Behavioral and Psychological Symptoms of Dementia An Overview

Behavioral and Psychological Symptoms of Dementia -An Overview. Seol-Heui Han Chungbuk National University Hospital

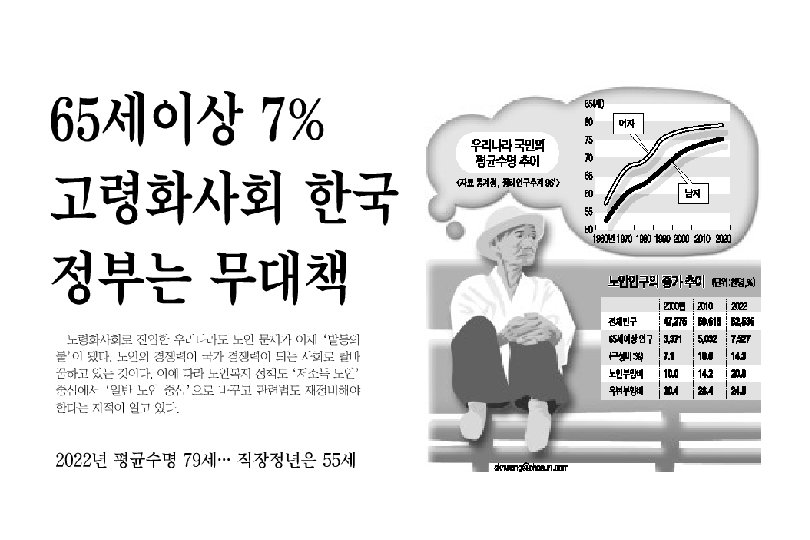
Estimations of the increasing size of the elderly population


X 2019/19

Definition of the dementia syndrome DEMENTIA v. Multiple cognitive deficits vmemory loss vaphasia vapraxia vagnosia vdisturbance in executive function v. These lead to functional decline

A, B, Cs of DEMENTIA A: Activities of daily living: ADL B: Behavioral and psychological symptoms of dementia (BPSD) C: Cognitive decline (D: Differential diagnosis) Loss of independence
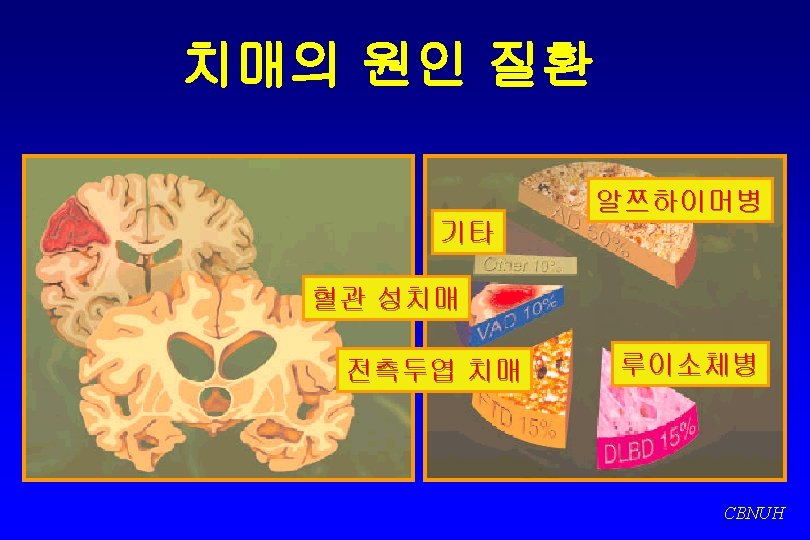

