Benign Bone Tumours Normal Anatomy diaphysis cortex metaphysi

Benign Bone Tumours

Normal Anatomy diaphysis cortex metaphysi s physeal physis scar epiphysis medullar y space METAPHYSIS childhood adult

Benign Bone Tumours l osteoid osteoma l osteochondroma l enchondroma

Clinical Presentation Asymptomatic l Pain l Swelling l Neurological symptoms l Pathological fracture l Incidental finding l

OSTEOID OSTEOMA • Small, benign, solitary painful lesion seen mainly in children & adolescents. • Any bone, tibia & femur…. . 50% Spine Painful Scoliosis

OSTEIOD OSTEOMA • Pain is the commonest presentation. • Pain is worsened by night, typically relieved by salicylates.

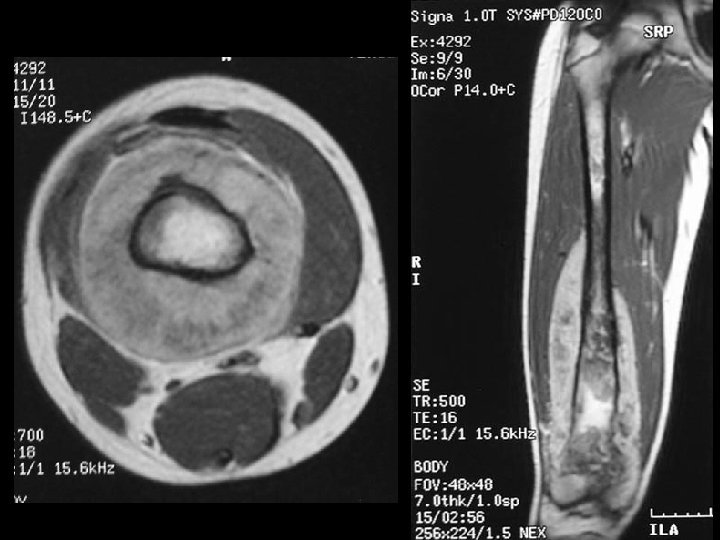
Example 8: 45 y/o with thigh pain

Example 8

 Pedunculated")
Osteochondroma (Exostosis) Pedunculated

OSTEOCHONDROMA • May be solitary or multiple. • Multiple…. . Diaphyseal aclasis. • ? ? Developmental abnormality of the metaphyseal area.

Osteochondroma:

Osteochondroma:

Osteochondroma Chondrosarcoma

Malignant transformation Usually occurs above the age of 40 years. Sudden increase in size. Swelling becomes painful.



ENCHONDROMA • Benign tumour of cartilage originating within the medullary cavity. • Common in the small bones of the hands and feet. • Common presentation: Mass or a Pathological fracture.

Ollier’s Disease: Multiple enchondromata.

Example 11

Benign Bone Tumours chondromata

Tumour Like Conditions of Bone l Simulate bone tumours l Benign tumours are common l The most common malignant bone tumours are secondary metastasis

Aneurysmal bone cyst • At any age • Can affect any bone • Metaphysis • Osteolytic lesion, trabeculated • Eccentric • Aneurysmal? ?


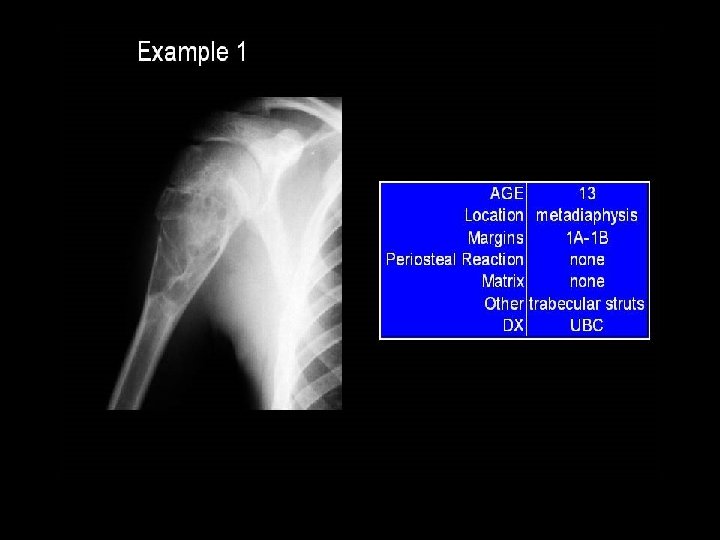
Simple bone cyst • Unicameral bone cyst • Metaphysis of long bones (humerus , femur) • Centric • Filled with straw-coloured fluid

• Bone Cyst – A wall of fibrous tissue filled with clear fluid • Clinical presentation • Pain • Not diagnosed unless a pathological fracture occurs.

