BDS 3 Orthodontics COMMONWEALTH OF AUSTRALIA Copyright Regulations

BDS 3 Orthodontics

COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING This material has been reproduced and communicated to you by or on behalf of The University of Adelaide under Part VB of the Copyright Act 1968 (the Act). The material in this communication may be subject to copyright under the Act. Any further reproduction or communication of this material by you may be the subject of copyright protection under the Act. The AUDSS assumes no responsibility or liability for any information, materials or other content provided by any of our student lecturers. All content is viewed and used by you at your own risk and we do not warrant the accuracy or reliability of any of the lecture material. The views expressed are those of the individual contributors and not necessarily those of the AUDSS of Adelaide School of Dentistry. Do not remove this notice.

Overview ■ Measuring growth and development ■ Factors influencing growth and development ■ Cranio-facial growth and development ■ Apical Base ■ Dental Arch development ■ Changes in 6 -12 y. o. tooth development ■ Classification of malocclusion

Methods used to study Growth and Development Direct • Anatomic • Maturity Indicators • Radiographs • Metallic Implants (Bjork) • 3 D imaging

Indirect Measurements ■ Vital Staining: incorporates into biologically active tissue ■ Histology, light and electron microscopy ■ Cross-sectional/ Longditudinal studies

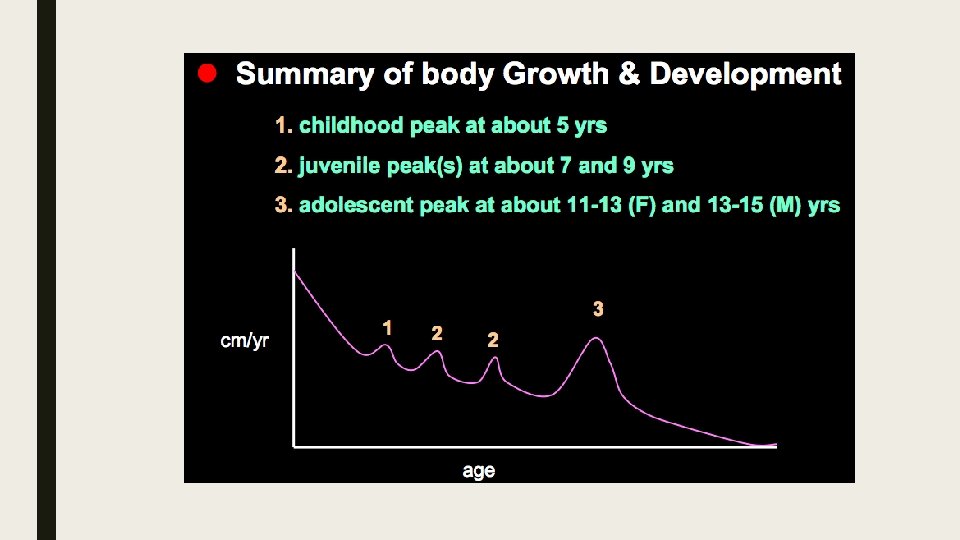
Growth and Development ■ Scammon’s Curve ■ Stylized distant curves for lymphoid, neural, general and genital tissues
 ■ Endomorphy = round and stocky ■ Mesomorphy = average ■")
Body Types (Sheldon) ■ Endomorphy = round and stocky ■ Mesomorphy = average ■ Ectomorphy = long and thin

Craniofacial Growth ■ Cranium Changes ■ Depth>Width>Height ■ Facial Changes ■ Height>Depth>Width

Craniofacial Growth

Factors influencing growth and development ① Genetics ② Hormones ③ Secular Trends ④ Disease ⑤ Season/Climate ⑥ Neural ⑦ Nutrition (homeorhesis) ⑧ Socio-economic Status ⑨ Exercise ⑩ Emotion
 • Spheno-ethmoidal synchondrosis (closes by")
Cranial Base • Fronto-ethmoidal synchondrosis (closes by 2 years) • Spheno-ethmoidal synchondrosis (closes by 7 years) • Inter-sphenoidal synchondrosis (closes by 1 year) • Spheno-occipital synchondrosis (closes by 14 -25 ? years)

Mandible ■ Develops as membrane bone in two halves around meckel’s cartilage ■ The symphysis unites within 12 months after birth ■ The gonial angle and coronoid process increase in size and largely depend on muscle activity ■ The mandible grows down and forward from the cranial base but the role of the condyle is still debated ■ Dental arch formation is mostly up and forward with space being produced distally by alveolar growth and resorption of the anterior border of the ramus
 is due to tooth eruption and")
Orthodontic Significance ■ Vertical face height increase (growth) is due to tooth eruption and alveolar bone production ■ Poor dento-alveolar facial patterns rarely improve by themselves

Apical Base Lundstrom ■ Theoretical/conceptual interface between the Mx/Md and their respective alveolar processes ■ Contain the tooth roots (after eruption) and tooth crown (pre-eruption) ■ Represents limits for tooth movements ■ Varies between individuals ■ Independent of tooth size Solow ■ Dento-alveolar Compensation

