Beeldvorming en beleid bij PUL Dirk Timmerman Tom

Beeldvorming en beleid bij PUL Dirk Timmerman Tom Bourne Emma Kirk Anne Pexsters Caroline Van Holsbeke Dominique Van Schoubroeck Ben Van Calster VVOG Genk, 10 Oktober 2013 CME: This presentation is free from any commercial bias and /or promotional intent
 2% Ectopic Pregnancy (EP) 10% PUL")
Positive Pregnancy Test TVS 88% Intra-uterine Pregnancy (IUP) 2% Ectopic Pregnancy (EP) 10% PUL h. CG & Prog 0 & 48 hrs TVS Failed IUP PUL 90% EP 10%

Ultrasound in early pregnancy 1. Reliable dating of pregnancy 2. Reliable diagnosis of miscarriage 3. Pregnancy of unknown location

1. Reliable Dating US Features – Week 4 • Thickened endometrium also found in: - late luteal phase of menstrual cycle - decidual reaction with an ectopic pregnancy • Corpus luteum

US Features - Week 4 • 32 -34 days • Echogenic or trophoblastic ring Gestational sac Fluid in cavity

US Features - Week 6 • • • Embryo grows rapidly Amniotic cavity expands CRL 4 -9 mm Mean sac diameter 16 -40 mm FH clearly visible 6 weeks (42 days)

Fetal Cardiac Activity – – Earliest proof of a viable IUP Should be evident when CRL > 2 mm 5 -10% embryos 2 -4 mm have no demonstrable FH Between 5 -9 weeks there is a rapid increase in mean heart rate from 110 – 175 bpm

US Features - Week 7 • Amniotic membrane and cavity more distinct • CRL 10 -15 mm • Fetal head visible • Upper limb buds 8 w +1 (16 mm)

Robinson curve Sonar measurement of fetal crown-rump length as means of assessing maturity in first trimester pregnancy Robinson H. British Medical Journal 1973 80 patients with certain dates 214 transabd US measurements 6 -14 weeks 4, 28 -31

Background: Robinson curve • Dating not possible in very early pregnancy • CRL is often too small for gestational age

Robinson CRL curve
 with known amenorrhoea (Pexsters")
New CRL curve based on more than 3500 pregnancies (Leuven) with known amenorrhoea (Pexsters et al. UOG 2010)
 CRL (in mm) Difference (in")
GA in weeks and CRL Robinson days (in mm) CRL (in mm) Difference (in days) 5+3 3. 60 0. 35 - 3. 25 4. 56 6+3 7. 46 5. 55 - 1. 91 2. 24 7+3 12. 72 11. 94 - 0. 79 0. 78 8+3 19. 40 19. 53 0. 13 - 0. 11 9+3 27. 49 28. 31 0. 82 - 0. 62 10+3 36. 99 38. 30 1. 31 - 0. 87 11+3 47. 90 49. 48 1. 58 - 0. 94 12+3 60. 23 61. 86 1. 63 - 0. 89 13+3 73. 96 75. 44 1. 48 - 0. 73
 - The largest difference between both curves is around 6 weeks.")
Conclusion (CRL curve) - The largest difference between both curves is around 6 weeks. Our new curve is probably more reliable because of large number of patients and the use of transvaginal ultrasound. - The first trimester growth curve was extended to 5 weeks GA, which allows for a correct dating of very early pregnancies
 should now be visualised on TVS")
Ectopic pregnancy • 90% of Ectopic Pregnancies (EP) should now be visualised on TVS prior to treatment • Diagnosis should be based on the positive visualization of an adnexal mass rather than the inability to visualise an intrauterine pregnancy

Ectopic pregnancy • Tubal • Interstitial • Cervical • Caesarean section scar • Ovarian

Tubal ectopic pregnancy Empty sac Inhomogeneous mass Uterus Ectopic Ovary “Bagel sign” 20% Ectopic “Blob sign” 60%

Tubal Ectopic Pregnancy Gestational sac and embryo Visible cardiac activity Ectopic Ovary Ectopic GS, yolk sac and embryo 13% Heart actitvity 7%

2. Diagnosis of miscarriage


In the absence of both embryo and yolk sac, the FPR for miscarriage was 4. 4% when an MSD cut-off of 16 mm was used and 0. 5% for a cut-off of 20 mm.