Bone Cysts simple bone cyst l fibrous dysplasia l aneurysmal bone cyst l

Imaging of Bone Tumours Solitary or multiple lesions? l What type of bone is involved? l Which part of the bone is involved? Are the margins of the lesion well defined? l Is there bony reaction? l Does the lesion contain calcification? l l

Bone Tumours Differential Diagnosis Haematoma l Infection l Stress fracture l

Bone Tumours Treatment • Rule is excision with or without bone graft • Growth disturbances • Neurovascular compression


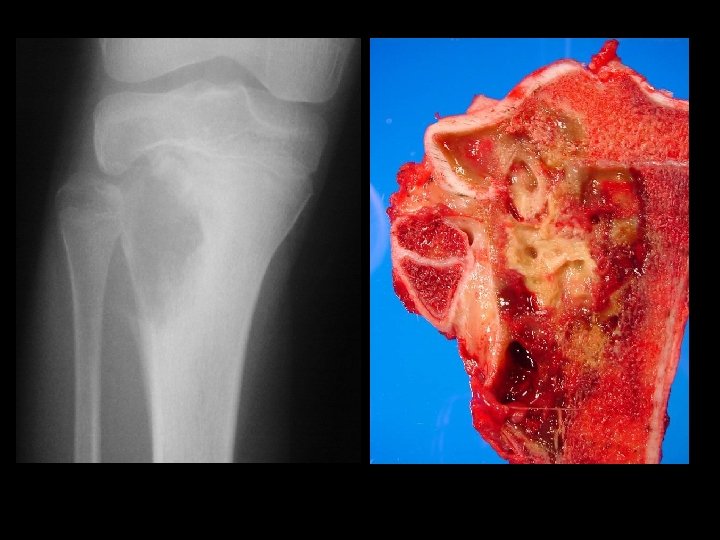
Giant cell tumour • • Uncertain origin Occurs in mature bone Area of old epiphysis Distal femur, proximal tibia, proximal humerus, distal radius.

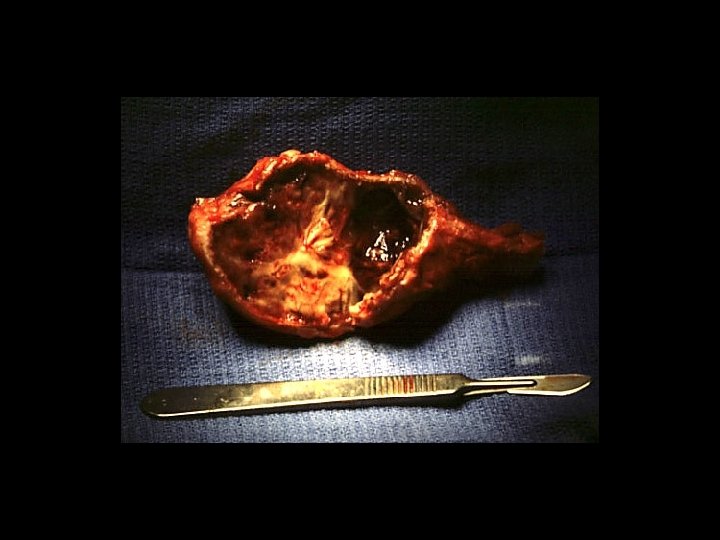





TREATMENT OPTIONS 1. Curettage & bone graft 2. Curettage & bone cement 3. Excision without replacement 4. Excision & replacement with: Artificial prosthesis (custom made) Allograft 5. Excision & replacement with upper end fibula 6. Excision & arthrodesis

THANK YOU


Neoplastic Bone Changes Endochondroma • Most often found in the hands and feet – Radiographic Findings • A well demarcated tumor which causes – thinning and scalloping of the cortex

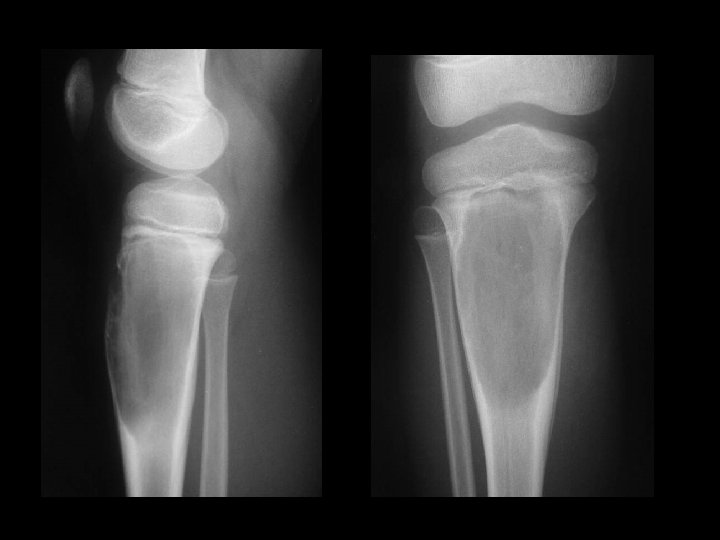
A 14 year old boy presents with pain and a mass above the knee. Take a look at the AP and lateral radiographs first.


