Behavioral Emergencies 2015 Three patients to see A

Behavioral Emergencies 2015

Three patients to see. . . A. 24 year old female with multiple superficial lacerations to left arm. Boyfriend called police, apparently was in an argument and locked herself in the bathroom threatening suicide. Brought by police. The triage nurse has known her for years. VS 78, 130/70, 22, O 2 sat 97% pain 15/10. GCS=15.

B. 43 year old male fell off a ladder and had a brief period of unresponsiveness. Awoke with moderate headache and walked into the kitchen. 20 minutes later his wife noted he seemed a bit confused and staggered a bit walking to the living room. When he didn’t seem to know where he was, she called the ambulance. He is now insistent that he be allowed to go home, gets up off the stretcher and pushes away the nurse. VS 68, 140/105, RR 12, O 2 sat 94%, GCS=14.

B.

C. A 36 year old male presents with his wife, who says that they are having difficulty at home. He is demanding and argumentative, and his wife is worried especially over money he has spent lately. He has run out of medications and his family doctor is away for two weeks. He hasn’t been sleeping more than 1 or 2 hours per night. He has plans to sell his business and start a new one. One night he was out driving his car all night. VS 110, 145/90, 20, O 2 sat 97%, GCS=15.

1. Discuss the approach to the agitated psychiatric patient. 2. Discuss the approach to the agitated medical/ surgical patient. 3. Display knowledge of the appropriate therapeutic choices for various scenarios. 4. Discuss the concept of “medical clearance”. 5. Display knowledge of suicide risk stratification. 6. Discuss the indications and contraindications for emergency psychiatric consultation. 7. Display knowledge of involuntary commitment and the legal aspects of this act. 8. Discuss the approach to and treatment of the anxious patient. 9. Knowledge of the differential diagnosis for confusion in the elderly. Objectives

�Managing Violent Patients Acute Agitation: Psychosis Organic Behavioral

Emergency Psychiatric Assessment Steps Safety and stabilization Identification of homicidal, suicidal, or other dangerous behavior Medical evaluation Psychiatric diagnosis and severity assessment Psychiatric consultation

What are potential causes of agitation or violent behavior? �Organic - deriving from medical disorders, including substance abuse and other toxidromes. � Drug/etoh withdrawal � Toxidromes � Endocrinopathies � Metabolic derangements � Substance abuse � Infections � Neurologic illness �Psychotic – schizophrenic, manic, delusional. �Non- organic, non-psychotic – personality disorders, impulse control disorders.

Risk Factors for Violence List some risk factors for violence: �Previous history of violence �Intoxication �Paranoid delusions �Drug/etoh withdrawal �Personality Disorder

Taylor—psychosis vs violence �The risk of being violent is raised by psychosis: what is the likelihood that a violent episode is due to psychosis? � 95% to 99% of society’s violence must be explained otherwise. � When violence is a problem, who is most at risk? � immediate social circle of a patient with psychosis are most at risk. �What are the 2 main routes by which psychosis is related to violence? 1. 2. Individuals unremarkable before the onset of illness and their violence is driven by psychotic symptoms; conduct, emotional difficulties and/or childhood abuse preceded the psychosis; lifestyle and substance misuse may be more prominent factors in the violence.

De-escalation Principles �Perceived threat is a major driver �Act as an advocate, not an adversary �Make patient comfortable �Create a therapeutic alliance

