BENIGN PROSTATIC HYPERPLASIA BPH Dr AMMAR FADIL BPH

BENIGN PROSTATIC HYPERPLASIA BPH Dr. AMMAR FADIL

• BPH is defined by – by an increased number of epithelial & stromal cells in the transition zones and periurethral area of the prostate and thus correctly referred to as hyperplasia and not hypertrophy • Is a common cause of lower urinary tract symptoms (LUTS)- (older term prostatism )in men 2

PROSTATE ZONES • Transitional zone, surrounds upper urethra, sphincter 5% of prostate glandular elements, site of BPH • Peripheral zone, 70% of prostate glandular elements, site of prostatic CA • Central zone 25% of prostate glandular elements; surrounds ejaculatory ducts 3

4

BPH • BPH is the most common benign disease in older men • The prevalence of BPH is related to age – 8 % in men 50 s – 90 % in men older than 80 years • BPH is a progressive disease characterized by prostate enlargement, which might subsequently determine the onset of lower urinary symptoms (LUTS). 5

• Histologic changes of prostatic enlargement are evident in 50% of men by the age of 60 y, Although not all patients have “luts” • half of men with prostatic enlargement develop LUTS • Norm Prostate size 20 gMLcubic CM 4. 4 x 3. 4 x 2. 6 cm (W x l x A-P) • Prostatic functions: – sperm nutrition – seminal anticoagulation 6

• prostate classification is often referred to the “ 3 lobes” of the prostate, namely, the median and the 2 lateral lobes 7
 Increase of prostatic cell number is")
Etiology of BPH 1. aging (decreased apoptotic activity) Increase of prostatic cell number is related to an imbalance in cell proliferation & cell death (apoptosis) 2. Hormonal imbalance Prostate is mainly composed by androgen dependent tissue, Serum testosterone levels decrease gradually with aging ; oestrogen remains constant. Increasing estrogen –to –androgen ratios According to this theory, the prostate enlargement because of increased estrogenic effects 3. Recently, the role of Chronic inflammation 8

pathology • BPH is characterized by an increased number of epithelial & stromal cells in the transition zones and periurethral area of the prostate. The main hormone acting on the prostate is Testosterone, which is secreted by the Leydig cells of the testes Testosterone is converted to DHT by the enzyme 5 a-reductase , which is found in high concentration in prostate. DHT has five times the potency of testosterone Castration results in the regression of established BPH and improvement in urinary symptoms. 9

Pathology As BPH nodules in the transition zone enlarge, they compress the outer zones of the prostate, resulting in the formation of a surgical capsule. • This boundary separates the transition zone from the peripheral zone and serves as a cleavage plane for open enucleation of the prostate during open simple prostatectomies 10

Pathophysiology • can be subdivided into the static & the dynamic component ü static component Mediated by the volume effect of BPH. intrusion into the urethral lumen leading to a (bladder outlet obstruction) BOO and LUTS 11

ü The dynamic component • A 1 -adrenoceptor-mediated prostatic smooth muscle contraction. • Smooth muscle accounts for 40% of the hyperplastic prostate. • This effect is the rationale for A-adrenoceptor blocker treatment for symptomatic BPH. 12

Effects of BPH ON Bladder. • BOO causes thickening of the wall of the bladder, the musculature of the bladder hypertrophies to overcome the obstruction and called trabeculae (cystoscopy). If left untreated, mucosal herniation between detrusor muscle bundles ensues, causing diverticula formation • Significant BPH is associated with increased blood flow, and the resultant veins at the base of the bladder are liable to rupture to cause haematuria 13

Cystogram cystoscopy 14
 2. Lower urinary tract symptoms (LUTS)")
Presentation and Symptoms 1. No symptoms (silent prostate) 2. Lower urinary tract symptoms (LUTS) These have been subdivided into irritative (storage) & obstructive (voiding) symptoms. Irritative symptoms have the most impact on the patient's quality of life. 3. Urine retention acute or chronic 4. Hematuria 5. UTI 6. vesical stone 7. bilateral hydronephrosis and renal failure 15

Lower urinary tract symptoms LUTS • storage 1. nocturia; 2. frequency; 3. urgency (urge incontinence) • voiding 1. weak stream 2. Intermittent stream – stops and starts; 3. Straining 4. sensation of incomplete bladder emptying; Hesitancy terminal dribbling 16

Acute urine retention AUR as a painful, palpable, or percussible bladder when the patient is unable to pass any urine. Patients are typically catheterized and then undergo a trial without catheter (TWOC) when ? while taking an α -blocker • A successful TWOC with an α-blocker reduces the chance of needing prostate surgery. • If the trial of voiding fails, the patient should be considered for surgical intervention 17

Assessment of Symptoms • To quantitate the severity of symptoms, a symptom-scoring system is used called : • International Prostate Symptom Score (IPSS) or AUA Symptom Score • The IPSS is an 8 -question tool (7 symptom questions + 1 quality of life question) designed to be completed by the patients We ask patients to quantify the severity of their complaints on a scale of 0– 5. Thus, the score can range from 0 to 35. A symptom score of 0– 7 is mild, 8– 19 is moderate , & 20– 35 is severe The IPSS assessment should include an assessment of quality of life, which is a reflection of the degree of ‘bother’ caused by a patient’s symptoms 18

19

Sign DRE are performed on all patients. DRE: The size & consistency of the prostate & to assess anal tone, faecal impaction. BPH usually is a smooth, firm, elastic enlargement of the prostate CA stony hard 20

