BASIC LIFE SUPPORT Dr Negoita Silvius Elias Hospital

BASIC LIFE SUPPORT Dr. Negoita Silvius Elias Hospital, Bucharest November 2018

WHY?

Who care?
 in the United States")
Epidemiology • The exact incidence of sudden cardiac arrest (SCA) in the United States is unknown, but estimates vary from 180, 000 to over 450, 000 • In North America and Europe, the estimated incidence falls between 50 to 100 per 100, 000 in the general population. • The most common etiology of SCA is ischemic cardiovascular disease resulting in the development of lethal arrhythmias. • Resuscitation is attempted in up to two-thirds of people who sustain SCA.
, electrical defibrillation, and other advanced")
Survival • Despite the development of cardiopulmonary resuscitation (CPR), electrical defibrillation, and other advanced resuscitative techniques over the past 50 years, survival rates for SCA remain low. • In the out-of-hospital setting, studies have reported survival rates of 1 to 6 percent. Survival-to-hospital discharge from out-of-hospital SCA reported 5 to 10 percent survival among those treated by emergency medical services (EMS) and 15 percent survival when the underlying rhythm disturbance was ventricular fibrillation (VF). In-hospital SCA reported a 17 percent survival to discharge. • While early, properly performed CPR improves outcomes, not performing CPR or low-quality performance are important factors contributing to poor outcomes. Multiple studies assessing both in-hospital and prehospital performance of CPR have shown that trained health care providers consistently fail to meet basic life support guidelines.

Algorithm

Cardiac arrest • Shockable 1. Ventricular fibrillation 2. Pulseless ventricular tachycardia • Non–shockable 1. Asystole 2. Pulseless electrical activity

Important concepts • In most communities, the median time from emergency call to emergency medical service arrival (response interval) is 5– 8 min, or 8– 11 min to a first shock. • Immediate recognition of sudden cardiac arrest (SCA) by noting unresponsiveness or absent/gasping breathing • Immediate initiation of excellent CPR – "push hard, push fast" (but not too hard nor too fast) – with continuous attention to the quality of chest compressions, and to the frequency of ventilations • Minimizing interruptions in CPR

Important concepts • For health care professional rescuers, taking no more than 10 seconds to check for a pulse • For single untrained rescuers, encouraging performance of excellent chest compression-only CPR • Using automated external defibrillators as soon as available • Activating emergency medical services as soon as possible

The chain of survival • Early recognition and call for help Chest pain should be recognized as a symptom of myocardial ischemia. Cardiac arrest occurs in a quarter to a third of patients with myocardial ischemia within the first hour after onset of chest pain • Early bystander CPR The immediate initiation of CPR can double or quadruple survival from cardiac arrest • Early defibrillation Defibrillation within 3– 5 min of collapse can produce survival rates as high as 50– 70%. This can be achieved by public access and onsite AEDs. • Early advanced life support and standardized post-resuscitation care Advanced life support with airway management, drugs and correcting causal factors may be needed if initial attempts at resus-citation are un-successful.

Phases of resuscitation • Electrical phase — The electrical phase is defined as the first 4 to 5 minutes of arrest due to ventricular fibrillation (VF). Immediate DC cardioversion is needed to optimize survival of these patients. Performing excellent chest compressions while the defibrillator is readied also improves survival • Hemodynamic phase — The hemodynamic or circulatory phase, which follows the electrical phase, consists of the period from 4 to 10 minutes after SCA, during which the patient may remain in VF. Early defibrillation remains critical for survival in patients found in VF. Excellent chest compressions should be started immediately upon recognizing SCA and continued until just before defibrillation is performed. • Metabolic phase — Treatment of the metabolic phase, defined as greater than 10 minutes of pulselessness, is primarily based upon postresuscitative measures, including hypothermia therapy. If not quickly converted into a perfusing rhythm, patients in this phase generally do not survive.

