Benign breast diseases Dr farhana ACUTE MASTITIS Occur

Benign breast diseases Dr. farhana

ACUTE MASTITIS • Occur during the first month of breastfeeding. • During this time the breast is vulnerable to bacterial infection because of the development of cracks and fissures in the nipples. • From this portal of entry, Staphylococcus aureus or, less commonly, streptococci invade the breast tissue. • The breast is erythematous and painful, and fever is often present

• Morphology. • Staphylococcal infections usually produce a localized area of acute inflammation that may progress to the formation of single or multiple abscesses

PERIDUCTAL MASTITIS • This condition is known by a variety of names, including recurrent subareolar abscess, squamous metaplasia of lactiferous ducts, and Zuska disease. • Women, and sometimes men, present with a painful erythematous subareolar mass that clinically appears to be an infectious process. • More than 90% of the afflicted are smokers.

Morphology • The key histologic feature is keratinizing squamous metaplasia of the nipple ducts. • Keratin shed from these cells plugs the ductal system, causing dilation and eventually rupture of the duct. • An intense chronic and granulomatous inflammatory response develops once keratin spills into the surrounding periductal tissue

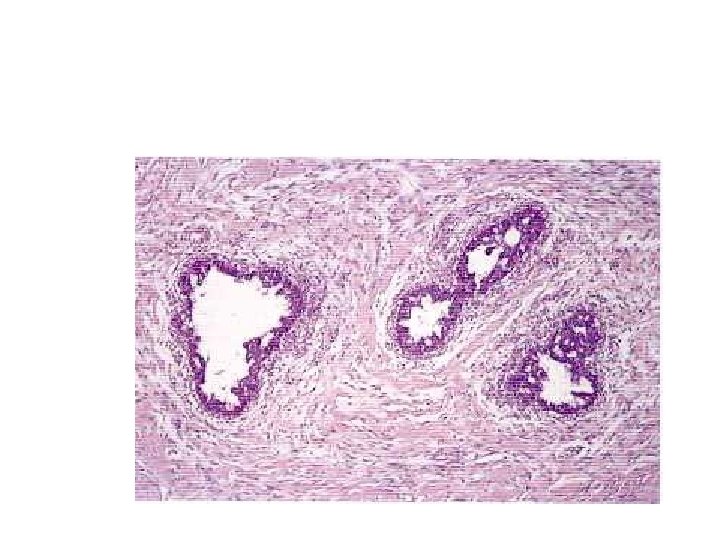
MAMMARY DUCT ECTASIA • This disorder tends to occur in the fifth or sixth decade of life, usually in multiparous women. • Patients present with a poorly defined palpable periareolar mass that is often associated with thick, white nipple secretions and sometimes with skin retraction.

Morphology. • This lesion is characterized chiefly by dilation of ducts, inspissation of breast secretions, and a marked periductal and interstitial chronic granulomatous inflammatory reaction. • The dilated ducts are filled by granular debris that contains numerous lipid-laden macrophages. • The periductal and interductal tissue contains dense infiltrates of lymphocytes and macrophages, and variable numbers of plasma cells

FAT NECROSIS • Fat necrosis can present as a painless palpable mass, skin thickening or retraction, a mammographic density, or mammographic calcifications. • The majority of affected women have a history of breast trauma or prior surgery

• Morphology. • Acute lesions may be hemorrhagic and contain central areas of liquefactive fat necrosis

• • • BENIGN EPITHELIAL LESIONS OF THE BREAST Classification 1. Non proliferative breast changes 2. Proliferative breast changes 3. Atypical hyperplasias

Non proliferative breast changes Syn: Fibrocystic changes • Benign nonproliferative epithelial changes characterized byØ Cystic change Ø Fibrosis Ø Adenosis Ø Occasionally, calcification • Age group- reproductive age group

• Clinical presentationØ Palpable masses Ø Nipple discharge Ø Incidental finding of densities or calcification on mammography

• Morphology • Three main patterns • 1. Cysts– Small cysts- formed due to dilation and unfolding of lobules – Large cysts- formed by coalescence of small cysts – Cyst content- semi translucent, turbid fluid

– Cyst lining- 1. flattened atrophic epithelium – 2. cells with apocrine metaplasiacells with abundant, granular, eosinophilic cytoplasm – 3. papillary projections – 4. calcifications – Unopened cysts are known as blue domed cysts


