BEHAVIOUR MANAGEMENT INTRODUCTION Behaviour management is as much

BEHAVIOUR MANAGEMENT

INTRODUCTION Behaviour management is as much a clinical skill as it is a science. It is not an application of individual techniques created to ‘deal’ with children, but rather a comprehensive methodology meant to develop a relationship between patient and doctor which ultimately builds trust and diminishes fear and anxiety.

DEFINITION BEHAVIOUR MANAGEMENT It is the means by which dental health team effectively and efficiently performs dental treatment for a child and at the same time instills a positive dental attitude.

BEHAVIOUR SHAPING Is The Procedure Which Slowly Develops Behaviour By Reinforcing A Successive Approximation Of The Desired Behaviour Until The Desired Behaviour Comes Into Being. BEHAVIOUR MODIFICATION Behavior Modification Is Defined As ” The Attempt To Alter Human Behavior & Emotion In A Beneficial Manner According To The Laws Of Modern Learning Theory”

OBJECTIVES • Establish effective communication with child and parent. • Gain child’s and parent’s confidence and acceptance of dental treatment. • Teach children and parents the positive aspects of preventive dental care. • To provide a relaxing and comfortable environment for the dental team to work in, while treating the child.

FUNDAMENTALS • Positive approach • Team attitude-the team should have interest, friendly and caring attitude. • Organization – effective planning without delay or indecisiveness • Truthfulness • Tolerance – rationally coping with child’s behaviour • Flexibility – if necessary, altering the treatment plans wisely.

Factors which affect child’s behaviour in the dental office. Under the control of the dentist • Effect of dental office environment. • Effects of dentist’s activity and attitude. • Dentist’s attire. • Presence / absence of parents in the operatory • Presence of an older sibling

Out of control of the dentist. • Growth and development. • Nutritional factors. • Past dental experiences. • Genetics. • School environment. • Socioeconomic status.

Under the control of the parents. • Home environment. • Family development and peer influence. • Maternal behaviour.

Mothers behavior 1. Overprotective, Child’s behavior - shy, submissive, anxious, dominant 2. Overindulgent - aggressive, demanding, display of temper tantrums

3. Under affectionate - usually well behaved but may be unable to cooperate, shy, may cry easily 4. Rejecting - aggressive, overactive, disobedient. 5. Authoritarian - evasive and dawdling
![Frankle’s Behaviour Rating Scale Rating 1 : [ Definitely Negative ] Refusal of treatment,](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-12.jpg "Frankle’s Behaviour Rating Scale Rating 1 : [ Definitely Negative ] Refusal of treatment,")
Frankle’s Behaviour Rating Scale Rating 1 : [ Definitely Negative ] Refusal of treatment, cries forcefully, or any other evidence of extreme negativism. Rating 2 : [ Negative ] Reluctant to accept treatment, not pronounced negative attitude. , Rating 3 : [ Positive ] Acceceptance of treatement, at times cautious follows dentist instrutions Rating 4 : [ Definitely positive ]Good raport with the dentist, takes interest in treatment & procedure
![Advantages of Frankl rating 1] It is functional. 2] It is quantifiable. 3] It](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-13.jpg "Advantages of Frankl rating 1] It is functional. 2] It is quantifiable. 3] It")
Advantages of Frankl rating 1] It is functional. 2] It is quantifiable. 3] It is reliable. 4] It is economic & eaisly applicable.
![Clinical classification by Wright { 1975 } A] Positive behaviour 1] Co-operative child :](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-14.jpg "Clinical classification by Wright { 1975 } A] Positive behaviour 1] Co-operative child :")
Clinical classification by Wright { 1975 } A] Positive behaviour 1] Co-operative child : These children are relaxed, show minimum apprehension, can be managed by behaviour shaping approach.
![2] Lacking in co-operative ability : Usually seen in very young children with whom](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-15.jpg "2] Lacking in co-operative ability : Usually seen in very young children with whom")
2] Lacking in co-operative ability : Usually seen in very young children with whom communication cannot be established. 3] Potentially co-operative : Children fall under this category have some behaviour problems, [fear] Has the potential to co-operate
![B ] Negative behaviour a] Uncontrolled / Hysterical / - Preschool children at their](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-16.jpg "B ] Negative behaviour a] Uncontrolled / Hysterical / - Preschool children at their")
B ] Negative behaviour a] Uncontrolled / Hysterical / - Preschool children at their first visit, - Temper tantrum i e, physical lashing out of legs, arms, loud crying and refuses to co-operate.
![b] Obstinate - behaviour : This type can be seen any age group. -](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-17.jpg "b] Obstinate - behaviour : This type can be seen any age group. -")
b] Obstinate - behaviour : This type can be seen any age group. - Usually in spoilt or stuburn children. - These children made co-operative. c] Timid behaviour : - Usually seen in a overprotected child at the first visit. - Is shy but co-operative.
![d] Tense co-operative : - These children are the borderline positive and negative behaviour.](http://slidetodoc.com/presentation_image_h2/a0207fc6d383401f2e376e5f193cad7c/image-18.jpg "d] Tense co-operative : - These children are the borderline positive and negative behaviour.")
d] Tense co-operative : - These children are the borderline positive and negative behaviour. e] Whining behaviour : - Complaining type of behaviour. - Allows for treatment but complains. f] Stoic behaviour : - Seen in physically abuse children. - They are co-operative and passively accepts all treatment.
CO-OPERATIVE: physically and emotionally co-opeerative regardless of treatment")
• LAMPSHIRE’S CLASSIFICATION – 1970 1)CO-OPERATIVE: physically and emotionally co-opeerative regardless of treatment 2)TENSE CO-OPERATIVE: co-operative but tensed. Tension may be unnoticed 3) OUTWARDLY APPREHENSIVE: hides behind mother, avoid looking or talking to dentist eventually accept treatment. 4) FEARFUL: require considerable support. Modeling, desensitization and other behaviour modifications become necessary. 5. STUBBORN OR DEFIANT: resist or try to avoid treatment. 6. HYPERMOTIVE: actually agitated, scream and start fighting. 7. HANDICAPPED: physically, mentally or emotionally handicapped. 8. Emotionally immature.