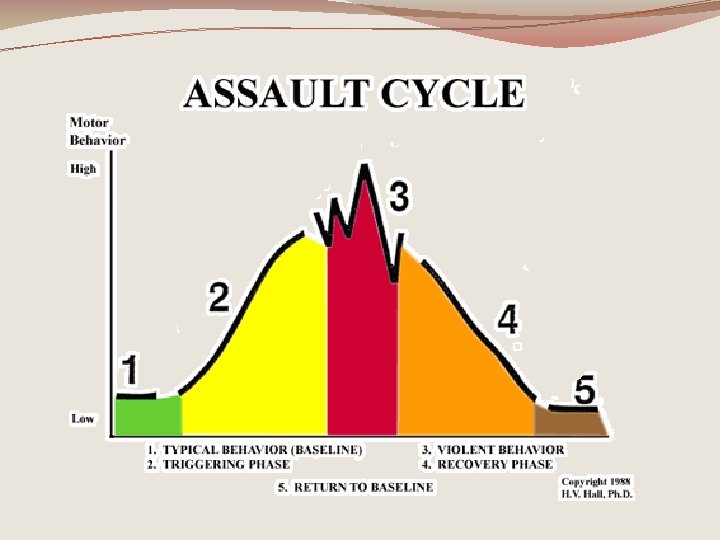
Recognize Agitation Early Escalating �Tension �Hostility �Uncooperativeness �Excitement �Poor impulse control �Angry �Pacing/restlessness �Clenched fists �Loud speech/shouting

Prevention �See them fast �Disarm patient �Private but not isolated bed �Safe room= no weapons �Keep door open �Security nearby �You and patient equidistant to door �Safe you = no weapons

De-escalation Principles: CANIT �C=Containment & Safety �A=Assessment �N=Nonviolent De-escalation Techniques �I=Intervention �T=Takedown & Control

De-escalation 10 Techniques �Respect personal space �Don’t provoke pt. �Establish verbal contact �Be concise �Identify wants/feelings �Listen closely �Agree or agree to disagree �Set clear limits �Offer choices and optimism �Debrief patient and staff

PO Drugs �Offers patient choice and control �Strengthens therapeutic alliance �Preferred by patients �Fast acting �Benzos & Antipsychotics

Physical Restraint �Systematic, consistent, protocol-driven and practiced techniques are best. �Preserve the physician- patient therapeutic alliance where possible. �Restraint team – at least 5 trained members and an experienced leader. �team should enter the room in unison. �Leader moves to the head and other members each take a limb.

Restraint Documentation �Time limited order �Patient’s presentation and reason for restraint, including the potential danger to patients or others. �The plan of care. �Assess decision making capacity. � Nursing notes: � injuries � frequent assessment � vital signs, � medical and behavioural status; � readiness for discontinuation of restraint.

Really Agitated �benzos still preferred, PO if possible �Lorazepam � 0. 5 – 2 IM/PO mg q 30 min. � reliable IM absorption, no metabolites �Consider midazolam � quicker onset IM, lasts 45 mins. � 5 mg IM q 15 min �haloperidol 5 mg + lorazepam 2 mg IM �More rapid sedation �Alternative: �Olanzepine 10 mg IM

Delirium

84 year old female �Brought in by daughter because she has is more sleepy in the daytime than usual, not getting out of bed as much, appetite is markedly decreased �Says she feels quite well, but has a cough �Daughter says she seems slightly confused off and on in last three days.

Delirium and Dementia

Compare dementia & delirium �Dementia— � chronic � impaired cognitive functioning in several areas, including memory, abstract thinking, judgment, personality, and other higher cortical functions such as language �Delirium == � acute � impairment in cognitive function & � clouding of consciousness, a reduction in the awareness of the external environment (manifest as difficulty sustaining attention), varying degrees of alertness ranging from drowsiness to stupor, and sensory misperception

Delirium is Common! �up to 70% of cases missed � 11%-42% of medical inpatients have delirium �Increased mortality, readmission, complications, falls, institutionalization, length of stay, aggression �drugs are most common reversible cause of delirium � especially anticholinergics, benzodiazepines and narcotics � diphenhydramine (Benadryl) associated with cognitive decline and urinary retention in hospitalized elderly (also dimenhydrinate)