• 2. Fibrosis • Fibrosis of the adjacent stroma due to rupture of the cyst and leakage of its content • 3. Adenosis • Definition – increase in the number of acini per lobule. • Acini are enlarged and not distorted- blunt duct adenosis

• Lactational adenomasØ Normal appearing breast tissue with physiological adenosis and epithelial lactational changes. Ø Seen in pregnant or lactating women Ø Present as palpable masses Ø Exaggerated focal response to hormones

• Proliferative breast disease without atypia • Proliferation of the ductal epithelium and/or stroma without atypia. • It includesØ Epithelial hyperplasia Ø Sclerosing adenosis Ø Complex sclerosing lesion(radial scar) Ø Papillomas Ø Fibroadenoma with complex features

• Epithelial hyperplasia • Myoepithelial cells and single layer of luminal cells- normal • >2 layer thick- epithelial hyperplasia • >4 layer thick- moderate and florid • Irregular fenestrations in the periphery

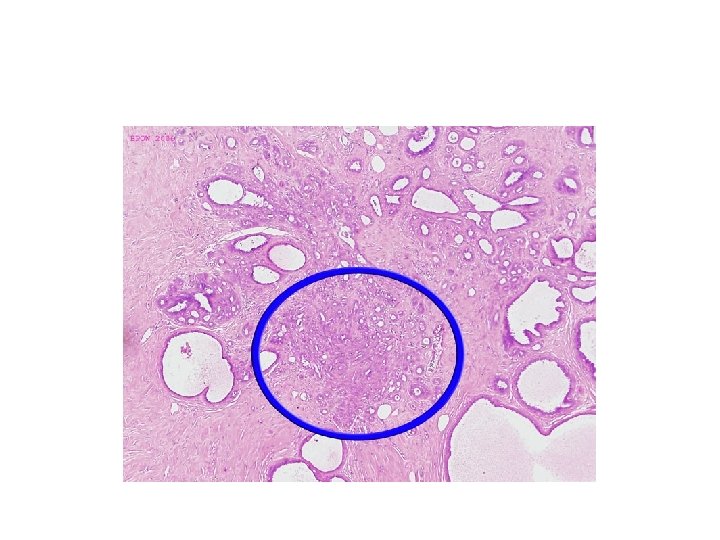
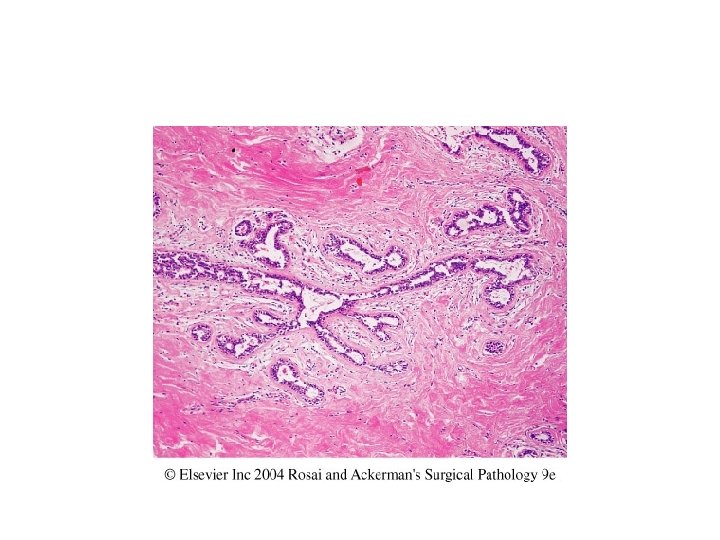
• Sclerosing adenosis ü Increase in the number of acini per terminal duct ü Acini are compressed in the centre and dilated at the periphery • Complex sclerosing lesion(radial scar) • Stellate lesions with central nidus of entrapped glands in a hyalinised stroma

• Papilloma ü Papillae lined by myoepithelial and epithelial cells projecting into the dilated ducts ü Large duct papillomas are solitary and present near the nipple ü Small duct papillomas are multiple and located deeper in the breast tissue

• • Fibroadenoma with complex features Calcifications Cysts>0. 3 cms Papillary apocrine metaplasia