AD- the extent of the problem v. AD represents over 50% of all dementia cases v. AD prevalence doubles every 5 years after 60 years of age v. AD affects 15 million people worldwide
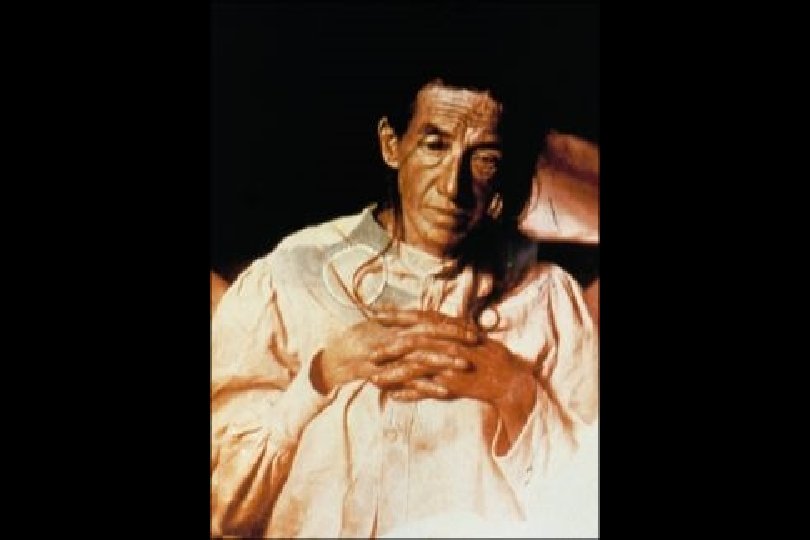
 Frau August D (F/51, 1901 -1906) vsuspiciousness of her husband vrapidly")
Alois Alzheimer (1907) Frau August D (F/51, 1901 -1906) vsuspiciousness of her husband vrapidly increasing memory impairment vno longer orient herself in her own dwelling vdragged objects here and there and hid them vbelieving that people were out to murder her vstarted to scream loudly vseems to have auditory hallucination CBNUH

AD risk and protective factors Risk factors ü Age ü Family History of AD (Apo. E-4) ü Head trauma ü Low educational level ü Environmental factors ü Down’s syndrome Protective factors ü Genetic (Apo. E-2) ü High educational level ü Long-term antiinflammatory drug use, e. g. NSAIDS ü Long-term use of estrogens (in women)
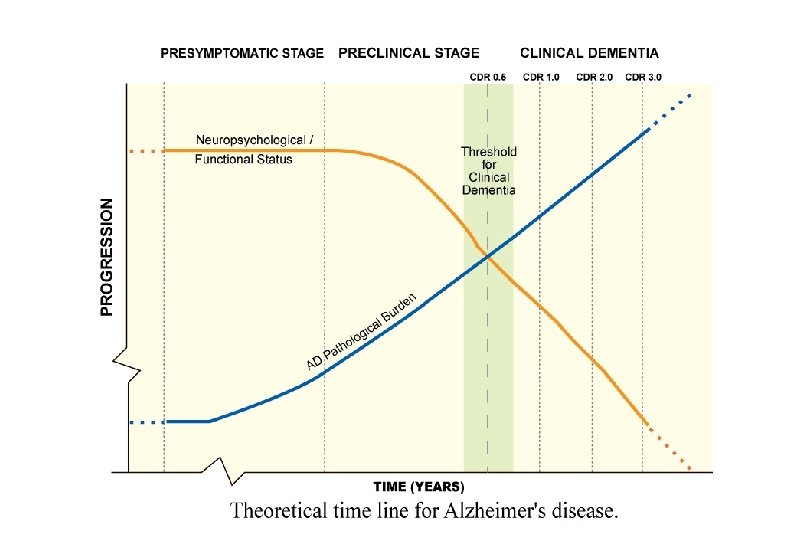

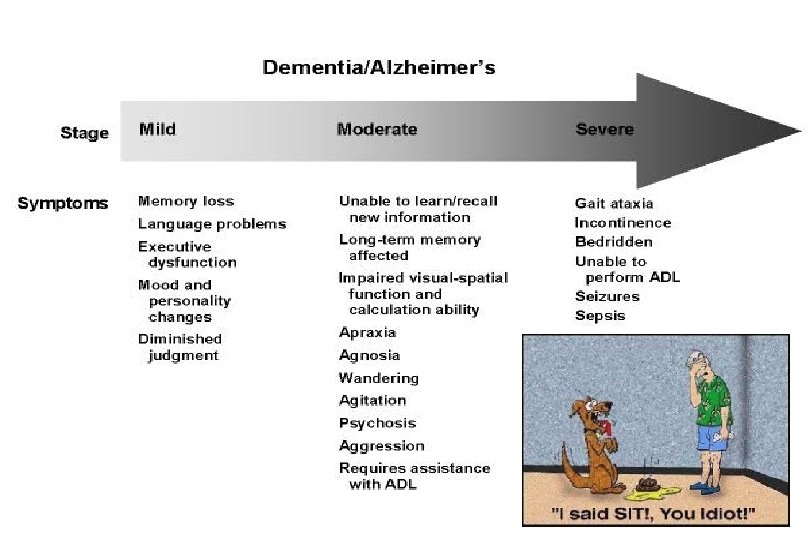
The natural progression of AD

Clinical features of AD Functional impairment ØADL ØIADL Insidious onset AD BPSD ØMood swings ØAgitation ØWandering Cognitive decline ØMemory loss ØAphasia ØApraxia ØAgnosia ØExecutive function difficulties Age over 60 years No gait difficulties IPA AD Conference, 1996

