BASIC INFECTION PREVENTION IN LONG TERM CARE FACILITIES

BASIC INFECTION PREVENTION IN LONG TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director SPICE

DEMOGRAPHIC REALITY Ø The United States continues to experience incredible transformation. Ø Over 10, 000 baby boomers are turning 65 every day, and the fastest growing Ø Ø demographic in the U. S. is women over age 85. This age wave is expected to continue well into the next century. The population age 65 and over has increased from 35. 9 million in 2003 to 44. 7 million in 2013 (a 24. 7 percent increase) and is projected to more than double to 98 million in 2060. By 2040, there will be about 82. 3 million older persons, over twice their number in 2000. People 65 and older represented 14. 1 percent of the population in the year 2013 but are expected to grow to be 21. 7 percent of the population by 2040. The 85+ population is projected to triple from 6 million in 2013 to 14. 6 million in 2040. The 2015 White House Conference on Aging: Looking to the future

OBJECTIVES Describe the problem of healthcare associated infections in LTCFs 2. Discuss basic measures for controlling transmission of infections in LTCF. 3. Discuss basics of dressing changes 4. Provide time for interactive competency demonstrations and discussion 1.

Are HAIs A Problem In Long Term Care? ?

YES Ø An estimated 1. 5 MILLION infections occur annually in LTCF Ø Resulting in as many as 350, 000 to 400, 00 deaths. Ø Cost between $673 million to $2 billion UTIs Sk Tis in/S su of e t Respiratory illness C diff Norovirus

BURDEN OF HAI IN LTC Ø A significant source of morbidity and mortality for nursing home residents and account for up to half of all nursing home resident transfers to hospitals Ø Result in an estimated 150, 000 to 200, 000 hospital admissions per year at an estimated cost of $673 million to $2 billion annually. Ø When a nursing home resident is hospitalized with a primary diagnosis of infection, the death rate can reach as high as 40 percent. “Interpretive Guidelines for Long-Term Care Facilities, ” Tag F 441”

WHY #1 Ø LCTFs are different from other healthcare settings in that elderly patients at increased risk for infection, are brought together in one setting and remain in the facility for extended periods of time; for most residents, it is their home.

WHY #2 Ø An atmosphere of community is fostered and residents share common eating and living areas, and participate in various facility-sponsored activities Ø Since able residents interact freely with each other, controlling transmission of infection in this setting is challenging

WHY # 3 Ø Residents who are colonized or infected with certain microorganisms are, in some cases, restricted to their room. Ø However, because of the psychosocial risks associated with such restriction, it has been recommended that psychosocial needs be balanced with infection control needs in the LTCF setting
 Ø “Published data on overall high employee")
ADDITIONAL CONTRIBUTING FACTORS Ø Nurse (staff turnover) Ø “Published data on overall high employee turnover rates in LTC facilities; 2011 data from the Quality Long Term Care Commission showed the following turnover rates: Ø administrators, 3 percent; Ø director of nursing, 39 percent; Ø RNs, 50 percent; Ø LPNs, 49 percent; and Ø CNAs, 71 percent. ” Infection Prevention in LTC: Emphasis Needed on Education, Evidence-Based Practices; Infection Control Today: Gail Bennett, RN, MSN, CIC, Rome, GA ICP Associates, Inc.

WHAT CAN WE DO BASIC INTERVENTIONS STANDARD PRECAUTIONS TRANS M BASED ISSION PRECA UTION S

MEASURES TO CONTROL TRANSMISSION STANDARD PRECAUTIONS Ø Implementation of Standard Precautions constitutes the primary strategy for the prevention of healthcareassociated transmission of infectious agents among patients and healthcare personnel. Ø Hand Hygiene Ø Soap and water vs alcohol based hand rub (ABHR) Ø Personal Protective Equipment Ø Gloves, gown, mask, eye protection TRANSMISSION BASED PRECAUTIONS Ø For patients who are known or suspected to be infected or colonized with infectious agents, including certain epidemiologically important pathogens, which require additional control measures to effectively prevent transmission. Ø Contact Ø Enteric or enhanced contact Ø Droplet Ø Airborne
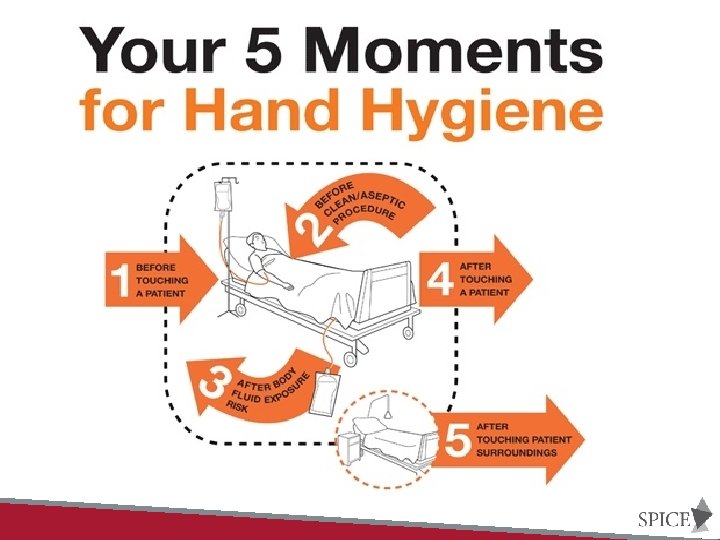