Personality Of The Dentist And Ancillary Help • • • Confidence Feel and act kindly Good psychology Conversation No force
 Communication 2) Behavior shaping ( modification )")
NON PHARMACOLOGICAL METHODS OF BEHAVIOUR MANAGEMENT 1) Communication 2) Behavior shaping ( modification ) a. desensitization b. modeling c. contingency management(reinforces )
 Behavior management a. Audio analgesia c. Voice control e. Humor g. Relaxation i.")
3) Behavior management a. Audio analgesia c. Voice control e. Humor g. Relaxation i. Aversive conditioning b. Bio feed back d. Hypnosis f. Coping h. Implosion therapy
 Verbal communication b) Non verbal communication c) Both")
COMMUNICATION • Types of communication a) Verbal communication b) Non verbal communication c) Both using verbal and non verbal

VERBAL - establishment of communication - message clarity Transmitter – Medium – Receiver • There has to be a fit between the intended message and the understood one

Voice control • Sudden and firm commands • Monotonous and soothing • Attempt to influence behavior directly • Greenbaum et al – loud commands reduced disruptive behavior. • Theory of chambers: voice control is most effective when used with other communications

Use of euphemisms Dental terminology Word substitutes rubber dam rubber raincoat sealant tooth paint air syringe wind gun water syringe water gun suction vacuum cleaner airotor whistling water gun
 Body language Smiling Eye contact Showing concern")
NON VERBAL COMMUNICATION ( MULTI SENSORY COMMUNICATION) Body language Smiling Eye contact Showing concern Touching the child Giving him a pat Giving a hug Expression of feelings without speaking Greenbaum et al – this contact helped children to relax, esp 7 -10 yrs of age.

BEHAVIOR MODIFICATION • Desensitization • Modeling • Contingency management

DESENSITIZATION • Joseph Wolpes • Gradational exposure of child to his/her fear • Wolpe’s technique, known as systematic desensitization, is based on relaxation and played a very prominent role in the evolution of behavior therapy during the 1960 s and 1970 s. • The treatment procedure is carried out in multiple sessions. The use of systematic desensitization involves three sets of activities. A. Encourage the patients to discuss their status of fear and anxiety, in order to construct a hierarchy of feared dental situations, from the least to the most anxiety-provoking. B. Teach the patient relaxation techniques. The most commonly used techniques are breathing and muscle relaxation. C. The final step is to gradually expose the patient to these situations in the hierarchy, from the least to the most anxiety-promoting.
 • Addleston 1959 • The dentist using the language that the")
Tell-Show-Do Technique (TSD) • Addleston 1959 • The dentist using the language that the child can understand tell the patient what is to be done. It is presented slowly and repeatedly. • The dentist demonstrates the procedure to the child using a model or himself and is done slowly. • The dentist proceeds to the dental procedure exactly as described. • Effective in children more than 3 yrs of age.

