BEHETS SYNDROME BS BS is a multisystem vasculitic
 BS is a multisystem vasculitic inflammation that has one basic major")
BEHÇET’S SYNDROME (BS) BS is a multisystem vasculitic inflammation that has one basic major feature- recurrent oral aphthous ulcers (AUs)- and two of any of the following features: recurrent genital AU, eye lesions (anterior or posterior uveitis), skin lesions (erythema nodosum or acneiform papulopustules), and a positive pathergy test. Other manifestations include synovitis, neurologic disorders, and thrombophlebitis.
 •")
Epidemiology • İÖ 5. yy, Hipokrat • 1936, Behçet ( eye disease+orogenital ulcers) • Age of onset: Third and fourth decades, peak incidence 20 -35 y • %2 -5 familial (Middle east %10 -15) • Prevalence: Highest in Japan (1: 10000), Turkey (80: 100000), Southeast Asia, the Middle East, southern Europe. Rare in northern Europe, United States. • Sex: Males > females
")
Pathogenesis • Etiology unknown (neutrophilic vascular reactions or leukocytoclastic vasculitis, vascular thrombosis, autoimmune responses) - Infectious (HSV, Hep C, parvovirus B 19, sreptococcus. . ) - Immunologic ( circulating immune complexes, ↑circulating TNF-alpha, Il-1β, Il-8→ activation of neutrophils↔↑intreaction with endothelial cells) - Genetic + enviromental factors • HLA-B 5 and HLA-B 51 association (eastern Mediterranean and East Asia) • The lesions are the result of leukocytoclastic (acute) and lymphocytic (late) vasculitis.

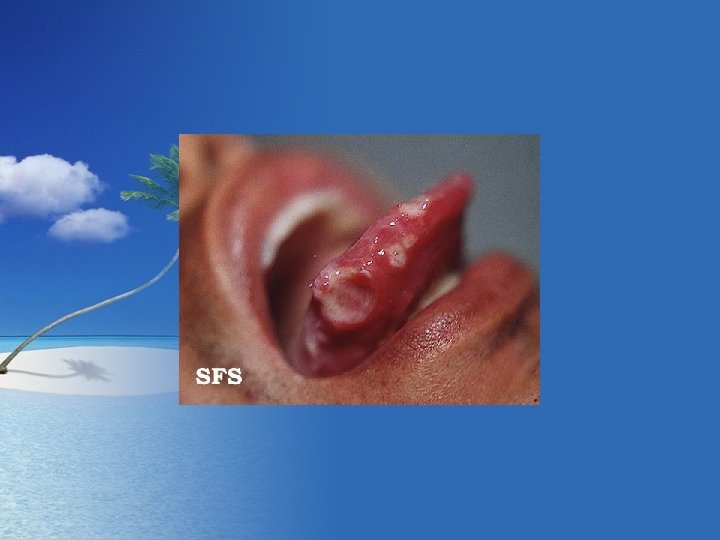
History • Painful ulcers erupt in a cyclic fashion in the oral cavity and/or mucous membranes.
 • Skin and Mucous Membranes – Aphthous Ulcers: Punched-out (3 -10")
Physical Examination (1) • Skin and Mucous Membranes – Aphthous Ulcers: Punched-out (3 -10 mm) with rolled borders and necrotic base; red rim; occur in crops (2 to 10) on oral mucous membrane (%100), vulva, penis, and scrotum; very painful – Erythema Nodosum-like Lesions: Painful inflammatory nodules on the arms and legs – Other: Inflammatory pustules, superficial thrombophlebitis, inflammatory plaques resembling those in Sweet’s syndrome, pyoderma-gangrenosum-like lesions, palpable purpuric lesions of necrotizing vasculitis.
 • Systemic Findings – Eyes: Leading cause of morbidity. Posterior uveitis,")
Physical Examination (2) • Systemic Findings – Eyes: Leading cause of morbidity. Posterior uveitis, anterior uveitis, retinal vasculitis, hypopyon, secondary cataracts, glaucoma, neovascular lesions – Musculoskletal: Nonerosive, asymmetric oligoarthritis – Neurologic: 25 %, onset delayed. Meningoencephalitis, BİH, cranial nerve pulsies, brainstem lesions, pyramidal/extrapyramidal lesions, psychosis. – Vascular: Aneurysms, arterial occlusions, venous thrombosis, varices; hemoptysis. Coronary vasculitis: myocarditis, coronary arteritis, endocaditis, valvular disease. – GI Tract: AUs throughout.
")
Laboratory Examinations • Dermatopathology • Pathergy Test • HLA Typing (Japanese, Koreans, Turks)
, hand-foot-and mouth disease, herpangina, chancre, mucous patch,")
Differential Diagnosis - Viral infection (HSV, VZV), hand-foot-and mouth disease, herpangina, chancre, mucous patch, eritema multiforme, pemfigus, lichen planus, squamous cell carcinoma, avitaminosis (pellegra, scurvy)

COURSE AND PROGNOSIS • Highly variable course, with recurrences and remissions • Remissions may last for weeks, months or yaers • One of the leading causes of blindness • With CNS involvement, there is a higher mortality rate

MANAGEMENT • Aphtous ulcers: Potent topical glucocorticoids. Intralesional triamcinolone, 3 to 10 mg/ml, injected into ulcer base. Thalidomide, 50 -100 mg PO. Colchicine, 0. 6 mg PO 3 times a day. Dapsone, 50 -100 mg PO/day. • Systemic involvement: Prednisone with or without azathioprine, cyclophosphamide, azathioprine alone, chlorambucil, cyclosporine.















- Slides: 26