• Proliferative breast disease with atypia • Atypical hyperplasia which resembles ductal carcinoma in situ but lacks sufficient features to diagnose as carcinoma in situ. • Includes • Atypical ductal hyperplasia(ADH) • Atypical lobular hyperplasia(ALH)

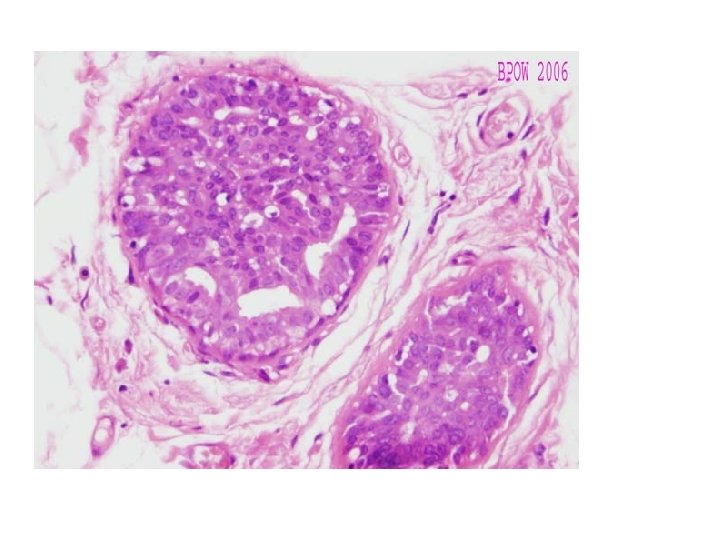
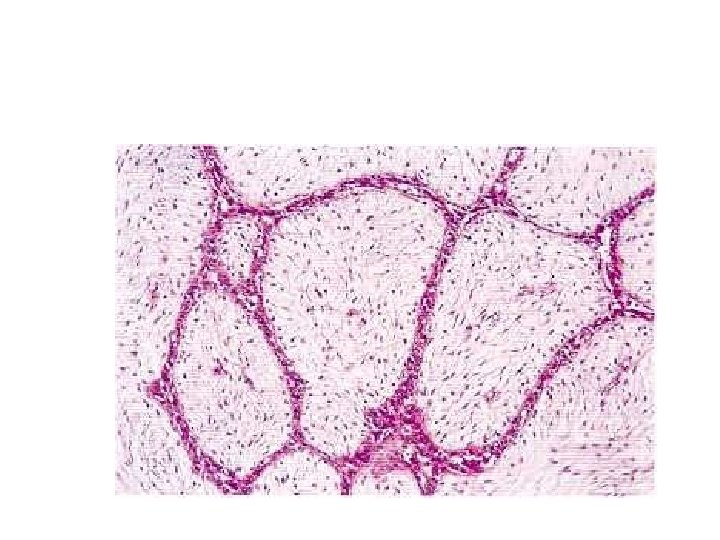
GYNAECOMASTIA • HYPERTROPHY OF MALE BREAST • Unilateral or bilateral enlargement of male breast • Enlargement mainly due to proliferation of ducts and increased periductal stroma

Gynaecomastia occurs in response to hormonal stimulation, mainly estrogen • Pubertal gynaecomastia (13 -17 yrs) • Senescent gynaecomastia (over 50 yrs) • Secondary gynaecomastia In endocrine disease associated with increased oestrogenic or decreased androgenic activity Eg. In hepatic cirrhosis, testicular tumors, pituitary tumors, carcinoma of lung • Idiopathic gynaecomastia

Morphology Gross • One or both male breast enlarged having smooth glistening white tissue Microscopy – 2 main features 1. Proliferation of branching ducts which display epithelial hyperplasia with formation of papillary projections at places 2. Increased fibrous stroma with myxoid appearance

STROMAL TUMORS • The two types of stroma in the breast, intralobular and interlobular, give rise to distinct types of neoplasms. • The breast specific biphasic tumors fibroadenoma and phyllodes tumor arise from intralobular stroma • This specialized stroma may elaborate growth factors for epithelial cells, resulting in the proliferation of the non-neoplastic epithelial component of these tumors.

Fibroadenoma This is the most common benign tumor of the female breast. Most occur in women in their 20 s and 30 s, and they are frequently multiple and bilateral. Young women usually present with a palpable mass and older women with a mammographic density or mammographic calcifications.

