Basic Neurovascular Anatomy and Differences between the Arteries

Basic Neurovascular Anatomy and Differences between the Arteries What the cardiologist needs to know Before becoming stroke interventionalists

Disclosure Statement of Financial Interest Within the past 12 months, I or my spouse/partner have had a financial interest/arrangement or affiliation with the organization(s) listed below. Affiliation/Financial Relationship Consulting Fees/Honoraria Company Cordis, Boston Scientific, Abbott Vascular Medrad Inc. , Access Closure Major Stock Shareholder/Equity Royalty Income tech. Northwind inc , Boston Scientific , Neuro Intervention Covidian Inc. , Setagon

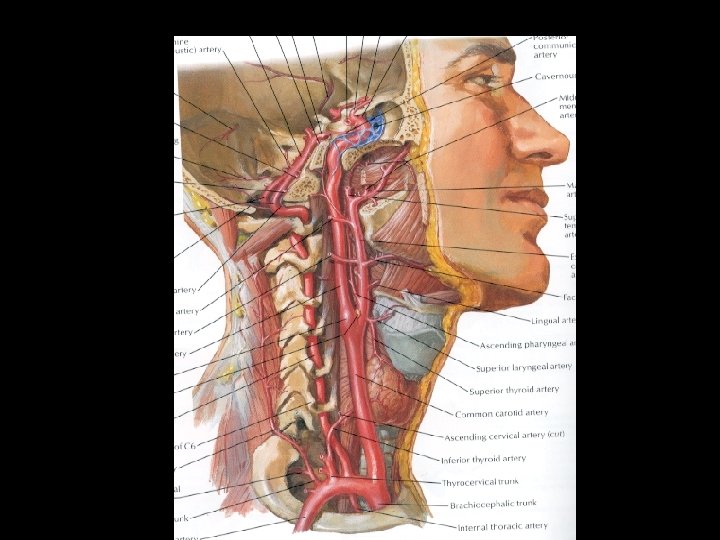
Procedure Carotid & Vertebral Angiography 1. Define aortic arch 15 -25 cc/15 cc/sec (5 Fr pig tail) 2. Type I arch JR 4 or HN 1 (5 Fr) Type III Arch; may need Simmons II, I, HN 5, 3. Catheterize prox common carotid (avoid manipulation) 4. Vertebral - selective vs non-selective (if selective, keep cath proximal) AR 2

Catheter configuration - anterior-superior designs

Simmons catheter - complex curves

Thyrocervical Trunk Note inferior thyroid branch (C 5 ant spinal art collateral


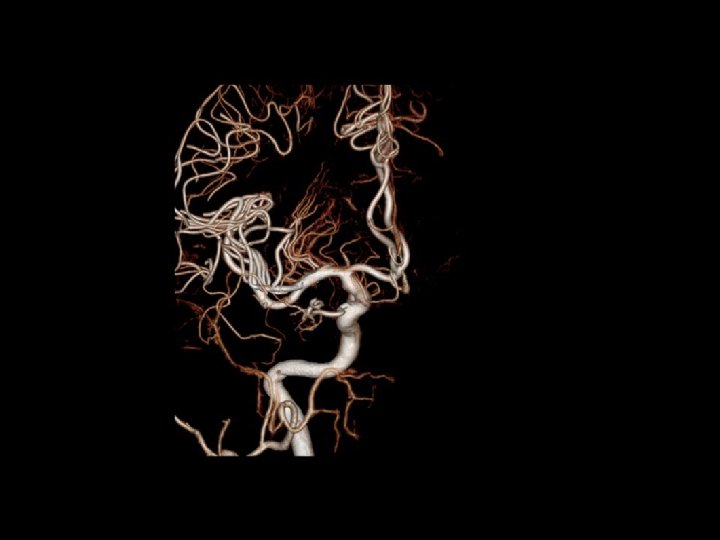
Note calcified Vertebrals and extensive collaterals in Vascular Malformation

How important is the External Carotid ?

Plaque Shift with occlusion of the External Carotid

External Occipital is only supply for Vertebral Basilar flow Basilar Infarct post procedure CEA

Stent with CAS has territorial increased risk. Why ?