Recognition of cardiac arrest • Recognizing cardiac arrest can be challenging. Both bystanders and emergency call handlers (emergency medical dispatchers)have to diagnose cardiac arrest promptly in order to activate the chain of survival. Checking the carotid pulse (or any other pulse)has proved to be an inaccurate method for confirming the presence or absence of circulation. • Agonal breaths are slow and deep breaths, frequently with a characteristic snoring sound. They originate from the brain stem, the part of the brain that remains functioning for some minute when deprived of oxygen. • The presence of agonal breathing can be erroneously interpreted as evidence that there is a circulation and CPR is not needed. Agonal breathing may be presenting up to 40% of victims in the first minutes after cardiac arrest, and if responded to as a sign of cardiac arrest, is associated with higher survival rates. • Bystanders should suspect cardiac arrest and start CPR if the victim is unresponsive and not breathing normally.

Recognition of cardiac arrest • Immediately following cardiac arrest, blood flow to the brain is reduced to virtually zero, which may cause seizure-like episodes that can be confused with epilepsy. • Bystanders should be suspicious of cardiac arrest in any patient presenting with seizures. • Although bystanders who have witnessed cardiac arrest events report changes in the victims’ skin color, notably pallor and bluish changes associated with cyanosis, these changes are not diagnostic of cardiac arrest.




Performance of excellent chest compressions • Chest compressions are the most important element of cardiopulmonary resuscitation (CPR). Coronary perfusion pressure and return of spontaneous circulation (ROSC) are maximized when excellent chest compressions are performed. • The following goals are essential for performing excellent chest compressions: • Maintain the rate of chest compression at 100 to 120 compressions per minute • Compress the chest at least 5 cm but no more than 6 cm with each down-stroke • Allow the chest to recoil completely after each down-stroke (it should be easy to pull a piece of paper from between the rescuer's hand the patient's chest just before the next down-stroke) • Minimize the frequency and duration of any interruptions

Performance of excellent chest compressions • To perform excellent chest compressions, the rescuer and patient must be in optimal position. The patient must lie on a firm surface. This may require a backboard if chest compressions are performed on a bed. All efforts to deliver excellent CPR must take precedence over any advanced procedures, such as tracheal intubation. • The rescuer places the heel of one hand in the center of the chest over the lower (caudad) portion of the sternum and the heel of their other hand atop the first. The rescuer's own chest should be directly above their hands. This enables the rescuer to use their body weight to compress the patient's chest, rather than just the muscles of their arms, which may fatigue quickly. • Animal and observational clinical studies suggest that chest compressions of proper depth (at least 5 cm) play an important role in successful resuscitation. In addition, full chest recoil between down-strokes promotes reduced intrathoracic pressures, resulting in enhanced cardiac preload and higher coronary perfusion pressures. • Inadequate compression and incomplete recoil are more common when rescuers fatigue, which can begin as soon as 1 minute after beginning CPR. The AHA Guidelines suggest that the rescuer performing chest compressions be changed every 2 minutes whenever more than one rescuer is present.

