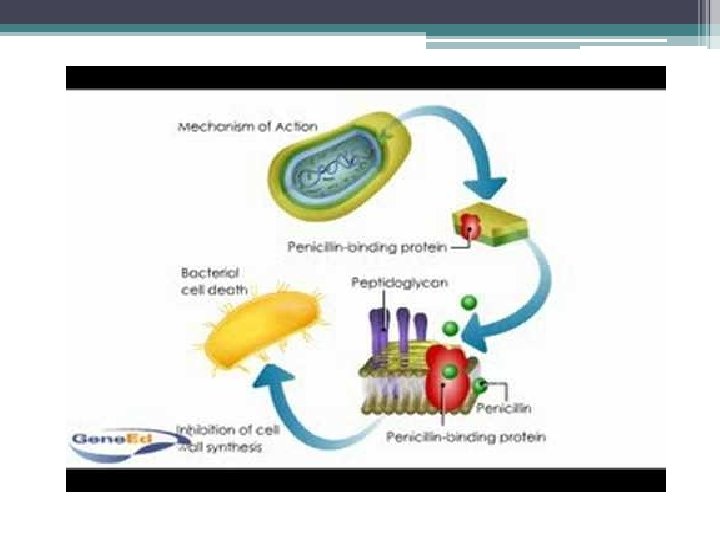
q. MECHANISM OF ACTION • Interfere with cell wall synthesis by binding to penicillin-binding proteins (PBPs) which are located in bacterial cell walls • Inhibition of PBPs leads to inhibition of peptidoglycan synthesis→ Cell death

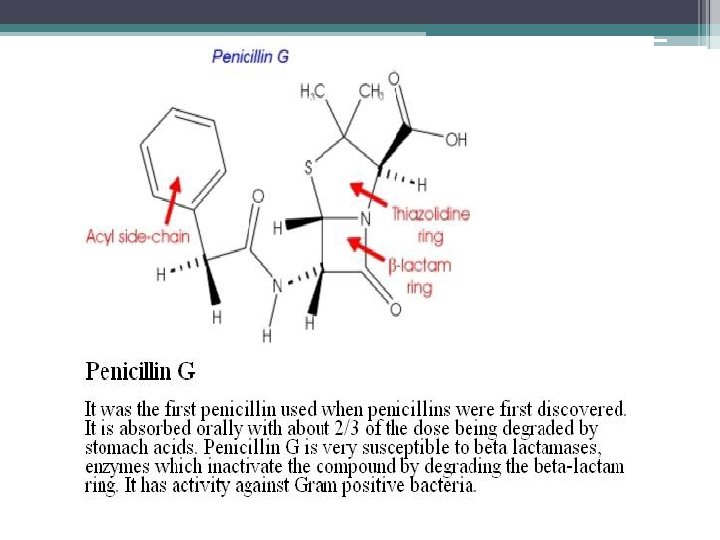
PENICILLINS • Penicillin was the first antibiotic to be used clinically in 1941. It is a miracle that the least toxic drug of its kind was the first to be discovered. • It was originally obtained from the fungus Penicillium notattum, but the present source is a high yielding mutant of P. chrysogenum

q Alexander Fleming discovered penicillin in 1928 q Alexander Fleming isolated the antibiotic substance penicillin from the fungus Penicillium notatum on September 15, for which he shared a Nobel Prize in 1945. q Penicillin is a antibiotic used in the treatment of bacterial infections caused by susceptible organisms