HAND HYGIENE Soap + Water OR Alcohol based hand rub

SOAP AND WATER Ø When hands are visibly dirty or contaminated with proteinaceous material or are visibly soiled with blood or other body fluids, wash hands with either a nonantimicrobial soap and water or an antimicrobial soap and water

SOAP AND WATER Ø Wash hands with non-antimicrobial soap and water or with antimicrobial soap and water if contact with spores (e. g. , C. difficile or Bacillus anthracis) is likely to have occurred. Ø The physical action of washing and rinsing hands under such circumstances is recommended because alcohols, chlorhexidine, iodophors, and other antiseptic agents have poor activity against spores.

HOW TO WASH HANDS Ø Wet hands with water Ø Apply amount of product recommended by manufacturer Ø Rub hands together vigorously at least 15 seconds, covering ALL surfaces of the hands and fingers Ø Rinse hands Ø Dry with disposable towel Ø Use towel to turn off faucet (and open door)

ALCOHOL BASED HAND RUB Ø If hands are not visibly soiled, use an alcohol-based hand rub for routinely decontaminating hands in all other clinical situations (listed next). Alternatively, wash hands with an antimicrobial soap and water in all clinical situations described. ü Before direct contact with patient ü Before donning sterile gloves ü Before inserting ANY invasive device (indwelling urinary catheters for example) ü After contact with intact skin ü After contact with body fluids, excretions, mucous membranes etc. , if not visible soiled ü If moving from contaminated body site – to clean body site ü After contact with inanimate objects (environment, medical equipment) ü After removing gloves

HOW TO USE AN ALCOHOL BASED HAND RUB Ø Apply product to palm of one hand rub hands together, covering all surfaces of hands and fingers, until hands are dry Ø Follow the manufacturer’s recommendations regarding the volume of product to use.

OTHER ASPECTS OF HAND HYGIENE ü Do not wear artificial fingernails or extenders when having direct contact with patients at high risk ü Keep natural nails tips less than 1/4 -inch long ü Wear gloves when contact with blood or other potentially infectious materials, mucous membranes, and nonintact skin could occur ü Remove gloves after caring for a patient. Do not wear the same pair of gloves for the care of more than one patient, and do not wash gloves between uses with different patients ü Change gloves during patient care if moving from a contaminated body site to a clean body site

HAND HYGIENE
 Ø Three overriding principals related to personal protective")
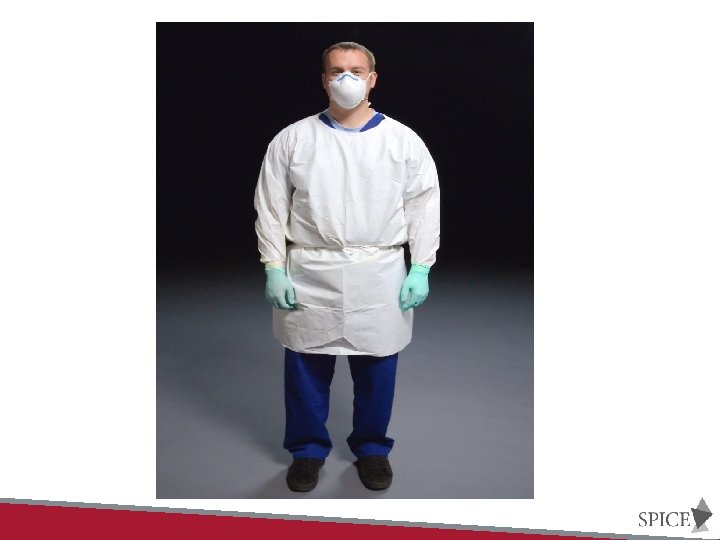
USE OF PERSONAL PROTECTIVE EQUIPMENT (PPE) Ø Three overriding principals related to personal protective equipment (PPE) Ø Wear PPE when the nature of the anticipated patient interaction indicates that contact with blood or body fluids may occur Ø Prevent contamination of clothing and skin during the process of removing PPE Ø Before leaving the patient’s room or cubicle, remove and discard PPE
 ü Keep hands away from face ü Work from")
SAFE WORK PRACTICES (PPE USE) ü Keep hands away from face ü Work from clean to dirty ü Limit surfaces touched ü Change when torn or heavily contaminated ü Perform hand hygiene