Minimizing interruptions • Interruptions in chest compressions during CPR, no matter how brief, result in unacceptable declines in coronary and cerebral perfusion pressure and worse patient outcomes. • Once compressions stop, up to 1 minute of continuous, excellent compressions may be required to achieve enough perfusion pressures. • Two minutes of continuous CPR should be performed following any interruption. • When preparing for defibrillation, rescuers should continue performing excellent chest compressions while charging the defibrillator until just before the single shock is delivered and resume immediately after shock delivery without taking time to assess pulse or breathing. • No more than three to five seconds should elapse between stopping chest compressions and shock delivery. If a single lay rescuer is providing CPR, excellent chest compressions should be performed continuously without ventilations.
 • When multiple trained personnel are present, the simultaneous performance of")
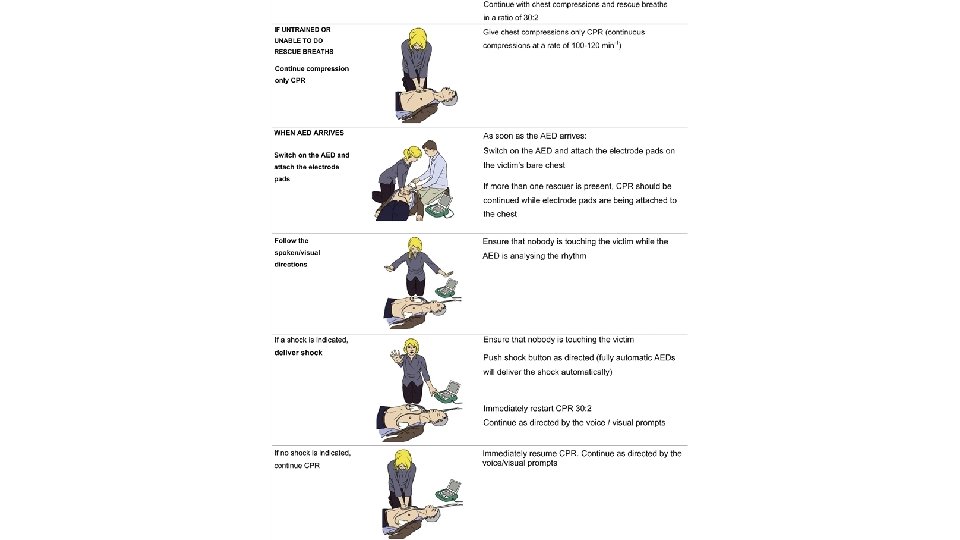
Compression-only CPR (CO-CPR) • When multiple trained personnel are present, the simultaneous performance of continuous excellent chest compressions and proper ventilation using a 30: 2 compression to ventilation ratio is recommended. • If a sole lay rescuer is present, should not interrupt excellent chest compressions to palpate for pulses or check for the return of spontaneous circulation, and should continue CPR until an AED is ready to defibrillate, EMS personnel assume care, or the patient wakes up • For many would-be rescuers, the requirement to perform mouth-tomouth ventilation is a significant barrier to the performance of CPR
 • This reluctance may stem from anxiety about performing CPR correctly")
Compression-only CPR (CO-CPR) • This reluctance may stem from anxiety about performing CPR correctly or fear of contracting a communicable disease, despite scant reports of infection contracted from the performance of mouth-to-mouth ventilation, none of which involve HIV. • CO-CPR circumvents these problems, potentially increasing the willingness of bystanders to perform CPR. • Evidence directly comparing bystander CO-CPR with conventional CPR using a 30: 2 ratio of compressions to ventilation is limited to one large observational study which suggests improved survival when conventional CPR is performed. • Nevertheless, we support CO-CPR when personnel to perform conventional CPR with a 30: 2 ratio are not available.

Ventilations • During the initial phase of SCA, when the pulmonary alveoli are likely to contain adequate levels of oxygen and the pulmonary vessels and heart likely contain sufficient oxygenated blood to meet markedly reduced demands, the importance of compressions supersedes ventilations. • Consequently, the initiation of excellent chest compressions is the first step to improving oxygen delivery to the tissues. This is the rationale behind the compressions-airway-breathing (C-A-B) approach to SCA. • Properly performed ventilations become increasingly important as pulselessness persists. In this, the metabolic phase of resuscitation, clinicians must continue to ensure that ventilations do not interfere with the cadence and continuity of chest compressions.

Ventilations • Give two ventilations after every 30 compressions for patients without an advanced airway • Give each ventilation over no more than one second • Provide only enough tidal volume to see the chest rise (approximately 500 to 600 m. L, or 6 to 7 m. L/kg) • Avoid excessive ventilation • Give one asynchronous ventilation every 8 to 10 seconds (6 to 8 per minute) to patients with an advanced airway (eg, supraglottic device, endotracheal tube) in place
 and")
Defibrillation • The effectiveness of early defibrillation in patients with ventricular fibrillation (VF) and short "downtimes" is well supported by the resuscitation literature and early defibrillation is a fundamental recommendation. • As soon as a defibrillator is available, providers should assess the cardiac rhythm and, when indicated, perform defibrillation as quickly as possible. For BLS, a single shock from an automated external defibrillator (AED) is followed immediately by the resumption of excellent chest compressions. • Biphasic defibrillators are preferred because of the lower energy levels needed for effective cardioversion. Biphasic defibrillators measure the impedance between the electrodes placed on the patient and adjust the energy delivered accordingly. Rates of first shock success are reported to be approximately 85 percent. • All defibrillations for patients in cardiac arrest be delivered at the highest available energy in adults (generally 360 J for a monophasic defibrillator and 200 J for a biphasic defibrillator). This approach reduces interruptions in CPR. • Controversy exists about the possible benefit of delaying defibrillation in order to perform excellent chest compressions for a predetermined period (eg, 60 to 120 seconds).