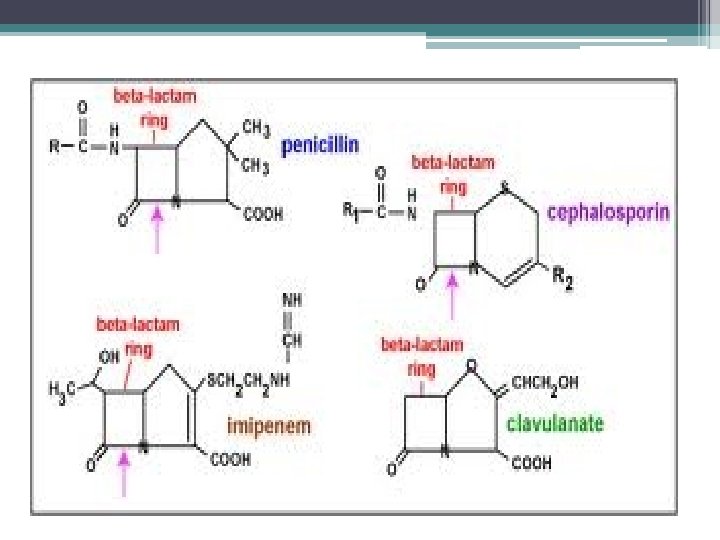
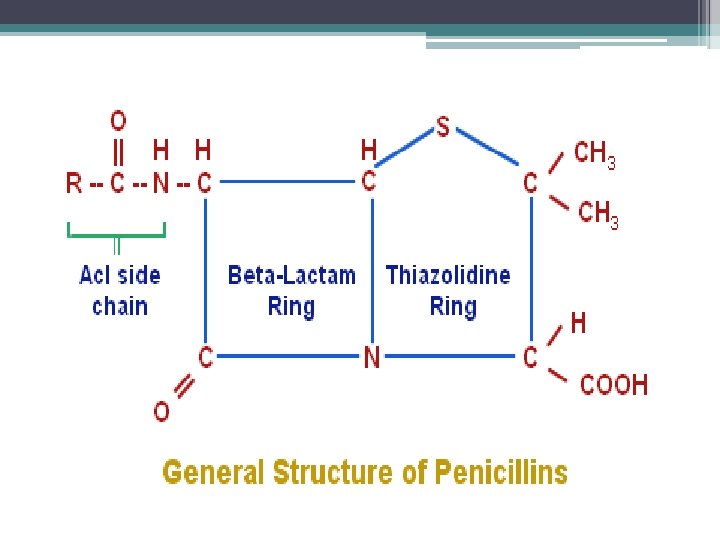
• The structure of the penicillins consists of a thiazolidine ring connected to a beta-lactam ring, which is attached to a side chain. • All penicillins are derived from 6 Aminopenicillanic acid. • The various penicillins differ in their side chain structure

• Penicillins are divided into natural and semisynthetic one (antistaphylococcal, extendedspectrum penicillins et. al) • Natural penicillins: extracted from the cultural solution of penicillia. • • Prototype is penicillin G Is p. H sensitive. Therefore not given orally. Effective against Gram-positive cells Susceptible to penicillinase

 a. Acid stable penicillin-V/phenoxymethyl")
CLASSIFICATION q. Narrow spectrum penicillins 1. Beta lactamase sensitive(natural penicillins) a. Acid stable penicillin-V/phenoxymethyl penicillin (oral) b. Acid labile penicillin-G/benzyl penicillin (I. M, I. V), procaine penicillin –G (I. M, depot), benzathine penicillin-G (I. M, depot) 2. Beta lactamase resistant (antistaphylococcal) a. Acid stable cloxacillin (oral, I. M), dicloxacillin (oral, I. M), flucloxacillin (oral, I. M) b. Acid labile methicillin (I. M, I. V), nafcillin (I. M, I. V)
 1. Acid stable (aminopenicillins)")
q. Extended spectrum Pns (all are sensitive to beta-lactamase degradation) 1. Acid stable (aminopenicillins) ampicillin (oral/parenteral), bacampicillin (oral/parental), talampicillin (oral/parenteral), amoxycillin (oral/parenteral) 2. Acid labile (antipseudomonal Pns) carbenicillin, ticarcillin, piperacillin, mezlocillin, azlocillin (all parenteral)

ACID STABLE- PENICILLIN V • The oral form of penicillins • Indicated only in minor infections because of their relatively poor B/A, weaker antimicrobial activity, the need for dosing many times • NARROW ANTIMICROBIAL SPECTRUM.

ACID LABILE-PENICILLIN G • It is relatively unstable in acid, thus the B/A is low. • Suitable for I/M or I/V admn. • A single 6 Lac unit I/M dose of procaine Pn yields clinically effective concentrations for 12 -24 hrs DOC- syphilis, neurosyphilis