Complex type 3 arch Deep seated innominate may be too difficult. Can be done but may not be worth the risk

PROBLEMS of the aortic arch Complexities of the aortic are responsible for almost all technical failures Ideal Trouble More Trouble

Shower Emboli Diffusion weighted

Diffusion Weighted MRI We are not capturing paritcles less than 100 u Before After CAS these silent ischemic embolic lesions can’t be good And long term could become a major issue

Percutaneous cervical approach and closing for carotid artery stenting N = 191 Markatis et al 2009

Remove wire, filter to internal carotid followed by pre dil and stent
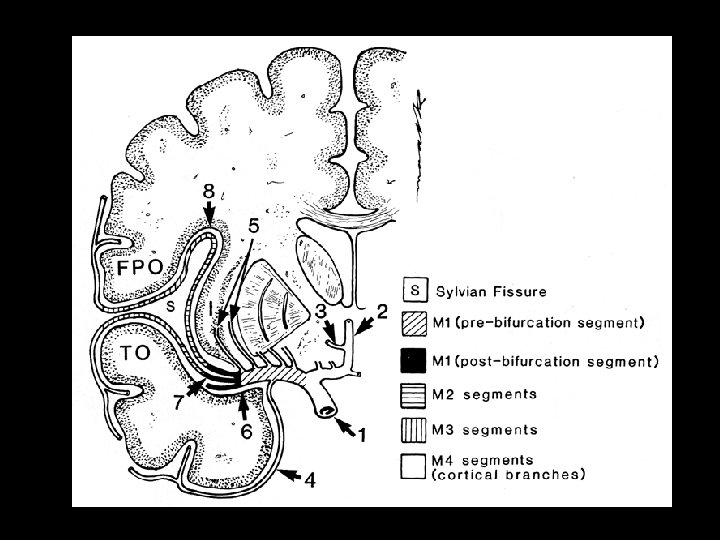
 Lateral Lenticulostriates M 3")
Middle Cerebral Artery Anterior - MCA Collosalmarginal Pericollosal (M 1) Lateral Lenticulostriates M 3 MCA M 2 MCA Genu M 1 MCA A 2 ACA A 1 ACA

Anterior Cerebral Circulation Lateral View
 Posterior thalamoperforating")
1. 2. 3. 4. 5. 6. 7. 8. Anterior thalamoperforating arteries (PCOM) Posterior thalamoperforating arteries and thalamogeniculate arteries (P 1) Medial posterior choroidal artery Lateral posterior choroidal artery Anterior temporal artery Posterior temporal artery Parietooccipital artery Calcarine artery
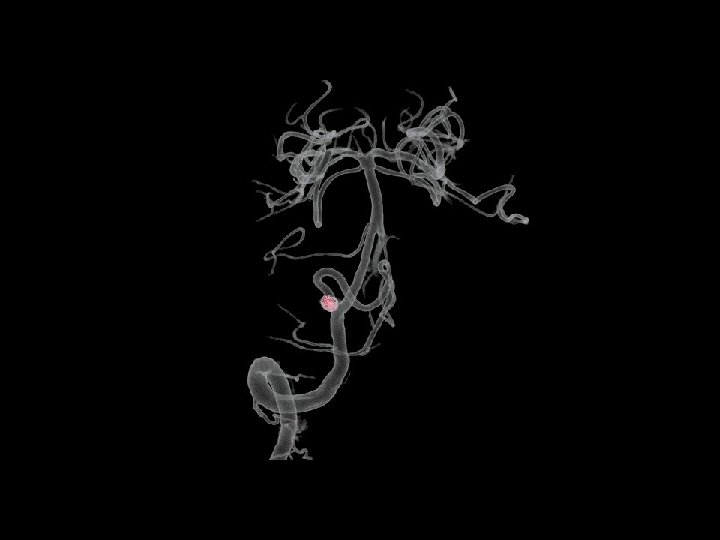

Segmental diffuse atherosclerotic change Note PICA occlusions

Segmental diffuse atherosclerotic change Note PICA occlusions

Venous Anatomy

Sagittal sinus thrombosis Collateralizing venous pattern

CT - Acute Right Hemispheric Stroke e CT-Negative? CTA-MCA Occlusive MCA no flow distribution CT-Perfusion

Collaterals Thalomostriates Infarct AVOID HEMORRHAGIC TRANSFORMATION

60 year old woman with recurrent left hemispheric TIA’s Critical L ICA stenosis Pre-dilation Post stent M 1 MCA Occlusion MCA stent 90 min post L MCA occlusion
- Slides: 32