MODELING • Bandura 1969 – social learning procedure • “ learning occurs as a result of direct experience – witnessing the behavior and outcome of that behavior for other people” • Live models, posters, filmed models, audiovisual aids. • 3 requirements: Ø concentrated attention Ø sufficient retention Ø reproduce effectively

, is a systematic reinforcement of desired behaviors and")
CONTINGENCY MANAGEMENT • Contingency management (CM), is a systematic reinforcement of desired behaviors and the withholding of reinforcement of undesired behaviors, is an effective strategy in the management of behavior. • Contingency management is based on the principle that behavior is a function of its consequences. • For example, if an action is followed by a positive consequence as perceived by that person, then the individual is likely to repeat that action. In contrast, if an action is followed by a negative consequence as perceived by that person, then the individual is unlikely to repeat the action.

• Positive reinforcement and contingent escape: • For example, offering a reinforcement which is important in the patient’s value system will give better results than things that do not hold any importance for her. It is a good idea to ask the caretaker of the patientabout a favorite activity or a demand, as simple as being allowed to play, watch a favorite television show or a time out from dental procedure as reinforcement, because a meaningless reinforcement may result in undesirable outcome. • Negative reinforcement and removal of contingent escape: A negative reinforcement is anything that, when taken away contingent on a response, tends to increase the probability or rate of that response

Non contingent reinforcement: Extinction occurs when a behavior is followed by no response, which decreases the likelihood of the behavior occurring again[5]. Ignoring the undesirable behavior will reduce the likelihood of the repetition of the behavior even though the patient may have indulged in it, consciously or unconsciously, to have an effect on the operator. Presentation or withdrawal of reinforcers a. positive reinforcers – Henry W Fields 1984 b. negative reinforcers – Strokes and Kennedy 1980 Types of reinforcements: social, material, activity reinforcers
 Social: for e. g. praise, positive facial expressions,")
Types of reinforcerments can be: a) Social: for e. g. praise, positive facial expressions, physical contact by shaking hand, holding hand, and patting shoulder or back. b) Material: May be given in the form of toys, games, sweet are not given - as reward since it causes caries. c) Activity reinforcer: Involving the child in some activity like watching a TV show/ special programmes with him. For the benefit of contingency management social reinforcers are the most effective.

BEHAVIOUR MANAGEMENT • • • Audio analgesia Biofeed back Humor Coping Voice control Relaxation Hypnosis Implosion therapy Aversive conditioning
 is the relief of pain using")
AUDIO ANALGESIA • Audioanalgesia (also known as audio-analgesia) is the relief of pain using white noise or music without using pharmacological agents while doing painful medical procedures such as dental treatments. It was first introduced by Gardner and Licklider in 1959. • Audio analgesia or ‘white noise’ is a method of reducing pain. This technique consists of providing a sound stimulus of such intensity that the patient finds it difficult to attend to anything else. (Gardner, Licklider, 1959) • Auditory stimulus such as pleasant music has been used to reduce stress and also reduce the reaction to pain.

• It has also been suggested that music may stimulate the production of endorphins and catecholamines. (Endorphins are closely linked with the release of oxytocin. They are also 'feel good' hormones, released when we are feeling relaxed. They help women cope with pain in labour, acting as natural painkillers. ) • The noise directly suppresses the pain caused by dental anaesthesia. • The noise masks the sound of dental drill and removes source of conditioned anxiety. • Music and noise cause relaxation

• Parts of the pain and auditory systems come together in several regions of the reticular formation of the brain. interactions between the two systems is inhibitory.

BIOFEED BACK • Biofeedback is also referred to as applied psychophysiological feedback, and is a mind–body technique. • The information assists the patient in gaining self-regulation of the physiological process being monitored. Monitoring oneself and then utilizing the information to practice and achieve selfregulation are the main goals of biofeedback. • For example if blood pressure is high the instrument gives stimulation and the subject is taught to control the signals, therefore it is useful in anxiety and stress related disorders. Electroencephalogram, electromyography can also be used in bio-feed back

• Reduction of muscle-tension levels through electromyographic biofeedback and operant conditioning of brain-wave activity through electroencephalographic biofeedback are commonly used for reducing anxiety. • Recently, the use of respiratory rate-biofeedback device has been shown to reduce preoperative general anxiety levels Biofeed back involves the use of certain instruments to detect certain physiological processes associated with fear. (Buonomono, 1979)