Crowding ■ Primary: Tooth size compared to apical base dimensions ■ Secondary: Environmental influences ■ Tertiary: Late facial growth (Van Der Linden)

Influences on tooth eruption Accelerating • Unusual: hyperthyroidism, hyperpituitarism, Turner’s Syndrome • Premature loss of primary teeth (within 6 to 12 months) • Familial Delaying General • Familial • Hypothyroidism, hypopituitarism • Cleidocranial dysostosis, achondroplasia, down syndrome • Hypovitaminosis (A and D) • Amelogenesis imperfecta Local • Abnormal tooth position • Ectopic eruption • Lack of arch space • Early loss of primary teeth (>2 years) • Ankylosis • Retained tooth roots • Trauma • Supernumeraries, tumors and cysts • Fibrous gingivae, sclerotic bone, primary failure of eruption
 ■ Most teeth erupt with 2/3 or")
Dental Age Emergence Age (Gates NSW 1964) ■ Most teeth erupt with 2/3 or 3/4 root formed Maturation stages (Nolla, Hotz, Fanning and Moorees)

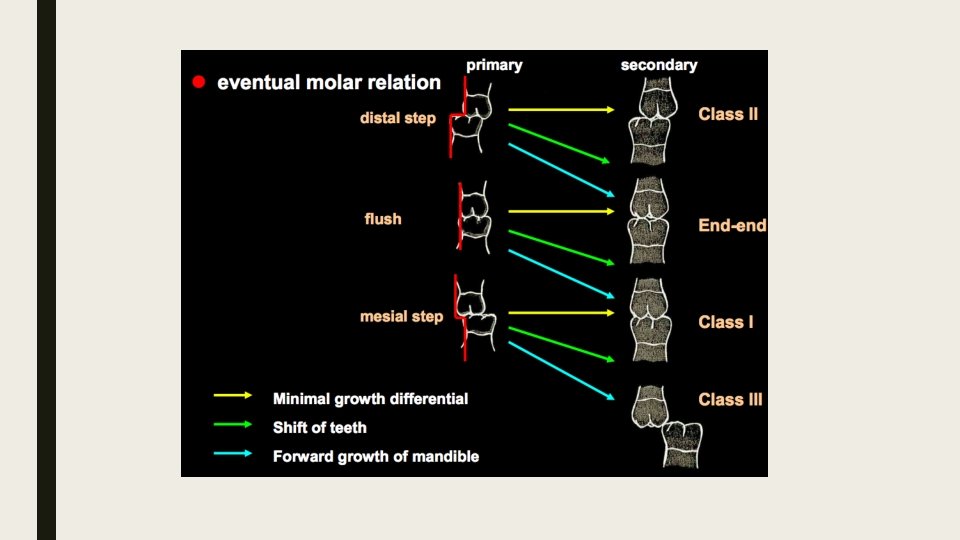
Dental Arch Development ■ ■ ■ Natal teeth: present at birth Primate spaces Terminal Plane (Friel) Flush (80%) Mesial Step (6%) Distal Step (14%) Interdental Spaces: Baume Type 1 (Spaced) Baume Type 2 (Closed)

6 -12 y. o. ■ Mixed dentition stage ■ Incisor Liability/ Negative leeway (Mx: -7. 42 mm, Md: 5. 14 mm) ■ Broadbent’s Ugly Duckling Stage
 ■ Mixed dentition stage ■ Arch width changes")
Dental arch development (6 -12 yrs) ■ Mixed dentition stage ■ Arch width changes – Increased inter-canine and inter-molar widths – Once canines erupt, decr inter-canine width (esp in Md) ■ Mx arch depth changes – Increases as incisors erupt – Once incisors erupt, decreased arch depth ■ Md arch depth – Little change from 6 -12 yo, then decreases (esp as Es exfoliate)
 ■ Only small increases in arch width (except inter-canine")
Dental arch development (12 -adult) ■ Only small increases in arch width (except inter-canine width in Md stable or reduces) ■ Decreased arch depth, esp in Md due to: – Incisor uprighting (late facial growth rotation, tertiary crowding) – Possible influence from 8 s and mesial tooth movement ■ Third molars – Highly variable, radiographic crypt usually from 8 yo (13 -14 yo if late)
 ■ Interdental and primate spaces (Baume")
Factors affecting dental arch alignment – assisting (8) ■ Interdental and primate spaces (Baume Type 1 - spaced deciduous arch) ■ Leeway space of Nance (large CDE size cf. 345) ■ Bradycephalic/euryprosopic face types (short, broad faces) ■ Large apical base and small teeth ■ Permanent incisors erupt more proclined than their primary successors increases arch depth ■ Increased arch width (inter-canine width most important) ■ Space created posteriorly for 7 s to erupt (Mx tuberosity apposition, Md – anterior border of ramus resorption) ■ Soft tissues: Normal lip and tongue function
 ■ Lack of interdental spacing (Baume type II) ■ Small")
Factors opposing alignment (11) ■ Lack of interdental spacing (Baume type II) ■ Small leeway space of Nance, flush terminal plane requiring molar adjustment (to class 1) ■ Inconsistent inter-canine width changes ■ Dolicocephalic/leptoprosopic OR bradycephalic with deep OB ■ Continual arch depth reduction after permanent incisors erupt ■ Incisor liability (1 s and 2 s larger than As and Bs) ■ Small apical base with large teeth (primary crowding) ■ Basal arch width is established early (about 6 yo) – but some Mx expansion may be possible before suture fusion ■ Containment of Md arch ■ Adverse soft tissue pattern (oral habits, high lip tone strong retroclining force on teeth)
 ■")
Classification of Malocclusion ■ Angle’s - incl modifications (Dewey-Anderson, Ackerman-Proffit, British Standard/Eastman system) ■ Lischer’s system –suffix ‘-version’ indicates direction of malposition (in relation to the line of occlusion) – Trans-version (tooth in the wrong order)

