Bells Palsy Nerve injuries Dr Mohammed Kalim Ansari

Bell’s Palsy & Nerve injuries Dr. Mohammed Kalim Ansari

overview • • • Introduction & Definition of Bell’s palsy Etiology Clinical features Management of Bell’s palsy Prognosis Nerve injuries

Management 1. Physiotherapy • the effect of facial paralysis or Bell’s palsy is wasting or muscle atrophy. • to maintain the muscle tone and should be instituted as early as possible. • electrical stimuli by galvanism, gentle massage and facial exercises.

2. Medications • If the patient is seen within 2 to 3 weeks of onset of symptoms—tab prednisolone in doses of 1 mg/kg/d for 10 to 14 days has been recommended with a gradual tapering. • Vitamins B 1, B 6, B 12 may be administered.

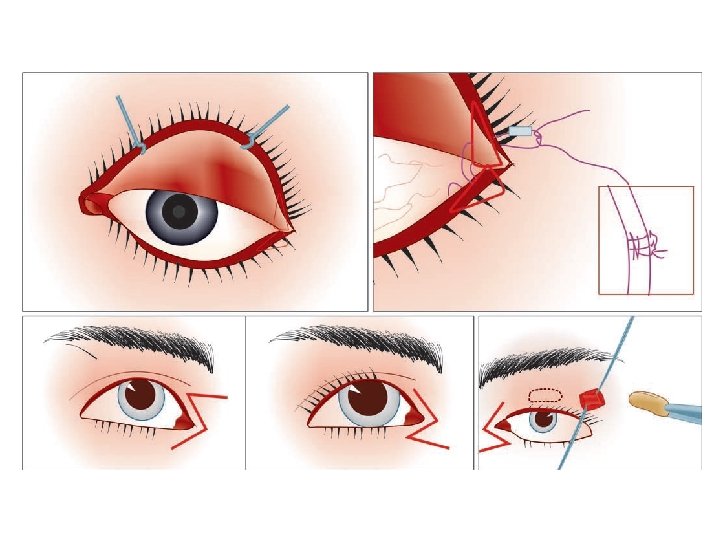
• If incomplete eye closure is present, artificial lubrication, taping the eye or perhaps the placement of a spring, gold weight or tarsorrhaphy might prevent visual loss from exposure keratitis.
 • is a neurotoxin, that temporarily interferes with acetylcholine release")
Clostridium botulinum toxin (Botax) • is a neurotoxin, that temporarily interferes with acetylcholine release from motor nerve endplates, causing skeletal muscle paralysis. • The effect lasts 4 to 6 months. • Botulium toxin has been useful in the treatment of facial paralysis by weakening the contralateral side to allow centering of the mouth, more symmetry on smiling.