Two Types of Delirium � 25 % --Agitated �usually identified �Most: Hypoactive �often missed �higher mortality
 � Fracture")
Delirium Risk Factors � Admission Characteristic vs Odds Ratio (95% Confidence Interval) � Fracture 6. 6 (2. 2 -19. 3) � Cognitive impairment 6. 3 (2. 9 -13. 7) � Age >80 5. 2 (2. 6 -10. 4) � Severe illness 3. 5 (1. 5 -8. 2) � Age >65 3. 0 (1. 2 -7. 7) � Infection 3. 0 (1. 4 -6. 1) � Vision impairment 1. 7 (1. 0 -2. 8) Neurohospitalist. 2013 October; 3(4): 194– 202.
 �")
AEIOU M&M TIPS Mnemonic for Delirium Etiology � E - epilepsy (especially post-ictal) � I - infection � O - oxygen (hypoxia) � U - uremia � M - myocardial infarction � & - anesthesia � M - metabolic � T - trauma/fracture � I - Insulin � P - polypharmacy � S - stroke All cases of Delirium require investigation for underlying organic cause

Mental Status and Mini-Mental State Examinations MMSE: Cognitive testing � the MMSE consists of a series of tasks that assess � � � � orientation, immediate and short-term memory, attention, calculation, language, visual construction. A score of 23 or less (out of a maximum possible of 30) = cognitive impairment.

CAM for delirium

Prevention �nonpharmacological intervention may prevent delirium in hospitalized older patients �education of family members about delirium, presence of clock, calendar, familiar objects, glasses in patient's room, reorientation of patient by family members, and extended visitation times �Reduced delirium (NNT 13), falls � Ageing 2012 Sep; 41(5): 629

Delirium in Elderly Dementia �Training, environmental intervention by guideline decreases use of restraints, increases family & patient satisfaction. �Antipsychotic use increases mortality �No clear benefit to any medication interventions Geri-EM Education Program

Delirium Rx �Support: �Quiet room, low lights, familiar people/ objects, re- orientation. �Avoid physical restraints. �Low dose haldol or risperidone. Treat pain, cause. �Caution re: drugs in elderly dementia—risk vs benefit �Increased mortality with antipsychotics �Benzos and anticholinergics can worsen sx. �No evidence cholinergics work

Two patients to see. . . �Case 1. Police bring in a 43 -year-old male to the ED after he threatened to kill his wife and then shoot himself. He insists that he just “lost his cool” but now feels better and wants to leave. He lost his job and has been drinking more heavily in the past couple months leading to arguments. �Case 3: 23 year old female complains of chest pains, palpitations, dizziness, nervousness and tremors over the past several months. Says family doctor not listening to her.

Clinical Assessment in the ED Clinical Assessment of the Patient with Suicide Risk 1. Medical history 2. Psychiatric history 3. Suicidal behavior history (previous attempts) 4. Substance use history 5. Psychosocial history --life stressors, impulsivity, aggression, relationships 6. Family psychiatric history to include history of suicide 7. Physical examination 8. Mental status examination (MSE) 9. Relevant laboratory tests 10. Drug inventory, including over-the-counter (OTC) drugs and supplements

Anxiety Disorders �Panic/Agoraphobia �GAD �Phobias �OCD �ASD/PTSD

Anxiety Shearer SL. Recent Advances in the Understanding and Treatment of Anxiety Disorders. Prim Care Clin Office Pract 34(2007) 475. • • • most common mental health disorders, more prevalent than both affective and substance abuse disorders. 1 -year prevalence 16% lifetime prevalence is 28. 8% median age of onset among mood disorders (age 30), median age of onset among anxiety disorders is much younger (age 11). Anxiety disorders can adversely affect quality of life, mobility, education, employment, social functioning, health care, and physical well being. • a primary anxiety disorder often contributes to secondary depression or substance abuse. • comorbidity with physical conditions associated with poor quality of life and disability. • Anxiety disorders impose a societal economic burden comparable with the cost of depression

