Basilic Cephalic Right Heart Catheterization Edo Kaluski MD

Basilic & Cephalic Right Heart Catheterization Edo Kaluski MD, FACC, FSCAI Director of Cath Lab & Interventional Cardiology RPH & Guthrie Health System Professor of Medicine at Rutgers NJMS

Edo Kaluski MD, FACC, FESC, FSCAI I have no relevant financial relationships relevant to this presentation Speaker for: Amgen, Zoll, Astra. Zeneca, DSI, Janssen Research support grants: Janssen, Astra. Zeneca,

1: The Total Forearm Approach
 1. Trans-radial and trans-ulnar interventions. 2. Trans-basilic")
Total Forearm Approach Mastering: (Patient centered approach) 1. Trans-radial and trans-ulnar interventions. 2. Trans-basilic / cephalic vein RHC interventions 3. Right and left radial / ulnar approach to perform VG, LIMA, RIMA and peripheral interventions.

Why Bother with basilic-cephalic RHC ? 1. ↑Patient convenience, comfort & safety 2. ↑ Cath lab efficiency 3. ↓RHC related bleeding. (When wrist diagnostic or interventional procedures are done anticoagulation is used) 4. Facilitate other procedures from the forearm (PICC line, TVP, Biopsy)

2. Anatomy
 •")
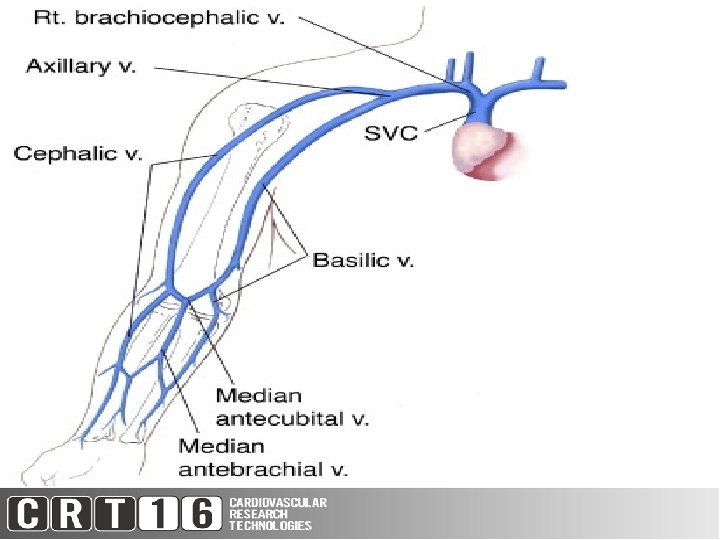
2 1 3 4 • Whether the nurse got the • Basilic (1) • Cephalic (2) • Median antecubital (3) • Median antebrachial (4)

3. Equipment

Equipment List 1. 20 G Angiocath / 21 G Needle 2. Baby Swan (with or without Thermodilution) 3. 5 F sheath 7 -11 cm* (Merit 5 F Radial Sheath & 0. 018” 45 cm wire) 4. 0. 014” HTF coronary wire – for difficult anatomy 5. Tegaderm 6. Ultrasound (rarely needed) & tourniquet

5 F 7 -11 cm Radial Sheath Cost 34$

Edwards 5 F TS 105 FS Arrow 4 F AI-017122 Arrow 5 F AI-017124 110 cm Cost 93$ Cost 65$
 • • Inability")
Limitation of the Edwards 5 F Thermodilution (TS 105 F 5) • • Inability to draw back Dampening of pressures Inability to pass wire Cost (93$ versus 65$)
 • Not thermodilution • Latex containing")
Limitation of the Arrow 5 F (AI 07124) • Not thermodilution • Latex containing • Small balloon 0. 75 ml (may not optimally wedge)
 Will not wedge")
Non-Balloon Tipped (4 F Pigtail or MP 100 -125 cm ) Will not wedge & not provide PCWP & PVR Will provide Fick CO/CI, PAP Low cost Conventional wires From left antecubital or tall subjects use 125 cm catheters. • ≥ 4 French • • •

4. Arm Preparation
 Holding Area RN inserts Angiocath in Antecubital Vein & Arm Prepped. Radial Ulnar")
1) Holding Area RN inserts Angiocath in Antecubital Vein & Arm Prepped. Radial Ulnar site Basilic Cephalic site

Ultrasound Guidance is Rarely Needed

Ideal Vein for ultrasound guidance Medial Antecubital Fossae • ≥ 3 mm in Diameter, ≤ 1 cm in depth, 3 cm long § <3 mm diameter 56% success § >6 mm 92% success >1. 6 cm depth predicts failure Avoid veins adjacent to nerves or arteries