• The epithelium of the fibroadenoma is hormonally responsive, and an increase in size due to lactational changes during pregnancy, which may be complicated by infarction and inflammation, can mimic carcinoma. • The stroma often becomes densely hyalinized after menopause and may calcify. • Large lobulated (“popcorn”) calcifications have a characteristic mammographic appearance, but small calcifications may appear clustered and require biopsy to exclude carcinoma

Morphology. • Fibroadenomas grow as spherical nodules that are usually sharply circumscribed and freely movable. • They vary in size from less than 1 cm to large tumors that can replace most of the breast. • The tumors are well-circumscribed, rubbery, grayish white nodules that bulge above the surrounding tissue and often contain slitlike spaces

• The delicate, cellular, and often myxoid stroma resembles normal intralobular stroma. • The epithelium may be surrounded by stroma or compressed and distorted by it. • In older women, the stroma typically becomes densely hyalinized and the epithelium atrophic.

• 1. Intracanalicular type- proliferation of the intralobular stroma compressing the ducts • 2. Pericanalicular type- poliferation of the stroma around cystically dilated glands

• • • Fibroadenoma with complex features Calcifications Cysts>0. 3 cms Papillary apocrine metaplasia Sclerosing adenosis

Juvenile fibroadenoma juvenile fibroadenomas are large and the term is best reserved for those fibroadenomas which occur in adolescents and have a very rapid growth rate. They are well-circumscribed lobulated masses which- may reach 15 -20 cm in diameter, stretching the skin and distorting the nipple. • Juvenile fibroadenomas are entirely benign and do not recur after complete local excision.

• Morphologically, they have an identical structure to the more typical fibroadenoma. The basic pericanalicular and intracanalicular growth patterns are seen but the stroma is likely to be cellular rather than hyalinized • Epithelial proliferation is usually present and often florid.

Phyllodes Tumor • Phyllodes tumors, like fibroadenomas, arise from intralobular stroma. • Although they can occur at any age, most present in the sixth decade, 10 to 20 years later than the peak age for fibroadenomas. • The majority are detected as palpable masses, but a few are found by mammography. • The term cystosarcoma phyllodes is sometimes used for these lesions

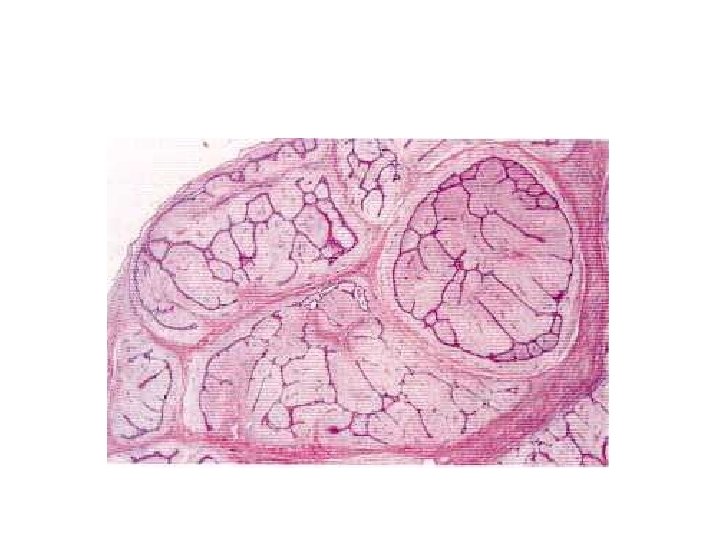
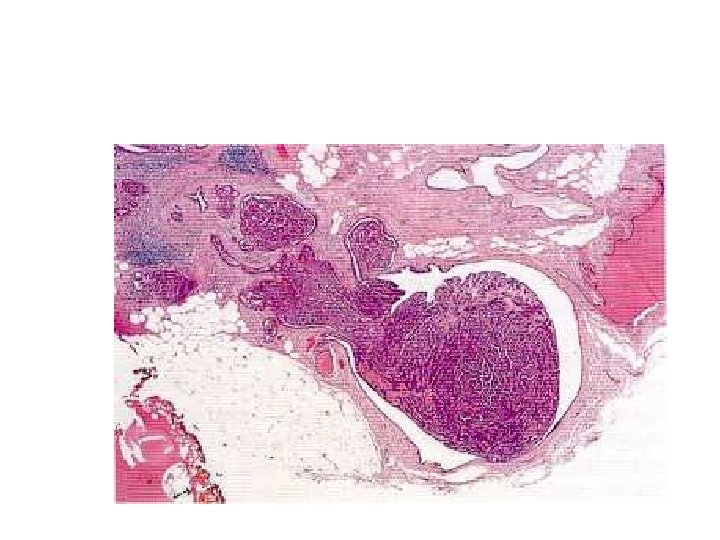
Morphology • The tumors vary in size from a few centimeters to massive lesions involving the entire breast. • The larger lesions often have bulbous protrusions (phyllodes is Greek for “leaflike”) due to the presence of nodules of proliferating stroma covered by epithelium. • In some tumors these protrusions extend into a cystic space. • This growth pattern can also occasionally be seen in larger fibroadenomas and is not an indication of malignancy.