“I believe I’ve been having hallucinations, Doctor. ”

wandering

Management of severe AD v. Provision of meaningful activities v. Treatment of coexisting medical conditions v. Management of the behavioral symptoms associated with dementia

Physical aggression, delusions, wandering v. Increased hospitalization v. Premature institutionalization v. Emotional suffering for patients and caregivers v. Increased financial costs v. Excess disability

What is BPSD? v. A term used to describe a heterogeneous range of psychological reactions, psychiatric symptoms, and behaviors occurring in people with dementia of any etiology - revised definition of BPSD, IPA -

Evolution of terms v Non-cognitive symptoms of dementia v Neuropsychiatric symptoms of dementia v Psychiatric symptoms and behavioral pathology of dementia v Behavioral problems of dementia v Problem behaviors of dementia v Behavioral disturbances of dementia (BDD) v Behavioral and psychological signs and symptoms of dementia (BPSSD) v Behavioral and psychological symptoms of dementia (BPSD)

Consensus Conference on Behavioral Disturbances of Dementia v. Etiology v. Nomenclature v. Scales and measurement v. Phenomenology v. Treatment and management v. Caregivers v. Cross-cultural components

Mini Mental State Examination score AD prognosis Optimal case 25 -----------| Symptoms 20 |-----------| Diagnosis 15 |------------| Loss of functional independence 10 |----------------| Behavioral problems 5 Nursing home placement |----------------------| 0 Death 1 2 3 |---------------------4 5 6 7 8 9 Years Feidman and Gracon, 1996

The prevalence of BPSD. Reprinted with permission from Finkel, 1998

Possible causes of challenging behavior v Physical causes v Effects of medication v Impaired vision/hearing v Acute illness (UTI, URI) v Chronic illness v Emotional causes v Depression v Fear v Frustration v Embarrassment v Unable to communicate needs or articulate feelings v Environmental causes v Environment too large v Too much clutter v Excessive or too little stimulation v No orientation information or cues v Too many choices or ideas at once v Unstructured or unfamiliar environment v Task-related causes v Too complicated v Too many steps combined v Task unfamiliar; requires new learning

Diagnosis and Assessment of BPSD v. Phenomenology is the basis of diagnosis v. Direct interview v. Direct observation v. Proxy report v. Measurements and scales v. Need for accurate descriptions v. Think of physical illness v. Think of sensory impairment

Symptoms assessed at patient/relative interview Symptoms assessed by behavioral observation or by patient /relative Anxiety Aggression Depressed mood Screaming Delusions, hallucinations Restlessness Agitation Wandering Culturally-inappropriate behaviors Sexual disinhibition Cursing Shadowing

Behaviors Common to Dementia v Repetitive speech or actions v Neglect of personal hygiene and grooming v Swearing or tactlessness v Wandering v Sundowning v Shadowing v Apathy or withdrawal v Hostility or aggression v Sleep disturbances v Paranoia and suspiciousness v Delusions v Hallucinations v Decreased awareness of personal safety v Forgetting what is private behavior v Catastrophic reactions Source: ADRDA, Inc. , 1999

Variation With Type of Dementia v Visual hallucinations are more common in Dementia with Lewy bodies v Disinhibition symptoms occur early in the some of the Frontotemporal dementias v Earlier onset of behavioral symptoms has been described in Huntington’s chorea, Creutzfeldt-Jacob disease and Pick’s disease

DLB: Neurobehavioral Decline of Mervyn Peake Self-portrait Treasure Island

DLB: Neurobehavioral Decline of Mervyn Peake Suffering from visual hallucination

Five General Principles About BPSD vary from person to person. v. Loss of control is not deliberate. v. BPSD do not occur in a vacuum. v. BPSD are communications. v. Positive approaches work best.

Nueroscience
- Slides: 36