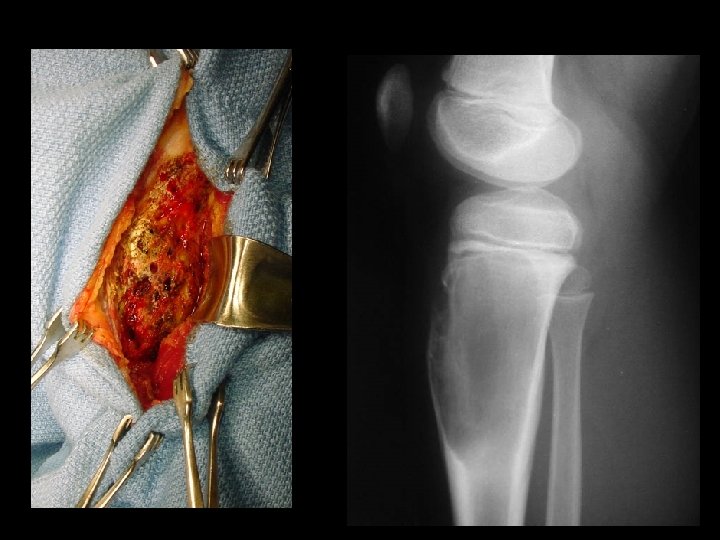
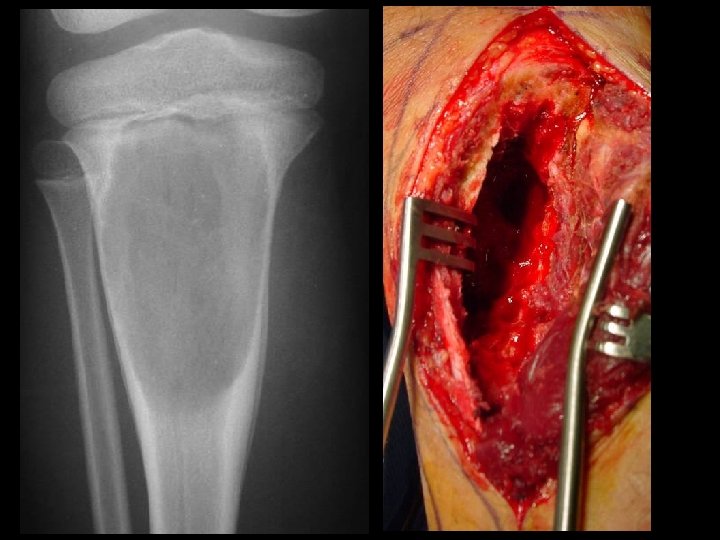
Biopsy obvious superficial mass, blind biopsy • tissue compartments must not be • contaminated Biopsy should be done in consultation with a – tumor surgeon. skinny needle most helpful with metastatic • disease core best for primary tumor •

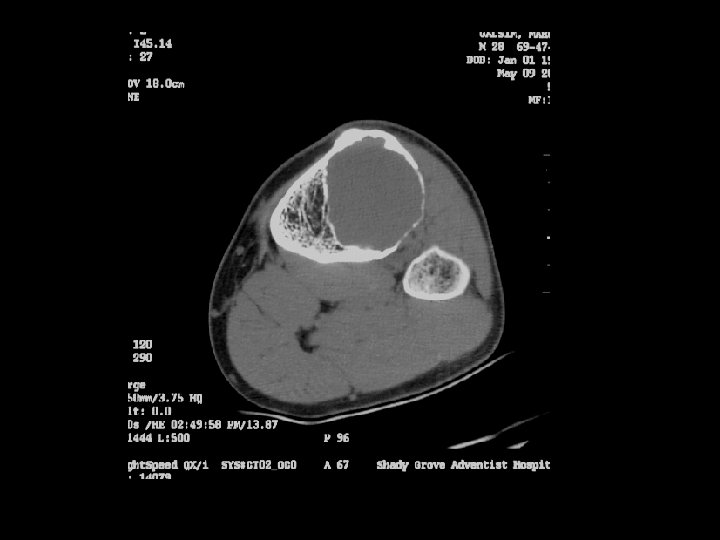
Cross-sectional imaging Pictures are pretty, but diagnosis • established at histology MRI best for most tumors • optimal results at sites with experience – Role of CT limited • may assist in assessing tumor matrix – useful in directing biopsy –

Normal Anatomy diaphysis cortex metaphysi s epiphysis medullar y space physeal scar childhood adult

In case of Bone Tumors: look for Location! Age Age Behavior

Location and age of patient most important • parameters in classifying a primary bone tumor. Simple to determine from plain • radiographs.
 reaction:")
Reaction of bone to tumor Limited responses of bone • destruction: lysis (lucency) reaction: sclerosis remodeling: periosteal reaction Rate of growth determines bone • response slow progression, sclerosis prevails – rapid progression, destruction prevails –

Example 4*, 35 y/o F, GCT

Example 9

Example 9 “onion-skin”

Example 10

Example 10

Example 11

Example 5

Example 5

Example 9

Example 9 “onion-skin”

Example 10

Example 10

Example 11

Summary History • Clinical examination • Plain Radiographs are essential for: • Age – Location – Margins – Aggressiveness of process dictates the – response of the bone Isotope scan • CT scan • MRI • Biopsy •

When ever examining a plain X-ray do not forget to look at:
- Slides: 78