Generalized Anxiety Disorder �GAD is the anxiety disorder linked to the highest frequency (35. 6%) of self-medication with alcohol and drugs, �associated with greater comorbidity and suicidality �in one sample, 87% of primary care patients with GAD did not present with the complaint of anxiety or worry; �most had nonspecific somatic complaints (eg, insomnia, head/muscle aches, fatigue, GI Sx)

Panic Disorder/ Agoraphobia Treatment Patient Education important! Feelings vs cognition Cognitive Behavioral Therapy True remission of panic disorder with high functioning occurs in 50% to 70% of patients who receive CBT SSRIs, SNRI’s highly effective compared with placebo high rate of discontinuation syndrome Benzodiazepines are considered second-line or adjunctive treatment • failure to address frequent comorbid depression, • tolerance or abuse potential, • effects on driving, and • possible deleterious effects on cognitive–behavioral treatment (CBT), especially with as-needed use Switch: nonresponder to CBT, SSRI trial may work, & vice versa

Acute intervention �Anxiety—avoidance—relief cycle �Face fears—cognitive reframing & education �Normalize feelings vs cognition �Teach patience & ability to delay and reflect vs react �“Wagon wheel in a rut” �Positive messages need repetitive reinforcement & support

Depression vs Anxiety

Major Depressive Disorder �Insomnia/ sleep disturbance �Anhedonia �Depressed mood �Suicidal thoughts �BHP 9 tool �Time �(SAD PERSONS mnemonic)

Comorbid—Medical Illness Cafarella, et al Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: A literature review. Respirology 2012. 17: 627.

COPD

How do YOU Treat Depression?

Treat: • to bear oneself toward : use <treat a horse cruelly> • to care for or deal with medically or surgically <treat a disease>

Spirito A. Cognitive. Behavioral Therapy for Adolescent Depression and Suicidality Child Adolesc Psychiatric Clin N Am 20 (2011) 191– 204 NNT=4 Hollon S. et al Effect of Cognitive Therapy With Antidepressant Medications vs Antidepressants Alone on the Rate of Recovery in Major Depressive Disorder A Randomized Clinical Trial JAMA Psychiatry. doi: 10. 1001/jamapsychiatry. 2014. 1054 online Aug 20, 2014 Cuijpers P Combined pharmacotherapy and psychotherapy in the treatment of mild to moderate major depression? JAMA Psychiatry 2014; 71(7): 747 -8

Management: Depression �CBT—as effective as Psychopharm �Start in mild to moderate �May need reduction of symptoms first in severe depression �Psychopharmaceutical �SSRI: first line (caution in Bipolar illness) �SNRI �Caution re benzodiazepines


Simkin D, Black N. Meditation and Mindfulness in Clinical Practice Child Adolesc Psychiatric Clin N Am 23 (2014) 487– 534 Miller. Neuroanatomical Correlates of Religiosity and Spirituality. JAMA Psychiatry, 2013; 1 DOI: 10. 1001/jamapsychiatry. 2013. 306 Rasic, D et al. Longitudinal relationships of religious worship attendance and spirituality with major depression, anxiety

Williams N et al. Interventional psychiatry: how should psychiatric educators incorporate neuromodulation into training? Acad Psychiatry. 2014 Apr; 38(2): 168 -76.

Nyer M What is the Role of Alternative. Treatments in Late-life. Depression? Psychiatr Clin N Am 36 (2013) 577– 596

Yinger, el al. Music Therapy and Music Medicine for Children and Adolescents Child Adolesc Psychiatric Clin N Am 23 (2014) 535– 553

Gow R, Hibbeln J. Omega-3 Fatty Acid and Nutrient Deficits in Adverse Neurodevelopment and Childhood Behaviors Child Adolesc Psychiatric Clin N Am 23 (2014) 555– 590 X Popper CW. Single-Micronutrient and Broad-Spectrum Micronutrient Approaches for Treating Mood Disorders in Youth and Adults Child Adolesc Psychiatric Clin N Am 23 (2014) 591– 672