Phyllodes tumor. Large leaf-like structures form clefts lined by epithelial cells. There is an associated cellular stroma

• Phyllodes tumors are distinguished from the more common fibroadenomas on the basis of cellularity, mitotic rate, nuclear pleomorphism, stromal overgrowth, and infiltrative borders. • Low-grade lesions resemble fibroadenomas but are more cellular and contain mitotic figures. • High-grade lesions may be difficult to distinguish from other soft-tissue sarcomas and may have foci of mesenchymal differentiation

• The frequency of chromosomal changes increases with grade and the majority of highgrade lesions are reported to have amplification of EGFR. • Recurrent phyllodes tumors are often of a higher grade than the presenting lesion.

• Phyllodes tumors must be excised with wide margins or by mastectomy to avoid local recurrences. • Axillary lymph node dissection is not indicated, because the incidence of nodal metastases is exceedingly small. • The majority are low-grade tumors that may recur locally but only rarely metastasize. • Rare high-grade lesions behave aggressively, with frequent local recurrences and distant hematogenous metastases in about one third of cases.

Duct Papilloma • Papillomas are true benign neoplasms of the ductal epithelium of the breast. They occur predominantly in women between- the ages of 35 and 55 years. Most patients present with single duct nipple discharge, which is often bloodstained, while in a minority there may be a palpable mass, usually close to the areola

• Duct papillomas can be divided into two main subgroups • central lesions which arise from the main ducts and are usually single, • and peripheral lesions which are associated with terminal duct lobular units and are multiple.

• Macroscopic appearances • Duct papillomas measure less than 2 -3 mm in diameter and are therefore difficult to visualize with the naked eye. • The site of a papilloma within a dilated duct may be indicated by adjacent amorphous debris, including blood clot, but in mostcases the pathologist receives a specimen of fibro-fatty tissue in which there is no discernible gross abnormality

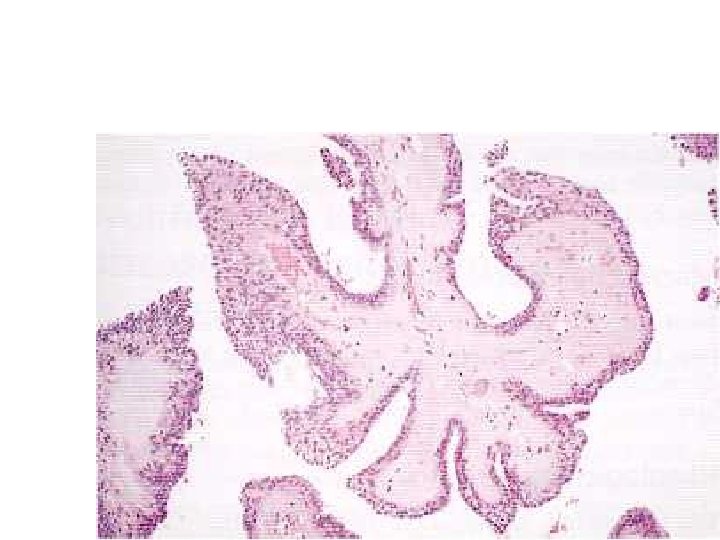
• Microscopically, papillomas consist of a fronded fibrovascular core attached by a stalk to the duct wall. • Multiple fronds from the same lesion may extend into several adjacent duct spaces. Occasionally the base may be sessile. • The fronds are covered by two types of epithelium , an outer cuboidal or columnar secretory cell layer and an inner, myoepithelial cell layer.
- Slides: 53