Important things to know about malocclusion ■ Different classification systems and their advantages + limitations (esp limitations of Angle’s classification) ■ Facial and dental features associated with different types of malocclusion (eg. Class 2 Div 1: convex facial profile + AOB maybe if mouthbreathing Hx dolicocephalic) ■ Class 3 – always check for functional shift (pseudo-class 3) from premature contacts/occlusal interferences ■ ‘Class 3 Subdivision’ – implies one side is class 1 ■ ‘Bimaxillary protrusion’ – Class 1 C+M but proclined incisors relative to apical base ■ Consider if dento-alveolar and/or skeletal in origin – lat ceph helps assess skeletal relationship

Angle’s classification ■ Adv – Simple to use – Internationally recognised – Provides a broad separation into visually distinct dental or occlusal patterns ■ Disadv – Does not specify magnitude/severity – Does not indicate aetiology clearly (eg. is C 2 D 1 due to retrognathic Md, protrusive Mx or both? ) – Does not encompass all dento-facial variation, only sagittal plane considered (not vertical or transverse problems, or asymmetry) – Dental patterns only, not skeletal or facial patterns – Static occlusion only

Ackerman-Proffit system • Can be used to help form a problem list • Continue to use it in BDS 4

Aesthetics + Nose, Lip and Chin Growth ■ Aesthetics = facial harmony, well balanced, symmetry, cultural and individual variability in perception of aesthetics ■ A well-balanced profile before puberty may deteriorate ■ Lips: lip line drops and lips lose tone with age ■ Chin growth: Bjork’s rotations

Few general principles to aesthetics ■ Good facial skeletal proportion and balance ■ Teeth relatively well-aligned (not overly protrusive) ■ Chin and lips mostly lie on a straight line ■ Smile aesthetics: – Consonant smile – curve of Mx 3 -3 parallels curve of lower lip – Gingival display (decreases with age) – Incisal display – Buccal corridor ■ Relatively straight profile ■ Smile aesthetics depends on: tooth alignment, tooth angulation and smile line

Questions: List five general factors and five local factors which cause tooth emergence to be delayed Write down the factors which oppose arch alignment Circle the Nolla Stage which corresponds to 2/3 of root formation? 0 1 2 3 4 5 6 7 Write down dental and facial features which characterise Class II, Div 1 subdivision Ectomorph, Consonant smile, Leptoprosopic 8 9 10

What is meant by negative leeway space? Part 1: what are the 5 factors which are considered in the Ackermann-proffit classification system? Part 2: illustrate the difference with Angle’s Classification Why is skeletal age estimates important for treatment planning in orthodontics Angle’s classification is widely used, but has its limitations and is sometimes difficult to apply. What factors should be considered prior to applying Angle’s classification system? Describe the Bolton’s analysis as it was performed during the learning laboratories Define the following term:

Cases: You need to list the problems, justify why they are a problem and provide a list of further information required and justify why you would need it. The second part of the question revolves around addressing the final question of the paragraph (ie. “what are the features of his occlusion? ”) 1) 12 year old male. Retroclined incisors, 100% overbite. “gums behind upper incisors get sore after eating” (complete deep bite with palate). Crowded lower incisors. What are the features of his occlusion?
 10 year old male. Can’t eat properly. Biting on back teeth for apples.")
2) 10 year old male. Can’t eat properly. Biting on back teeth for apples. Breathing issues. Was advised to get surgery 4 years ago related to breathing issues. Parent’s declined the surgery treatment, but now want to reconsider. The parents want to know if the treatment can still be considered and want to know about his dento-facial growth in the last 4 years.
 17 year old female. Concerned about lower teeth tilting backwards. Chin looked larger")
3) 17 year old female. Concerned about lower teeth tilting backwards. Chin looked larger on profile. She wanted to be a hygienist. “teeth had changed a lot in last 5 years”. What would you tell her?
.")
References: PROFFIT, W. R. , FIELDS, H. W. , & SARVER, D. M. (2007). Contemporary orthodontics. St. Louis, Mosby Elsevier. JAWAD, Z. , BATES, C. , HODGE, T. (2015). Who needs orthodontic treatment? Who gets it? And who wants it? Brittish Dental Journal 218; 99 -103
- Slides: 38