Interobserver reproducibility 8 w +2

Interobserver variability of measurements CRL MSD CRL 1 of first 95% PI for CRL 1 MSD of first 95% PI for MSD of observer (mm) of second observer (mm) 5 [4. 5 -5. 6] 16 [13. 5 -19. 8] 6 [5. 4 -6. 7] 18 [15. 1 -22. 2] 7 [6. 3 -7. 9] 19 [16. 0 -23. 4] 10 [8. 9 -11. 2] 20 [16. 8 -24. 5] 20 [17. 9 -22. 4] 21 [17. 6 -25. 7] 30 [26. 7 -33. 5] 22 [18. 4 -26. 9] PI = prediction interval. Scans by two experienced consultants with an interest in early pregnancy ultrasound
: The Management of Early Pregnancy Loss •")
Addendum to GTG No 25 (Oct 2006): The Management of Early Pregnancy Loss • Recent research suggests that given inter-observer variability in ultrasound measurements and the greater variation in early embryonic growth than has hitherto been assumed, a more conservative approach to the diagnosis of early pregnancy loss is warranted. • The studies from Imperial College London, Queen Mary, University of London and the KU Leuven, Belgium published in the November 2011 issue of Ultrasound Obstet Gynaecol concluded that current definitions used to diagnose miscarriage could lead to an incorrect diagnosis and they call for clearer evidence based guidance on detecting miscarriage. Having carefully considered these papers, we recommend adoption of the following interim guidance with immediate effect:
: The Management of Early Pregnancy Loss •")
Addendum to GTG No 25 (Oct 2006): The Management of Early Pregnancy Loss • Ultrasound diagnosis of miscarriage should only be considered with a mean gestation sac diameter >/= 25 mm (with no obvious yolk sac), or with a fetal pole with crown rump length >/=7 mm (without evidence of fetal heart activity) • A TVS should be performed in all cases where there is any doubt about the diagnosis and/or a woman requests a repeat scan, this should be performed at an interval of at least one week from the initial scan before medical or surgical measures are undertaken for uterine evacuation. No growth in gestation sac size or CRL is strongly suggestive of a nonviable pregnancy in the absence of embryonic structures. We would add: no embryonic structure seen for an empty sac on repeat scan > 7 days later
 study Prospective: observational - consecutive cases Multicentre (8): St Thomas’s,")
Diagnosis of miscarriage (DOM) study Prospective: observational - consecutive cases Multicentre (8): St Thomas’s, Chelsea and Westminster, Northwick Park, Queen Charlottes and Chelsea, St Mary’s, Princess Anne Southampton, Genk Definitions: intrauterine pregnancies of unknown viability (PUV): Empty gestation sac, or gestation sac with a yolk sac but no embryo seen with MSD of < 30 mm. Embryo with an absent heartbeat and CRL < 8 mm Recruitment: 2925 consecutive women Reference standard: viable pregnancy at the time of first trimester screening ultrasonography at 11 -14 weeks (@ 99% reach term) Outcome measures: sensitivity, specificity, PPV and NPV with CI’s for specificity. Risk of miscarriage

Empty Gestation Sacs Diagnostic performance of MSD to predict miscarriage in pregnancies with an empty GS USA (Spec 96 CI 94 -98 ROM 83) Old UK/AUS/NZ (Spec 99, 5 CI 98 -99. 9 ROM 93) New UK/AUS/NZ/USA (Spec 100, CI 99 -100 ROM 98)

Empty Gestation Sacs Sensitivity and specificity by MSD cut-off for pregnancies with empty GS. 95% CIs 96% at 16 99. 5% at 20 100% at 25 Specificity Sensitivity

Sensitivity and specificity by CRL cut-off for pregnancies with embryo, but no FH (95% CIs) 95% at 5 97% at 6 99% at 7 Specificity Sensitivity
 • Positive pregnancy test (h. CG > 5")
3. Pregnancy of Unknown Location (PUL) • Positive pregnancy test (h. CG > 5 IU/L) • No sign of intrauterine or extrauterine pregnancy at TVS • No products of conception visualised at TVS
, Emma Kirk, Cecilia Bottomley, Yazan")
PUL: London – Leuven studies George Condous (now Sydney), Emma Kirk, Cecilia Bottomley, Yazan Abdallah, Jessica Preisler, Tom Bourne Ben Van Calster, Sabine Van Huffel, Kirsten Van Hoorde, Anne Pexsters, Dominique Van Schoubroeck, Caroline Van Holsbeke, Jan Deprest, Dirk Timmerman

PUL clinical issues • Ideal rate of PULs? • Role of single measurements of h. CG and progesterone? • Can we manage PULs on single visit? • Change in serum h. CG over time better than single measurements of h. CG and progesterone? • Can we develop mathematical models to be used in clinical setting to manage PULs?