Ultrasound guidance • Tie a tourniquet. Locate the vein with U/S. Compression test (may use Doppler to avoid arteries) • Estimate depth • Local anesthetic. • Puncture skin at 45 degrees with needle perpendicular top probe • Identify needle tip and advance towards the vein • Confirm tenting & penetration, do a wiggle under U/S • Position needle more perpendicular to vein advance wire
 Lidocaine SC to radial/ulnar and antecubital site 3) Exchange Angio-cath to 5 F")
2) Lidocaine SC to radial/ulnar and antecubital site 3) Exchange Angio-cath to 5 F Radial Sheath Over. 018” Wire 45 cm wire & Secure with Tegaderm 4) Flush sheath via side-port or with dilator via central lumen Basilic Cephalic Site 5 F Radial Ulnar site (4 F)
")
Flushing Sheath With Dilator (No backflow from sheath sidearm)

5. Step by step approach

Advance Baby-Swan 30 -35 cm into the Radial Sheath with deflated balloon (watch for resistance) Resistance? Advance a BMW wire through the sheath under fluoro Once in RA advance the “baby swan over it.

Advance without balloon inflation 30 -35 cm Baby swan tip

Optional injection via Baby Swan RIJ Cephailic V. Basilic V. Axillary V SVC
")
Perform optional injection via Baby Swan (conventional anatomy)
")
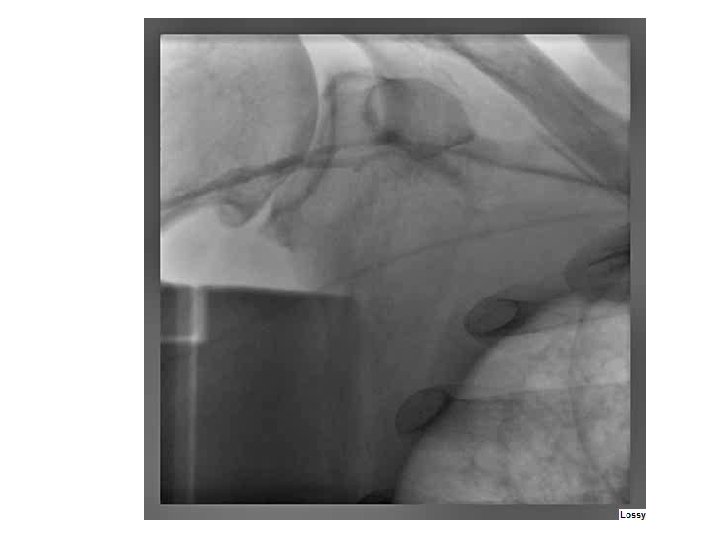
basilic & cephalic communicating directly with SCV (no Axillary vein)

Cephalic duplication & stenosis

Inflate balloon when in Axillary Vein

Troubles……resistance to advancing PAC 1. BMW wire with 1 -2 cm 45 degree angle tip 2. Deep breath 3. Contrast injections 4. NTG IV 5. Consider alternative approach

Troubles……Resistance
")
Optimal Wedging (0. 75 ml balloon)

Optimal Wedging

6. Post-procedural management

7. Complications
 • Bleeding vascular")
Issues & Complications • Arterial access (instead of venous…. most common) • Bleeding vascular • Arrhythmia, infection, air emboli (like any RHC) • ICD /CRT lead tangling, tethering & knotting • Side-port backflow (use dilator to flush) • Venous injury and thrombosis (unknown) • Incomplete study (exceedingly rare!!!) • Catheter entrapment

8. Limitations

Limitations 1. 2. 3. 4. 5. 6. Optimal wedging Pressure dampening Catheter length (110 cm) Issues with venous access (use ultrasound) Unusual venous anatomy Occlusive devices, electrodes etc.

9. Contraindications

Contraindications 1. SVC obstruction 2. Limited limb (LN dissection / mastectomy lymphedema / absent or occluded aertery) / RT 3. EP devices / equipment in SVC 4. Anomalous venous return 5. Prior brachial cut-down or surgery or burn 6. No visible or accessible veins

10. Conclusions
")
1. Basilic /Cephalic RHC Is great for our patients (safe, convenient and easy)

2. It’s a great addition to wristbased procedures.

3. It can be easily taught and incorporated into your practice.

Thank You For Your Attention! Next time before you go femoral remember: that there at least 2 sides to every story ……and every wrist…and numerous antecubital veins to choose from.
- Slides: 47