HUMOR Helps to elevate the mood of the child, which helps the child to relax. Functions of humor a) Social: Forming and maintaining a relationship. B) Emotional: Anxiety relief in the child, parent and doctor. C) Informative: Transmits essential information in a non- threatening way. D) Motivation: It increases the interest and involvement of the child. e) Cognitive: Distraction from fearful stimuli
 COPING : It is the mechanism by which the child copes up with")
4) COPING : It is the mechanism by which the child copes up with the dental treatment. It is defined as the cognitive and behavioral efforts made by an individual to master, tolerate or reduce stressful situations Patients under stress prefer to draw comfort or reassurance from an authority figure. Thus establishing a close or trusting relationship with the doctor nurse.
 Behavioral: Are physical and verbal activities")
Coping effects may be of two types A) Behavioral: Are physical and verbal activities in which the child engages to overcome a stressful situation. B) Cognitive: The child may be silent and thinking in his mind to keep calm. Cognitive coping stragies can enable the children to: * Maintain realistic perspective on the events at hand * Perceive the situation as less threatening

RELAXATION • This technique is used to reduce stress. • It is based on the principle of elimination of anxiety. • Relaxation involves a series of basic exercises, which may take several months to learn, and which require the patient to practice at home for atleast 15 mins per day.

HYPNOSIS • Hypnosis is an altered state of consciousness characterized by a heightened suggestibility to produce desirable behavioral and physiological changes. • Greatest benefit of hypnosis is to reduce anxiety and pain.

IMPLOSION THERAPY • Sudden flooding with a barrage of stimuli which have affected him adversely and the child has no other choice but to face the stimuli until a negative response disappears. • Implosion therapy mainly comprises of HOME, voice control and physical restaints.

AVERSIVE CONDITIONING • Aversive conditioning can be a safe and effective method of managing extremely negative behaviour. • Two common methods used in clinical practice are HOME and physical restraint.
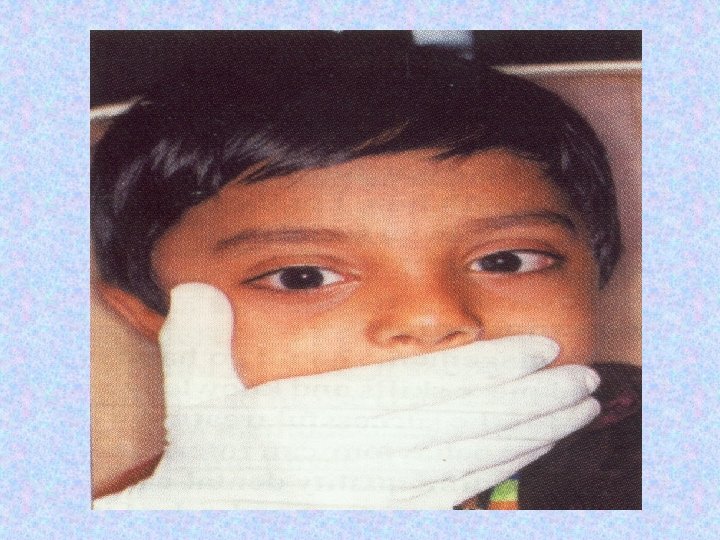
 • Introduced by Evangeline Jordan, 1920 • The purpose")
HOME (Hand Over Mouth Exercise) • Introduced by Evangeline Jordan, 1920 • The purpose of HOME is to gain attention of the child so that communication can be achieved

INDICATIONS: • A healthy child who can understand but who exhibits defiance and hysterical behaviour during treatment. • 3 -6 yrs old • A child who can understand simple verbal commands. • Children displaying uncontrollable behaviour.

CONTRAINDICATIONS: • Child under 3 yrs of age. • Handicapped child/immature child, frightened child. • Physical, mental and emotional handicap.

TECHNIQUE: • The dentist firmly places his hand over the child’s mouth and behavioral expectations are calmly explained close to the child’s ear. • When the child’s verbal outburst is completely stopped and the child indicates his willingness to co-operate, the dentist removes his hand. • Once the child co-operates, he should be complimented for being quiet and praised for good behaviour.

• It should be noted that the child’s airway is not restricted while performing the technique and the whole procedure should not last for more than 20 -30 seconds.