21

Investigations of men with BPHLUTS Essential investigations 1. A urinalysis to exclude infection or hematuria 2. Renal function tests S. Creatinine & B. urea (renal insufficiency may be observed in 10% of BPH) 3. Prostatic specific antigen (PSA) 4. Ultrasound assess prostatic size, PVR, kidneys 5. Urinary flow rate (flowmetry) ADDITIONAL TESTS – urodynamic study are reserved for patients with suspected neurologic disease 22

US 23

Flowmetry • The simplest & most useful test in the assessment LUTS • Normal Q max 20 -25 ml/s in men < 10 ml s indicate obstruction 24

Differential Diagnosis • Urethral stricture, • Ca. P (may be detected by abnormalities on the DRE or an elevated PSA) • Neurologic disease, stroke, diabetes mellitus 25
 alpha blocker b) 5")
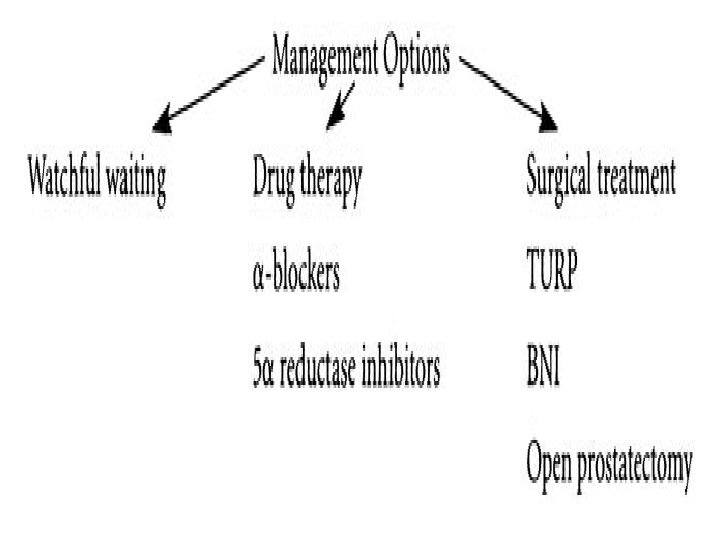
Modality of therapy 1. watchful waiting 2. Pharmacological therapy a) alpha blocker b) 5 alpha reductase inhibitor c) combination therapy d) 5 PDI 3. phytotherapy 4. Surgery TURP, TUIP, HOLEP, OPEN surgery 26

1. Conservative treatment= Watchful waiting Is suitable in men with mild symptoms It includes education, re-assurance • Fluid restriction especially before bedtime • Avoidance of caffeinated beverages • Avoidance of some drugs (e. g. , diuretics) • treatment of constipation 27

2. Pharmacological management A. α-ADRENERGIC BLOCKERS α blocking agents inhibit the contraction of smooth muscle that is found in the prostate. causes an improvement in flow rates and symptom scores • SE: dizziness , orthostatic hypotension & retrograde ejaculation 28

B. 5α –reductase inhibitors – which inhibit the conversion of testosterone to DHT, the most active form of androgen in prostate. – causes a reduction in prostatic volume up to 20 % over 6 months. – It is only appropriate in larger prostates (>40 g) • SE: sexual problems (e. g. , loss of libido) 29

Alpha-blockers – Doxazosin – Alfuzosin 10 mg – Tamsulosin 0. 4 mg – Recently silodosin 5 -alpha-reductase inhibitors – Finasteride 5 mg – Dutasteride 0. 5 mg 30

C. Combination alpha-blocker and 5 -alphareductase inhibitor therapy – Both groups of drugs are effective; however, αblockers work more quickly D. Tadalafil 5 mg is the only Type 5 Phosphodiesterase (PDE 5) inhibitor that is approved for the treatment of BPH related voiding symptoms. 31
")
3. Phytotherapy These agents are derived from plants ü ü African plum (Pygeum africanum) & saw palmetto 32

Indications of surgery • Recurrent or refractory retention (failing at least one attempt at catheter removal) or any of the following clearly related to BPH § severe symptoms not responding to medical therapy • vesical stones • Recurrent UTIs • Recurrent gross hematuria • Dilatation of the upper urinary tract due to BOO, w or wo renal insufficiency 33
")
Surgery • Men should be offered TURP • Men with smaller prostates (<30 g) should be offered transurethral incision of the prostate. TUIP • Open prostatectomy should be offered to men with prostates >80 g only. 34

Counselling men undergoing prostatectomy 1. Retrograde ejaculation This occurs in about 65% of men after prostatectomy. 2. Erectile dysfunction This occurs in about 5% of men 35

Operative treatment 1. TURP Transurethral resection of the prostate TURP is most suitable for prostates < 80 cc. 2. Open prostatectomy – Transvesical prostatectomy – Retropubic prostatectomy (Millin) • When the prostate is too large to be removed endoscopically, an open enucleation is necessary. Prostate glands > 80 g • Open prostatectomy may also be initiated when concomitant bladder stone is present 36

37

38

39
 Laser Advantages")
LASER Therapy Laser Vaporization Enucleation HOLEP ( holmium laser enucleation of prostate) Laser Advantages (1) minimal blood loss (2) ability to treat patients receiving anticoagulation therapy Disadvantages (1) more irritative voiding complaints & (2) High cost 40

LASER 41

Complications of BPH • • • UTI Urine retention Vesical stones, Hematuria , urinary incontinence, upper urinary tract deterioration with renal insufficiency 42

Note • The severity of urinary symptoms do not correlate with prostate size. Small prostates can cause severe symptoms. Large prostates can be asymptomatic 43
- Slides: 44