Benign Breast Lesions NITMED TUTORIALS INC NITMED TUTORIALS

Benign Breast Lesions NITMED TUTORIALS INC © NITMED TUTORIALS

Mock Pretest • This is a picture of a 22 yr old man. • What is the most obvious abnormality? • List 5 causes.

Objectives • To understand the presentation of the different types of benign breast lesions and their management

Outline • • • Introduction Relevant anatomy Classification Differential diagnosis Different types

Introduction • Most common cause of breast problems • Estimated that up to 30% of women will require treatment for a benign breast disorder • Most common symptoms - pain, lumpiness or a lump. • Aim of treatment - exclude cancer - Then treat remaining symptoms.

Anatomy The mature breast lies cushioned in adipose tissue between the subcutaneous fat layer and the superficial pectoral fascia The adult breast lies between the second and sixth ribs and extends from the sternal edge to the midaxillary line. Its size and shape varies from one individual to the next but is characterized by fullness in the lower area and ptosis or drooping, which becomes pronounced with increasing age. FUNCTION – infant feeding

Exclusion of cancer by triple assessment • History and physical examination • Radiological assessment -Ultrasound in patients under 35 years old -Mammography in patients over 35 years old • Pathological assessment -Fine-needle aspiration cytology -Trucut biopsy

Classification • • Congenital abnormalities Breast injuries Breast inflammation ANDI (aberrations of normal development and involution)

Congenital abnormalities Amastia – congenital absence of breast With absence of sternal portion of pectoralis major- Poland syndrome’s syndrome Polymazia – accessory breasts Polythelia Accessory nipple Diffuse hypertrophy – seen in healthy girls around puberty

Diffuse hypertrophy

Breast injuries Haematoma Traumatic fat necrosis -Acute -Chronic Common in Stout middle age women Results in painless lump. Difficult to differentiate from cancer. Biopsy is required Breast transection could occur in RTA from seat belt

Breast inflammation Bacterial mastitis is the most common and is often related to lactation. Staphylococcus aureus is a common organism responsible. Clinical features – signs of acute inflammation. Initially cellulitis, later an abscess (breast abscess) Treatment Early cellulitis phase: antibiotics – flucloxacillin and co-amoxiclav Abscess phase – repeated aspiration under antibiotic cover (currently preferred), - Incision and drainage (artery forceps and finger ensure that loculi are broken, then dependent drain)
 Tuberculosis of the breast: rare, associated with PTB or cervical TB Seen")
Breast inflammation(contd) Tuberculosis of the breast: rare, associated with PTB or cervical TB Seen more in parous women Presents with multiple chronic abscesses and sinuses, attenuated surrounding skin Nodes prominent Diagnosis: bacteriology and histology Treatment : anti-tuberculous drugs(slow)
 of the breast and anterior chest")
Mondor’s disease Thrombophlebitis of the superficial veins (thoracoepigastric) of the breast and anterior chest wall. Appears as thrombosed subcutaneous cord attached to skin. Self limiting.

Duct ectasia/periductal mastitis dilatation of the breast ducts, which is often associated with periductal inflammation. Pathogenesis obscure, more common in smokers Clinical features: Nipple discharge (of any colour), a subareolar mass, abscess, mammary duct fistula and/or nipple retraction Treatment: exclude cancer Antibiotics Surgery: excision of all the major ducts (Hadfield’s operation)

Aberrations of normal development and involution • Due to confusing nomenclature of benign breast disease • Fibrocystic disease, fibroadenosis, chronic mastitis and mastopathy • New system was derived by Cardiff breast clinic

Concept of ANDI • Breast is a dynamic structure that undergoes changes throughout a woman’s reproductive life with superimposed cyclical changes throughout the menstrual cycle • Pathogenesis of ANDI involves disturbances in breast physiology extending from perturbation of normality to well-defined disease processes • Little correlation between the histological appearance of breast tissue and the symptoms.
 • Cyst")
Pathology of ANDI (essentially 4 features which vary in extent and degree) • Cyst formation • Fibrosis: dense white fibrous trabeculae replaces fat and elastic tissue • Hyperplasia: of lining ducts and acini with or without atypia • Papillomatosis: extensive hyperplasia may result in overgrowth in ducts