Diamond, P et al. Ketamine infusions for treatment resistant depression: a series of 28 patients treated weekly or twice weekly in an ECT clinic J Psychopharmacol June 2014 28: 536 -544 Price R et al Effects of ketamine on explicit and implicit suicidal cognition: a randomized controlled trial in treatment-resistant depression. Depression and Anxiety 31: 335– 343, 2014 Ketamine had a rapid antidepressant effect in some patients with severe depression http: //www. scientificamerican. com/article/is -ketamine-next-big-depression-drug/


https: //itunes. apple. com/us/app/safe ty-plan/id 695122998? mt=8 http: //www. therapistaid. com/therapyworksheet/safety-plan/suicide/none

Mental Health & Suicide �Over 90% of suicide victims have a mental health and/or substance use disorder � 50 -75% receive inadequate treatment �Risk increased in Mood Disorders, Anxiety Disorders, PTSD, and comorbid states with medical illness �Highest in elderly � 3 rd most common cause of mortality in young adults �Independent of diagnosis, targeting and treating suicidal ideation and behaviors may have benefit.

Suicidal Continuum �Best identified before any suicidal behavior occurs. �Early identification of suicidal ideation presents the greatest opportunity to reduce the risk of suicide attempt and death. � Continuum begins with suicidal thoughts, � evolving into a wish to die, � consolidated into an intention to act, � resulting in a methodology or plan formulated to end one’s life. �The evolution of these steps can occur over minutes or years. �Each step along the continuum presents an opportunity to intervene and prevent the act of suicidal self-directed violence.
:")
Treatment Targets �Brent D et al. The Treatment of Adolescent Suicide Attempters Study (TASA): Predictors of Suicidal Events in an Open Treatment Trial J. Am. Acad. Child Adolesc. Psychiatry, 2009; 48(10): 987 -996 � suicidal ideation, � family cohesion, � sequelae of previous abuse. �“ 40% of events occurred with 4 weeks of intake: an emphasis on safety planning and increased therapeutic contact early in treatment may be warranted” �Wren et al: concept of multiple risk intervention �Safety Box concept IFEM Hong Kong

Suicide Assessment: SAFE-T

Direct Warning Signs Three signs with highest likelihood of suicidal behaviors in the near future: Suicidal communication - writing or talking about suicide, wish to die, or death (threatening to hurt or kill self)) • Seeking access or recent use of lethal means: such as weapons, medications, or other lethal means • Preparations for suicide - evidence or expression of suicide intent, and/or taking steps towards implementation of a plan. Makes arrangements to divest responsibility for dependent others (children, pets, elders), or making other preparations such as updating wills, making financial arrangements for paying bills, saying goodbye to loved ones, etc. Worse with a history of previous or multiple attempts

Suicide Risk Assessment & Action † Modifiers that increase the level of risk for suicide of any defined level : • Acute state of Substance Use: Alcohol or substance abuse history is associated with impaired judgment and may increase the severity of the suicidality and risk for suicide act • Access to means : (firearms, medications) may increase the risk for suicide act • Existence of multiple risk factors or warning signs or lack of protective factors †† Evidence of suicidal behavior warning signs in the context of denial of ideation should call for concern (e. g. , contemplation of plan with denial of thoughts or ideation)

1. Ideation Questions Example of Questions on Ideation: • “With everything that has been going on, have you been experiencing any thoughts of killing yourself? ” • When did you begin having suicidal thoughts? • Did any event (stressor) precipitate thoughts? • How often do you have thoughts of suicide? • How long do they last? • How strong are thoughts of suicide? • What is the worst they have ever been? • What do you do when you have these (suicidal) thoughts? • What did you do when they were the strongest ever? • Do thoughts occur or intensify when you drink or use drugs?