• Single I/M dose of 1. 2 million units of benzathine Pn-G can provide plasma levels which are sufficient to protect against beta-haemolytic streptococcal infection for 3 weeks( longest acting)
, unless inflammation (meningitis) is")
• There is poor penetration into the cerebrospinal (CSF), unless inflammation (meningitis) is present. • Pn-G is excreted by the kidneys, its elimination occurs via tubular secretion while only 10% is excreted by glomerular filtration • Probenicid blocks tubular secretion of Pn
,")
SPECTRUM OF ACTIVITY & USES q. Gm +ve cocci: strep pyogenes (pharyngitis, otitis media), strep pneumoniae, strep viridanss & strep faecalis i. e. , enterococcus (SABE) • Simultaneous administration with gentamicin to treat enterococcal endocarditis • Single injection of benzathine Pn-G is satisfactory for treating rheumatic fever as it prevents colonisation of beta haemolytic streptococci
, gas gangrene (C perfringes),")
q. Gm +ve bacilli: • DOC for tetanus (C tetani), gas gangrene (C perfringes), diphtheria (C diphtheriae), anthrax (Bacillus anthraecis), meningitis (l monocytogenes) • Spirochetes like T Pallidum (syphilis) are highly sensitive. Benzathine Pn-G (2. 4 MU I. M once a wk for 2 -3 weeks)
")
q. Pn-G is moderately active against gm –ve cocci such as N meningitidis (menigitis) & N gonorrhoeae (gonorrhoea) qalso active against Actinomycetes like actinomyces israelii (cranio -facial/thoracic/abdominal abscess)
 • Methicillin")
ANTISTAPHYLOCCAL PENICILLINS • Narrow spectrum, beta lactamase resistant (cloxacillin, dicloxacillin, methicillin, nafcillin) • Methicillin is no longer used because of nephrotoxicity. Nafcillin is preferred for parenteral use while cloxacillin & dicloxacillin can be given orally

• Osteomyelitis, septicaemia, endocarditis & cellulitis c/b susceptible strains of staphylococci • Cloxacillin in addition can also be used to treat mild staphylococcal skin infection such as impetigo
 • Both have adequate oral B/A, ingestion of")
BROAD SPECTRUM PENICILLINS Ampicillin and amoxycillin(aminopenicillins) • Both have adequate oral B/A, ingestion of food decreases the B/A of ampicillin so must be administered 1 hr before or after meals Bacampicillin & talampicillin are prodrugs of ampicillin, disturb intestinal flora to much lesser extent

• They are similar to penicillin G in the activity against gram-positive organisms but are weaker than the latter. • They are more satisfactory for the treatment of enterococci and streptococcus viridians

• They are similar to chloramphenicol in the activity against gram-negative organisms (B pertusis, H Inflenza, E coli, S typhi, P mirabilis & Shigella) • Amoxycillin is also used in multidrug regimens for eradication of H pylori in duodenal & gastric ulcers

• Ampi & amox are also very effective against strep viridans & enterococci (SABE) & pneumococci • For SABE, ampicillin 2 g I. V every 6 hrs may be used in place of Pn-G • Ampicillin is also effective in meningitis c/b L monocytogenes

• They are acid-resistant but are not penicillase-resistant. • P. aeruginosa are fail to respond to these drugs.
 • ureidopenicillins (piperacillin, mezlocillin, azlocillin) are acid")
ANTIPSEUDOMONAL PENICILLINS • Carboxypenicillins (carbenicillin & ticarcillin) • ureidopenicillins (piperacillin, mezlocillin, azlocillin) are acid labile

• Piperacillin have comparable spectra of activity against many gm +ve & gm –ve organisms, special feature is their activity against P aeruginose & indole +ve Proteus which are not inhibited by Pn-G or aminopenicillins

• Used for serious infections due to pseudomonas, proteus, klebsiella as in burns, septicaemia, UTI & in immunocompromised patients. • Generally used in combination with an aminoglycoside (gentamicin) for pseudomonal infections.

BETA LACTAMASE INHIBITORS • Resemble b-lactam antibiotics only structurally but do not possess any significant antimicrobial action • They bind irreversibly to the catalytic site of susceptible b-lactamases (produced by bacteria) to prevent hydrolysis of Pns (SUICIDE INHIBITORS) • They can inhibit plasmid mediated blactamases which are responsible for transferred drug resistance
, SULBACTAM (semisynthetic) & TAZOBACTAM (structural analogue")
• CLAVULANIC ACID (derived from streptomyces clavligerus), SULBACTAM (semisynthetic) & TAZOBACTAM (structural analogue of sulbactam)

• Only clavulanic acid is orally absorbed, others are used parenterally • They are available in FDC • clavulanic acid is combined with amoxycillin • sulbactam with ampicillin • tazobactam with piperacillin

• Addition of clavulanic acid with amoxycillin extends the antimicrobial spectrum of amoxycillin against b-lactamase producing bacteria like strep pneumoniae, H influenzae & moraxella (otitis media, sinusitis, RTIs), methicillin sensitive staph aureus, K pneumoniae (nosocomial Pneumoniae), penicillinase producing N gonorrhoae, blactamase producing anaerobes, E coli, Proteus

• Amoxycillin 250/500 mg + clavulanic acid 125 mg tablets/capsules

• Ampicillin 1 g + sulbactam 0. 5 g; I. V/I. M • Piperacillin 2 g + tazobactam 0. 25 g; I. V/I. M • Adverse effects are rare except GI intolerance, stomatitis & rashes

RESISTANCE TO PENICILLINS 1. production of β-lactamase enzymes • most important and most common • hydrolyzes beta-lactam ring causing inactivation 2. Trapping mechanism. • Some b -lactams tightly bind with b lactamase and stay outside the bacterial cell. Thus, these beta-lactams can’t enter the bacterial cell wall to combine with the PBPs.