Major symptoms Painful, often multiple, usually bilateral masses in the breast. Rapid fluctuation in the size of the masses is common. Frequently, pain occurs or increases and size increases during premenstrual phase of cycle. Most common age is 30– 50 years. Rare in postmenopausal women not receiving hormonal replacement

Treatment • • • - Exclude cancer Reassure Use pain chart if unsure if cyclical or non-cyclical. Adequate support Firm bra (day) softer bra (night) Exclude caffeine (controversial) Medication Evening primrose oil (GLA) Better effect in women >40 years Danazol Bromocriptine Tamoxifen LHRH agonist

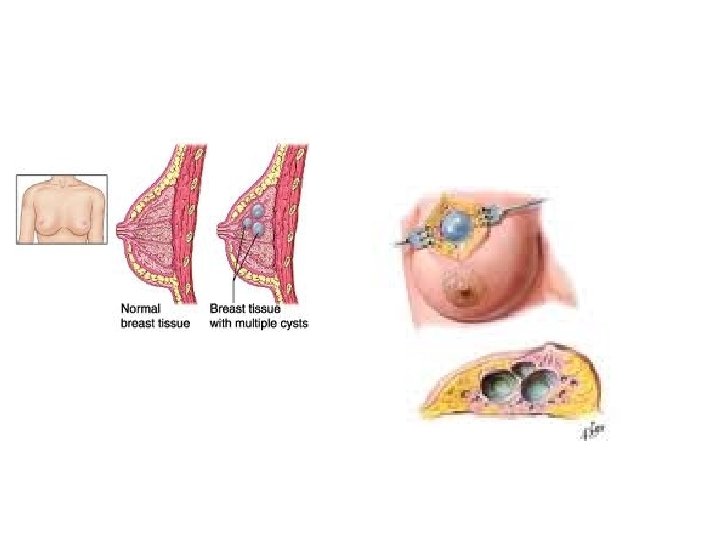
Breast cysts Occur most commonly in last decade of reproductive life Result of a non-integrated involution of stroma and epithelium Often multiple, may be bilateral and can mimic malignancy. Diagnosis can be confirmed by aspiration and/or ultrasound. Typically present suddenly and cause great alarm Prompt diagnosis and drainage provides immediate relief Treatment Aspiration. biopsy if -persistent lump -cyst recurs repeatedly in same area -cyst fluid is blood-stained

Fibroadenoma Most common breast lumps in young women but can occur at any time during the reproductive years Usually arise in fully developed breast between ages 15 and 25 years Arise from hyperplasia of a single lobule and Usually grow up to 2– 3 cm in size. They are surrounded by a well marked capsule and can thus be enucleated through a cosmetically appropriate incision. Fibroadenoma does not require excision unless -associated with suspicious cytology -Becomes very large -patient expressly desires lump to be removed

Giant fibroadenoma >5 cm in diameter often rapidly growing are similar to smaller fibroadenomas can be enucleated through a submammary incision. They are more common in the Afro. Caribbean population. difficult to distinguish from phylloides tumours both clinically and on core biopsy

Phylloides tumour Previously sometimes known as serocystic disease of Brodie or cystosarcoma phylloides, Usually occur in women over the age of 40 years but can appear in younger women Present as a large, sometimes massive, tumour with unevenly bosselated surface. Occasionally, ulceration of overlying skin occurs because of pressure necrosis Despite their size they remain mobile on the chest wall Can recur locally, very rarely develop features of a sarcomatous tumour & may metastasise via the bloodstream Treatment: wide local excision. Massive tumours, recurrent tumours and malignant type: mastectomy

Gynaecomastia? • Presence of breasts in the male resembling those of the mature female • Usually physiological but often needs to be investigated for hormonal causes -Oestrogen or steroid therapy - Liver disease - Pituitary gland tumour - Testicular tumour - Use of spirinolactone • Treatment in severe cases is by excision of breast tissue

Conclusion • A good knowledge of benign breast lesions is important • Triple assessment will exclude cancer • For lumps, likely diagnosis varies with age - Fibroadenomas common in young women - Cysts are common in women aged 30 -50 years - All new lumps in women over 50 years old are cancer until proven otherwise

Bibliography • Dr Ismaila BO, Prof Sule, Dr Adaiah, Dr Balogun • Bailey and Love’s short practice of surgery 25 th ed • Clinical surgery 2 nd ed • Sabiston textbook of Surgery 18 th ed • Principles and practice of surgery including pathology in the tropics 4 th edition
- Slides: 28