2. Intent Questions Example of Questions on Intent: • Do you wish you were dead? • Do you intend to try to kill yourself? • Do you have a plan regarding how you might kill yourself? • Have you taken any actions towards putting that plan in place? • How likely do you think it is that you will carry out your plans?
 Examples of Questions on Preparation: •")
3. Preparatory Behavior Questions (may need collateral hx) Examples of Questions on Preparation: • Do you have a plan or have you been planning to kill yourself? If so, how would you do it? Where would you do it? • Do you have the (drugs, gun, rope) that you would use? Where is it right now? • Do you have a timeline in mind for killing yourself? • Is there something (an event) that would trigger acting on the plan? • How confident are you that your plan will end your life? • What have you done to begin to carry out the plan? • Have you made other preparations (e. g. , updated life insurance, made arrangements for pets)?

Safety Plan Component of Safety Plan: The Safety Plan should consist of a written, prioritized list of coping strategies and sources of support that patients can use to alleviate a suicidal crisis. Patients are instructed first to recognize when they are in crisis (Step 1) and then to utilize Steps 2 through 5 as needed to reduce the level of suicide risk: 1. Recognizing warning signs of an impending suicidal crisis 2. Employing internal coping strategies 3. Utilizing social contacts and social settings as a means of distraction from suicidal thoughts 4. Utilizing family members or friends to help resolve the crisis 5. Contacting mental health professionals or agencies 6. Restricting access to lethal means.

Safety PLan

Suicide Focused Therapy �Suicide-focused psychotherapies that have been shown to be effective in reducing risk for repeated self-directed violence should be included in the treatment plan of patients at high risk for suicide, if the risk for suicide is not adequately addressed by psychotherapy specific to the underlying condition.

Goals of Consultation & Hospitalization �Diagnostic Clarification �Treatment initiation �Maintenance of Safety �Note Risk vs Benefit: regression, damage to therapeutic alliance

Benzodiazepines in Suicidal Risk • Use caution when prescribing benzodiazepines to patients at risk for suicide. • It is important to pay attention to the risk of disinhibition from the medication, and respiratory depression (particularly when combined with other depressants) by limiting the amount of benzodiazepines dispensed. • Avoid benzodiazepines with a short half-life and the long-term use of any benzodiazepine to minimize the risk of addiction and depressogenic effects.

Depression and Suicide in Children and Adolescents Can send home if: The patient is not imminently suicidal. The patient is in medically stable condition. The patient and the parents agree to return to the ED if suicidal intent recurs. The patient is not intoxicated, delirious, or demented. Potentially lethal means of self-harm have been removed. Treatment of underlying psychiatric diagnoses has been arranged. Acute precipitants to the crisis have been addressed and attempts have been undertaken to resolve them. The physician believes that the patient and family will follow through on treatment recommendations. The patient's caregivers and social supports are in agreement with the discharge plans.

Borderline PD �mood instability, impulsivity, aggressivity and prone to intense anger. �Tendency toward self injury. �Major risk factor for suicide. �Associated with as many as 55 % of attempted suicides. �More likely to make repeated attempts than actually complete one.

Anorexia nervosa � Refusal to maintain weight within a normal range for height and age (>15% below ideal body weight) � Fear of weight gain � Severe body image disturbance in which body image is the predominant measure of self worth with denial of the seriousness of the illness � In females, secondary amenorrhea for greater than three cycles or primary amenorrhea

Eating Disorder Questions--SCOFF 1. Do you make yourself Sick because you feel uncomfortably full? 2. Do you worry you have lost Control over how much you eat? 3. Have you recently lost more than One stone (6. 4 kg or 14 lb) in a 3 -mo period? 4. Do you believe yourself to be Fat when others say you are too thin? 5. Would you say that Food dominates your life?

Eating Disorders Complications Suicide is one of the leading causes of death for patients with anorexia.

Involuntary Admission �Involuntary hospitalization is considered when: � The patients words or behaviours suggest that they are at imminent risk of harm to themselves or others, �There is a mental health illness �Specific guidelines are governed by individual provinces/ states. �Is not a determination of competency

Questions?
- Slides: 83