ADVANCED LIFE SUPPORT
 and early defibrillation for treatable arrhythmias remain the")
Principles • Excellent cardiopulmonary resuscitation (CPR) and early defibrillation for treatable arrhythmias remain the cornerstones of basic and ACLS • Early recognition of the deteriorating patient and prevention of cardiac arrest is the first link in the chain of survival. • Once cardiac arrest occurs, only about 20% of patients who have an in -hospital cardiac arrest will survive to go home. • Current ALS Guidelines strongly recommend that every effort be made NOT to interrupt CPR; other less vital interventions (eg, tracheal intubation or administration of medications to treat arrhythmias) are made either while CPR is performed

Do not attempt cardiopulmonary resuscitation • Does not wish to have CPR • Is very unlikely to survive cardiac arrest even if CPR is attempted.

Resuscitation team management • Leadership • Communication

In hospital resuscitation

Starting in-hospital CPR • One person starts CPR as others call the resuscitation team and collect the resuscitation equipment and a defibrillator. If only one member of staff is present, this will mean leaving the patient. • Give 30 chest compressions followed by 2 ventilations. • Compress to a depth of at least 5 cm but not more than 6 cm. • Perform chest compressions should be performed at a rate of 100– 120 min− 1. • Allow the chest to recoil completely after each compression; do not lean on the chest. • Minimize interruptions and ensure high-quality compressions. • Undertaking high-quality chest compressions for a prolonged time is tiring; with minimal interruption, try to change the persondoing chest compressions every 2 min. • Maintain the airway and ventilate the lungs with the most appropriate equipment immediately to hand. Pocket mask ventilation or two-rescuer bag-mask ventilation, which can be supplemented with an oral airway, should be started. Alternatively, use a supraglottic airway device (SGA) and self-inflating bag. Tracheal intubation should be attempted only by those who are trained, competent and experienced in this skill.

Starting in-hospital CPR • Waveform capnography must be used for confirming tracheal tube placement and monitoring ventilation rate. Waveform capnography can also be used with a bag-mask device and SGA. • Use an inspiratory time of 1 s and give enough volume to produce a normal chest rise. Add supplemental oxygen to give the highest feasible inspired oxygen as soon as possible. • Once the patient’s trachea has been intubated or a SGA has been inserted, continue uninterrupted chest compressions (except for defibrillation or pulse checks when indicated) at a rate of 100– 120 min and ventilate the lungs at approximately 10 breaths min. Avoid hyperventilation (both excessive rate and tidal volume). • If there is no airway and ventilation equipment available, con-sider giving mouth-to-mouth ventilation. • When the defibrillator arrives, apply self-adhesive defibrillation pads to the patient whilst chest compressions continue and then briefly analyze the rhythm. • Continue resuscitation until the resuscitation team arrives or the patient shows signs of life.

Advanced Life Support

Advanced Life Support

Advanced Life Support • The first monitored rhythm is VF/p. VT in approximately 20% bothfor inhospital and out-of-hospital cardiac arrests. • Minimize the delay between stopping chest compressions and delivery of the shock (the pre shock pause); even a 5– 10 s delay will reduce the chances of the shock being successful. • If IV/IO access has been obtained, during the next 2 min of CPR give adrenaline 1 mg and amiodarone 300 mg. • The use of waveform capnography may enable ROSC to be detected without pausing chest compressions and may be used as a way of avoiding a bolus injection of adrenaline after ROSC has been achieved. Several human studies have shown that there is a significant increase in end-tidal CO 2 when ROSC occurs.

Advanced Life Support • In animal studies, peak plasma concentrations of adrenaline occur at about 90 s after a peripheral injection and the maximum effect on coronary perfusion pressure is achieved around the same time (70 s). • When VF is present for more than a few minutes, the myocardium is depleted of oxygen and metabolic substrates. • A single precordial thump has a very low success rate for cardioversion of a shockable rhythm.