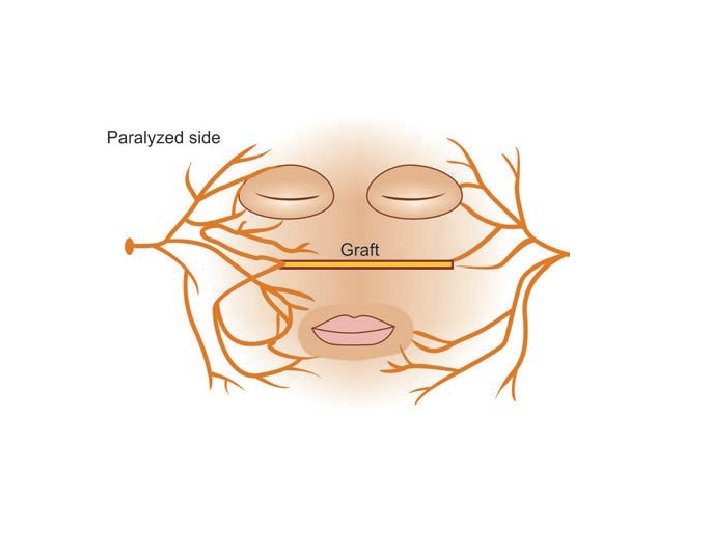
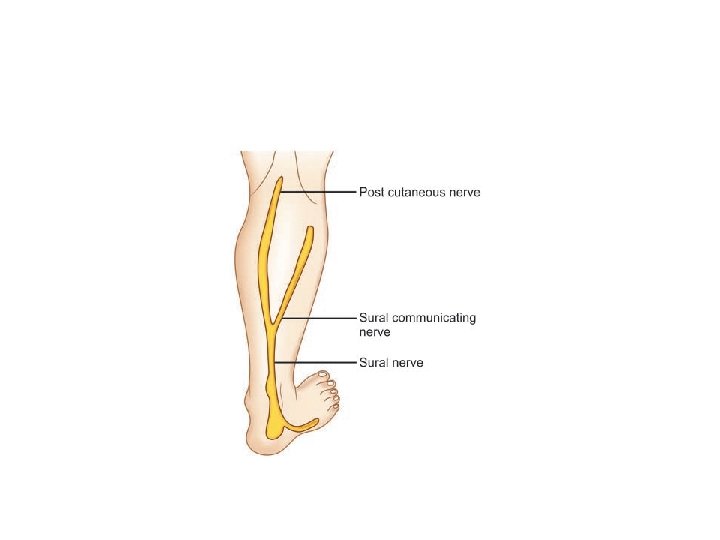
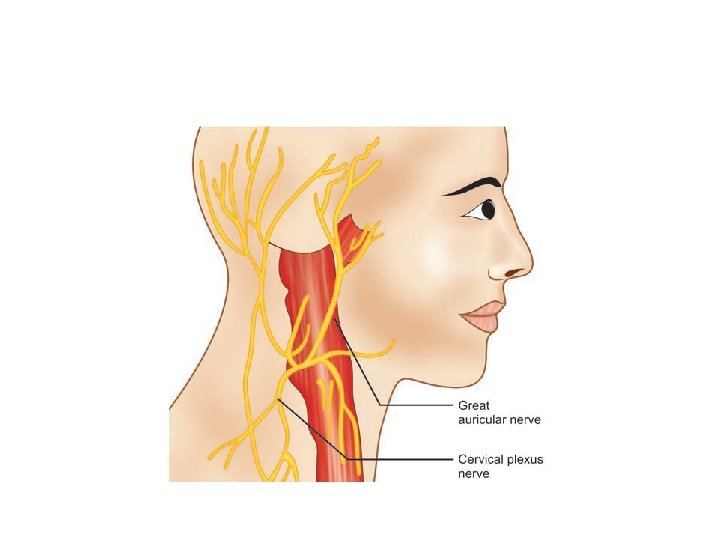
3. Surgical procedures • Nerve decompression—can be carried out internally or externally. • Nerve anastomosis—reanimation— anastomosis of the central end of hypoglossal or spinal accessory nerve with the distal end of the facial nerve is done. • Nerve grafting—whenever there is evidence of neuroma or loss of portion of a nerve, nerve grafting can be considered.