Rate of PULs • Quality of scanning is key - Detection of early IUPs & ectopic pregnancy using TVS increases with experience - PUL rates should be < 15%
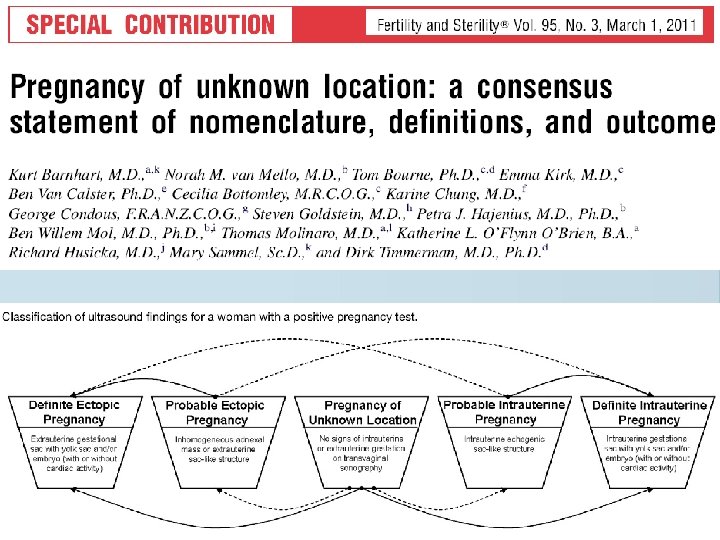

Classification of final outcomes of PUL

PULs: low risk of ectopic pregnancy • Expectant management safe • Outpatient basis • Reduce need for unnecessary intervention

‘PUL and HCG 1000 IU/L, then laparoscopy’ Progesterone nmol/L + Miscarriage + Intrauterine pregnancy + Ectopic pregnancy h. CG

Single hormonal markers Single hormone measurement 0 h PUL outcome Area Under ROC Curve Sensitivity Specificity Prog < 20 nmol/L Failing PUL 0. 952 87. 2% 89. 6% h. CG > 1000 IU/L Ectopic 0. 666 21. 6% 87. 3% h. CG > 1500 IU/L Ectopic 0. 666 18. 9% 93. 4% h. CG > 2000 IU/L Ectopic 0. 666 13. 5% 95. 2% Condous et al, Hum Reprod 2004; Ultrasound Obstet Gynecol 2005

Single visit strategy • Single measurements of progesterone can predict viability, but neither h. CG nor progesterone can locate the pregnancy • A ‘single visit strategy’ can eliminate 85% of non-ectopic pregnancies out the system • 67% of the ectopic pregnancies are not adequately followed Condous et al, Int’l J Gynaecol Obstet 2004 Condous et al, Human Reproduction 2005

h. CG ratio h. CG 48 hr h. CG 0 hr

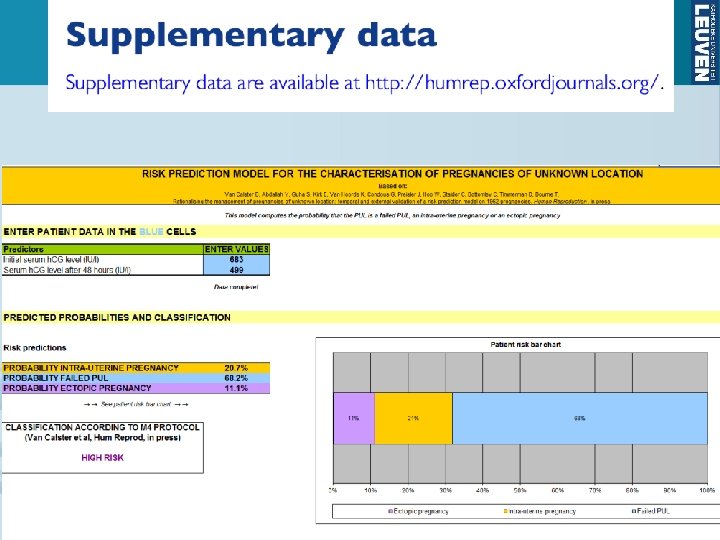
h. CG ratio vs. probability of PUL outcome h. CG 0 h 1000 IU/L h. CG 48 h 1100 2000 IU/L 500 IU/L h. CG ratio = 1. 1 2 0. 5

Rules for h. CG ratio in PUL • If h. CG ratio 0. 8, then a miscarriage is likely • If 0. 8 < h. CG ratio 1. 66, there is a high risk of ectopic pregnancy • If h. CG ratio > 1. 66, then an ongoing intrauterine pregnancy is likely