Advanced Life Support • Tracheal intubation provides the most reliable airway, but should be attempted only if the healthcare provider is properly trained and has regular, ongoing experience with the technique. • Tracheal intubation must not delay defibrillation attempts. Personnel skilled in advanced airway management should attempt laryngoscopy and intubation without stopping chest compressions; a brief pause in chest com-pressions may be required as the tube is passed through the vocal cords, but this pause should be less than 5 s. • In the absence of personnel skilled in tracheal intubation, a supraglottic airway (SGA) (e. g. laryngeal mask airway, laryngeal tube or i-gel) is an acceptable alternative.

Intravenous access and drugs • Establish intravenous access if this has not already been achieved. Although peak drug concentrations are higher and circulation times are shorter when drugs are injected into a central venous catheter compared with a peripheral cannula • A central venous catheter requires interruption of CPR and can be technically challenging and associated with complications. • Peripheral venous cannulation is quicker, easier to perform and safer. • Drugs injected peripherally must be followed by a flush of at least 20 ml of fluid and elevation of the extremity for 10– 20 s to facilitate drug delivery to the central circulation. • If intravenous access is difficult or impossible, consider the Intra Osseus route. Injection of drugs achieves adequate plasma concentrations in a time comparable with injection through a vein. • Multiple studies have demonstrated that lidocaine, epinephrine, atropine, vasopressin, and naloxone are absorbed via the trachea; however, the serum drug concentrations achieved using this route are unpredictable.

Adrenaline • During cardiac arrest, the initial IV/IO dose of adrenaline is 1 mg. There are no studies showing improvement in survival or neurological outcomes with higher doses of adrenaline for patients in refractory cardiac arrest. • There is an increasing concern about the potential detrimental effects of adrenaline. While its alpha-adrenergic, vasoconstrictive effects cause systemic vasoconstriction, which increases macrovascular coronary and cerebral perfusion pressures, its beta-adrenergic actions (inotropic, chronotropic) may increase coronary and cerebral blood flow, but with concomitant increases in myocardial oxygen consumption, ectopic ventricular arrhythmias (particularly when the myocardium is acidotic), transient hypoxemia from pulmonary arteriovenous shunting, impaired microcirculation, and worse post-cardiac arrest myocardial dysfunction. • The optimal dose of adrenaline is not known, and there are no human data supporting the use of repeated doses.

Amiodarone • Amiodarone is a membrane-stabilising anti-arrhythmic drug that increases the duration of the action potential and refractory period in atrial and ventricular myocardium • Following three initial shocks, amiodarone in shock-refractory VF improves the short-term outcome of survival to hospital admission compared with placebo or lidocaine. • Appears to improve the response to defibrillation when given to humans or animals with VF or hemodynamically unstable ventricular tachycardia. • Amiodarone 300 mg is recommended if VF/p. VT persists after three shocks.

Lidocaine • Is recommended for use during ALS when amiodarone is unavailable. Lidocaine is a membrane-stabilizing anti-arrhythmic drug that acts by increasing the myocyte refractory period. It decreases ventricular automaticity, and its local anaesthetic action suppresses ventricular ectopic activity. • Lidocaine is indicated in refractory VF/p. VT (when amiodarone is unavailable).

Intravenous fluids • Hypovolemia is a potentially reversible cause of cardiac arrest. • Infuse fluids rapidly if hypovolemia is suspected. In the initial stages of resuscitation there are no clear advantages to using colloid, so use balanced crystalloid solutions, Hartmann’s solution or 0. 9% sodium chloride. • Avoid glucose, which is redistributed away from the intravascular space rapidly and causes hyperglycaemia, and may worsen neurological outcome after cardiacarrest.

Duration of resuscitation attempt • Duration of resuscitative effort >30 minutes without a sustained perfusing rhythm • Initial electrocardiographic rhythm of asystole • Prolonged interval between estimated time of arrest and initiation of resuscitation • Patient age and severity of comorbid disease • Absent brainstem reflexes • Normothermia
- Slides: 43