Beta blockers and anesthesia Dr S Parthasarathy MD
,")
Beta blockers and anesthesia Dr. S. Parthasarathy MD. , DA. , DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics Ph. D ( physiology) – IDRA, FICA

Mainly non cardiac surgeries

What are they ? • Preferentially blocks beta receptors of the adrenergic system
: Pindolol. •")
Classify ? • Nonselective blockers. • – With ISA (Intrinsic sympathetic activity): Pindolol. • – With MSE (Membrane stabilising effect): Propranolol, sotolol, timolol. • – Both ISA and MSE: Alprenolol, oxyprenolol. • – Neither ISA or MSE: Nadolol. Pro – BBB cross • • Cardioselective blockers. Aten – no • – With ISA: Practolol, acebutolol • – With MSE: Acebutolol • – Neither ISA or MSE: Atenolol, metoprolol, esmolol

Actions !! • Reduce heart rate • Reduce contractility - reduce cardiac output • • Decrease AV nodal conduction Decrease arrythmogenicity - phase IV decrease Reduced rennin angiotensin activity ISA Peripheral vasoconstriction activity ? Bronchospasm Decreased glucagon response to hypoglycemia Decrease IOP

• Carvidolol-- some vasodilation • Nebivolol • nitric oxide potentiation

Indications • • Hypertension Angina Sinus tachycardia and paroxysmal atrial tachycardia Coronary artery disease Dissection aorta Hypertrophic obstructive cardiomyopathy QT–prolongation syndrome Cyanotic spells in tetralogy of Fallot.

Other indications • • Prophylaxis of migraine Essential tremor Anxiety Alcohol withdrawal syndrome. • Thyrotoxicosis • Glaucoma

Contraindications to beta blockers • • Peripheral arterial disease AV blocks Bronchospasm Frank CCF ! -- Slow start and slow rise • Bradycardia and hypotension and hypoglycemia in fetus – beware

Anesthetic beta blocker • Esmolol is effective in quick control of supraventricular tachyarrhythmias in patients with acute myocardial infarction where it reduces heart rate and myocardial oxygen demand. • It is also used to control perioperative hypertension with tachycardia. • Dose of esmolol 50 to 200 mcg/kg/min. • rapid onset (within 20 seconds) short duration of action (9 to 10 min). • 10 mg / ml – 10 ml vial

• Acts better when sympathetic activity is high !!

When its working ? • • Heart rate around 55 Less than 20 % increase with stress Should not be any AV block Then its working

They don’t do !! • Beta-blockers do not affect the serum electrolytes, particularly serum potassium/serum uric acid levels, • but glucose tolerance deteriorates in some non-insulin dependent diabetics also.

Anesthetic considerations

Premedication • Already on drugs continue • Think of using in hypotensive anesthesia

Anesthetic considerations volatile agents produce more CVS depression

In general anesthesia • • Fentanyl Vecuronium Neostigmine Succinyl choline Bradycardia may be more severe

General anesthesia – concerns. Normal sympathetic response to blood loss, acute hypovolaemia may be obtunded: Simultaneous use of calcium channel blockers cause additive myocardial depression Bradycardia following acute blood loss should be anticipated. Avoid Hypercarbia should be avoided - hypotension because the vasodilatation produced by carbon dioxide is no longer offset by tachycardia due to activation of the adrenergic system

Can we reverse ? ? • Atropine–dose - 2 to 3 mg intravenously. • Isoprenaline–specific antagonist for beta adrenergic blocking drugs. It is given as an infusion with a dose of 2 to 5 mcg/min • Calcium chloride–increases myocardial contractility. Dose: 500 to 100 mg over 10 to 20 min. • Aminophylline– 5 mg/kg/IV, inhibits phosphodiesterase, • Glucagon 5 -10 mg I/V • Cardiac pacing.

Other uses • To abolish hypertensive response to laryngoscopy. • Adjunct to nitroprusside induced hypotension. • Postoperative hypertension in coronary artery bypass graft patients. • For by pass surgery on beating heart. • Supraventricular arrhythmias.

In neuraxial anesthesia • Heart rate fall and hypotension more • Test dose may not be foolproof • Other causes of tachycardia ruled out – think of beta blockers • Ephedrine – unopposed alpha activity
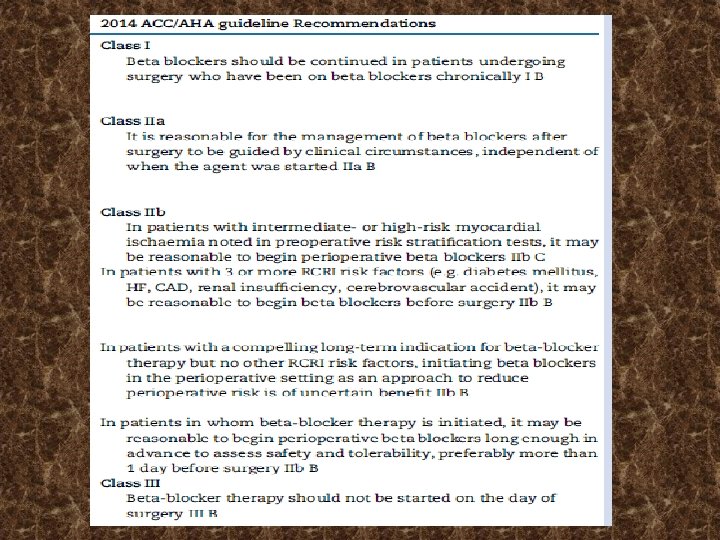
 • showed the benefit of a perioperative β blockade")
POISE (Peri Operative ISchemic Evaluation) • showed the benefit of a perioperative β blockade in terms of reduction in cardiovascular death and MI, but with an increased risk of stroke and total mortality. • 1 week prior to surgery – important • Postop continue

Summary • • What drugs Classification Effects Uses Contraindications General anesthesia Regional POISE trial
- Slides: 24