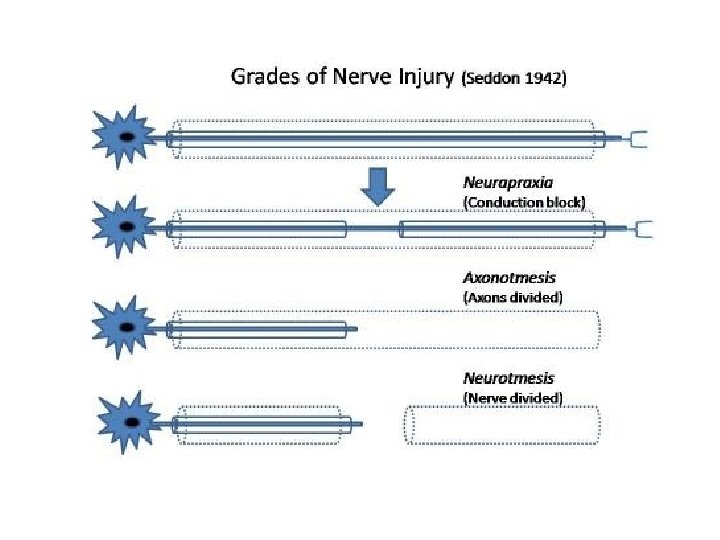
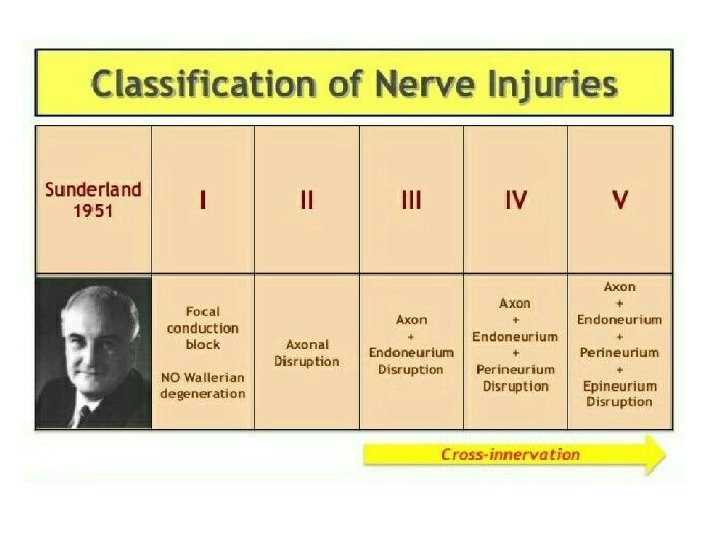
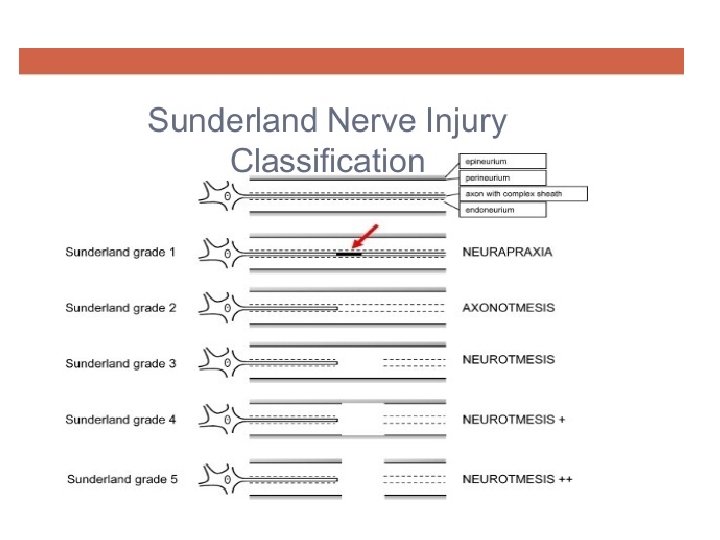
Nerve injuries

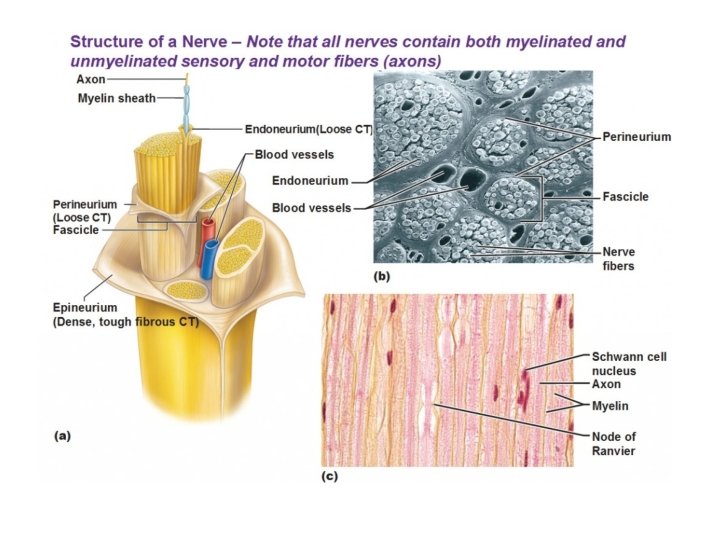
Basic anatomy of nerve
- Slides: 17