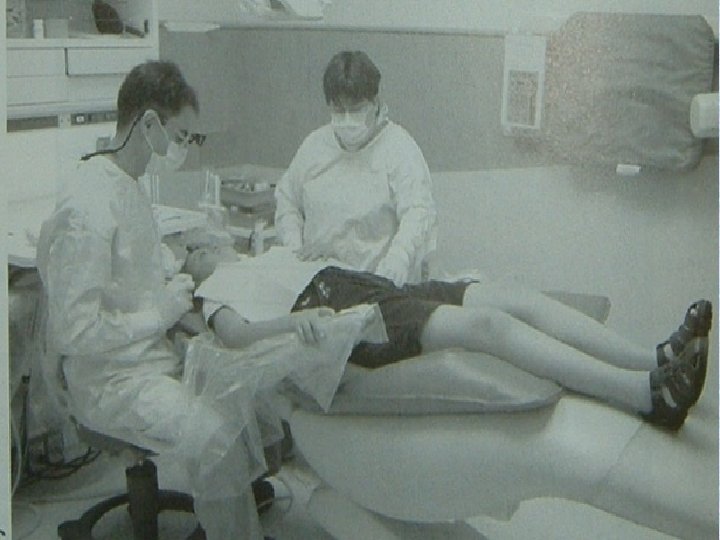
PHYSICAL RESTRAINT • Restraints are usually needed for children who are hypermotive, stubborn or defiant. - Kelly 1976 • Involve restriction of childs head, hands, feet, or body. Active Passive

TYPES OF RESTRAINTS • For body: Ø pediwrap Ø papoose board Ø sheets Ø bean bag with straps Ø towels and tapes

For extremities: Ø Velcro straps Ø Posey straps Ø Towel and tape.
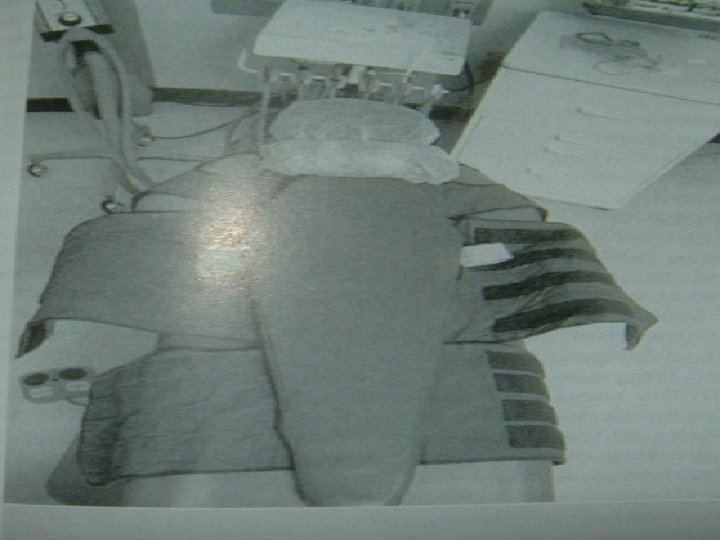

USE OF RESTRAINTS SHOWN

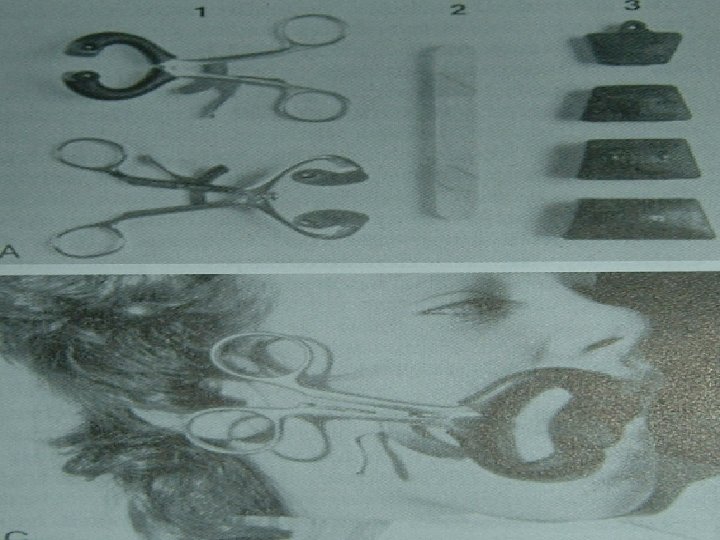
For mouth: Ø mouth blocks Ø tongue blades Ø mouth props

For head: Ø Head positioner Ø Forearm body support

HEAD POSITIONER

- Slides: 69