Mathematical Models Model M 1 h. CG ratio (h. CG 48 hr/h. CG 0 hr) Model M 2 log progesterone average Model M 3 Age log progesterone average h. CG ratio Model M 4 h. CG ratio log average of the two h. CG levels Condous et al, Hum Reprod 2004 Condous et al, UOG 2007 Van Calster et al, AIM 2009

Detection rate of ectopic pregnancy in PUL § Single h. CG measurement: 30 % § Single h. CG and progesterone: 50 % § HCG ratio: 75 % § Subjective assessment : § Logistic regression model M 4: 25 – 60 % 88 %

astraia Gyn ultrasound Chris Harris

NIUP IPUVI PUL Miscarriage Ectopic

Chance of diagnostic scan 5 wks 7 wks

1. Can we accurately define a group of low-risk PUL in order to safely reduce follow-up for these pregnancies and allocate resources to PUL at increased risk? § Select a group of PUL as being at low risk avoid ectopics in this group: high NPV, high sensitivity for EP 2. Externally validate the PUL prediction model M 4

Study design and setting § Multi-centre, observational, diagnostic accuracy study § 5 London university hospitals § Retrospective internal validation on data from St. George’s (SGH) § Prospective external validation on data from § § Queen Charlotte’s and Chelsea Hospital (QCH) Chelsea and Westminster Hospital (CWH) West Middlesex Hospital (WMH) St. Mary’s Hospital (SMH) § Aim: avoid giving reduced follow-up to ectopics

IPULA study using M 4 h. CG at day 0 Woman with PUL Yes High risk h. CG at 48 h Apply M 4: Estimated probability of ectopic ≥ 5%? Yes No Probability of IUP > probability of Failed? Low risk IUP Repeat scan and h. CG in 48 h Low risk Follow-up scan in 2 weeks No Low risk Failed PUL Follow-up UPT in 2 weeks

Data SGH; n = 1341 Total n = 1962 QCH; n = 309 CWH; n = 130 WMH; n = 101 SMH; n = 81 Failed PUL 47 to 70% IUP 17 to 41% Ectopic 8 to 16% External; n = 621
 External validation (QCH, CWH, WMH,")
PUL triage by outcome: cross-tabulation Prediction Internal validation (SGH) External validation (QCH, CWH, WMH, SMH) High risk Low risk IUP Low risk failed Failed PUL IUP True outcome Ectopic
 External data 11")
Ectopics and interventions Low risk High risk SGH 17 94 (85%) External data 11 81 (88%) List of 11 false negatives h. CG Day 0 h. CG ratio Prob ectopic Intervention 62 0. 34 <0. 1% Expectant 78 2. 88 <0. 1% Expectant 112 2. 04 4. 0% Expectant 147 2. 21 1. 1% MTX 168 3. 15 <0. 1% Expectant 170 0. 39 <0. 1% MTX 225 0. 59 0. 8% Expectant 829 2. 02 4. 4% MTX 911 2. 29 0. 5% Laparoscopy 1220 3. 57 <0. 1% Salpingotomy 1707 0. 51 2. 6% Laparoscopy

PUL triage by M 4: High risk area

IPULA: International PUL Analysis Multicentric prospective study to test the diagnostic performance of new models Tom Bourne, George Condous, Emma Kirk, Arnaud Installé, Ben Van Calster, Dirk Timmerman Interested centers: IPULA. study@gmail. com

IPULA in Clinical Data Miner Arnaud Installé

The care of any pregnancy at any gestation should be to the same standard • Appropriate training and equipment • Senior input • Compassion • Rigorous diagnostic criteria • Cut-off values need to be harmonised • Influence of gestation must be accounted for • Stipulate ultrasound findings on repeat scans to define miscarriage • Manage patient expectation+4 on repeat scans – 10 rules and models to do this • Remember expectant management is unlikely to be harmful. Intervention certainly can be. • Future will be individualised risk/diagnosis • “FIRST DO NO HARM”

Conclusies • Naarmate meer vrouwen zich vroeger in de zwangerschap aanbieden voor een echografie, stijgt diagnose van PUL • Betere referentiecurves zullen accurate dating bevorderen • Betere richtlijnen en deskundig gebruik van echografie kan het aantal foutieve diagnosen van miskraam +/- elimineren • Echocursus en training zijn nodig voor vroege zwangerschap • Onderzoek over echo in vroege zwagerschap is nodig
- Slides: 60