3. Modification of target PBPs. • responsible for methicillin resistance in staphylococci and penicillin resistance in pneumococci. 4. Impaired penetration of drug to target PBPs. • which occurs only in Gm -ve species, is due to impermeability of the outer membrane that is present in Gm -ve but not in Gm +ve bacteria.

5. The shortage of autolytic enzyme. • Under this circumstance, the beta-lactams have normal inhibiting action, but their kill effects are very poor. 6. The presence of an efflux pump. • Some organisms also may transport betalactam antibiotics from the periplasm back across the cell wall via an efflux pump

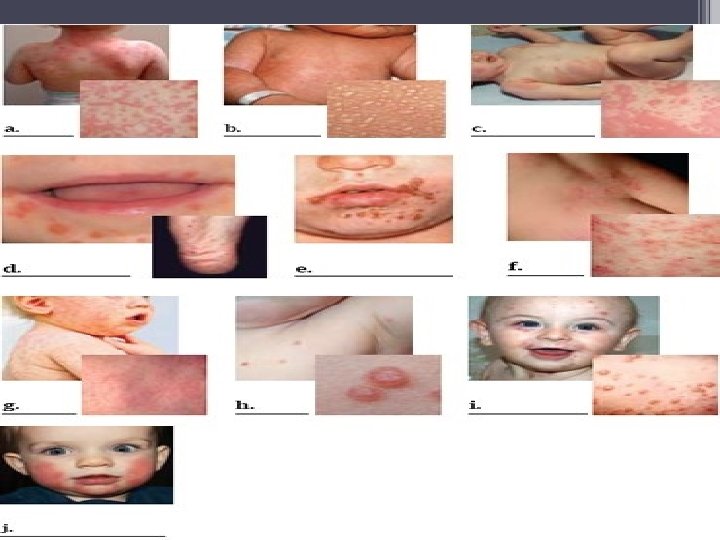
ADVERSE EFFECTS 1. Hypersensitivity reactions – 5 to 20 % q Immediate HS reactions – m/c & occur within 20 min of parenteral administration • Urticaria, pruritis, wheezing, sneezing, rhinitis – may pass over to anaphylaxis c/b diffused pruritis, hypotensive shock, angioneurotic edema, choking, l/o of consciousness & death • Adrenaline (s/c or i/m), corticosteroids (i/v or i/m), antihistamines (i/m), O 2 inhalation, i/v fluids or plasma expanders

q. Accelerated HS reactions usually occur within 72 hrs • Rash, fever, urticaria but rarely angioneurotic edema, fatality is extremely rare q. Late HS reactions occur after 72 hrs • Morbiliform, urticarial or erythematous eruptions, local inflammatory reactions, lymphadenopathy, splenomegaly, serum sickness

2. GASTROINTESTINAL diarrhoea is more common with ampicillin, glossitis, stomatitis, abnormal taste sensation

3. NEPHROTOXICITY, is very rare. 4. SUPERINFECTIONS, results from alterations in intestinal flora. A higher incidence occurs with broad-spectrum penicillins. 5. Pn injected in a syphilitic patient may produce Jarisch-Herxheier reaction c/b fever, myalgia & even collapse d/t sudden release of spirochaetal breakdown products which may last upto 72 hrs

DRUG INTERACTIONS q. ANTAGONISTIC COMBINATIONS • Oral Pns may be antagonised by bacteriostatic antibiotics (tetra, chloram, erythro) as they will diminish bactericidal effect of Pns by inhibiting the bacterial growth • Pns & AG’s should not be mixed in same syringe as they inactivate each other • Ampicillin with allopurinol may cause non-urticarial maculopapular rash • Hydrocortisone inactivates ampicillin if mixed in the I/V fluid

q. SYNERGISTIC COMBINATIONS • Probenecid prolongs the action of Pn by decreasing its tubular secretion • Procaine Pn-G with gentamicin against strep viridans, strep faecalis in SABE • Piperacillin & gentamicin against Pseudomonas & proteus • FDC of ampicillin/amoxycillin with cloxacillin in postoperative & respiratory infections.
- Slides: 49