GLOVES Ø Wear gloves when it can be reasonably anticipated that contact with blood or other potentially infectious materials, mucous membranes, nonintact skin, or potentially contaminated intact skin (e. g. , of a patient incontinent of stool or urine) could occur Ø Remove gloves after contact with a patient and/or the surrounding environment (including medical equipment) Ø Do not wear the same pair of gloves for the care of more than one patient. Ø Do not wash gloves for the purpose of reuse since this practice has been associated with transmission of pathogens Ø Change gloves during patient care if the hands will move from a contaminated body-site (e. g. , perineal area) to a clean body-site

GOWNS Ø Wear a gown, that is appropriate to the task, to protect skin and prevent soiling or contamination of clothing during procedures and patient-care activities when contact with blood, body fluids, secretions, or excretions is anticipated Ø Wear a gown for direct patient contact if the patient has uncontained secretions or excretions Ø Remove gown and perform hand hygiene before leaving the patient’s environment Ø Do not reuse gowns, even for repeated contacts with the same patient

MOUTH, NOSE, EYE PROTECTION Ø Use PPE to protect the mucous membranes of the eyes, nose and mouth during procedures and patient-care activities that are likely to generate splashes or sprays of blood, body fluids, secretions and excretions. Ø Select masks, goggles, face shields, and combinations of each according to the need anticipated by the task performed

Donning PPE

• Gloves Doffing PPE – Grasp outside of glove with opposite gloved hand, peel off – Hold removed glove in gloved hand – Slide fingers of ungloved hand under remaining glove at wrist • Goggles/Face Shield – To remove, handle by “clean” head band or ear pieces – Place in designated receptacle • Gown – – Unfasten neck, then waist ties Remove gown using a peeling motion Gown will turn inside out Hold away from body, roll into a bundle and discard • Mask – Grasp ONLY bottom then top ties/elastics and remove – Discard

PERSONAL PROTECTIVE EQUIPMENT

Wound Care Issues Ø Present literature suggests that pressure ulcer dressing protocols may use clean technique rather than sterile, but that appropriate sterile technique may be needed for those wounds that recently have been surgically debrided or repaired. • ©National Pressure Ulcer Advisory Panel March 2014

Ø Sterile technique. Ø Sterile is generally defined as meaning free from microorganisms. Ø Involves strategies used in patient care to reduce exposure to microorganisms and maintain objects and areas as free from microorganisms as possible. Ø Sterile technique involves meticulous hand washing, use of a sterile field, use of sterile gloves for application of a sterile dressing, and use of sterile instruments. Ø “Sterile to sterile” rules involve the use of only sterile instruments and materials in dressing change procedures; and avoiding contact between sterile instruments or materials and any non-sterile surface or products. Ø Sterile technique is considered most appropriate in acute care hospital settings, for patients at high risk for infection, and for certain procedures such as sharp instrumental wound debridement.

Ø Clean Technique Ø Clean means free of dirt, marks, or stains. Ø Clean technique involves strategies used in patient care to reduce the overall number of microorganisms or to prevent or reduce the risk of transmission of microorganisms from one person to another or from one place to another. Ø Clean technique involves meticulous handwashing, maintaining a clean environment by preparing a clean field, using clean gloves and sterile instruments, and preventing direct contamination of materials and supplies. Ø No “sterile to sterile” rules apply. Ø This technique may also be referred to as non-sterile. Ø Clean technique is considered most appropriate for long-term care, home care, and some clinic settings; for patients who are not at high risk for infection; and for patients receiving routine dressings for chronic wounds such as venous ulcers, or wounds healing by secondary intention with granulation tissue.

General Steps; Changing Dressings ü Disinfect area around bedside where supplies are going to be placed (over bed table etc. , ) ü Place trash bag near by ü Perform hand hygiene ü Gather all necessary supplies, equipment ü Don clean disposable gloves ü Remove tape and outer dressings and dispose of in trash container ü Assess the wound for color, edema, exudate, odor etc. , ü Remove soiled gloves, dispose of and perform hand hygiene ü Put on clean gloves ü Apply dressing and secure ü Dispose of all supplies ü Remove gloves and perform hand hygiene

Points to Remember • Contamination of the wound is minimized by not touching it. Blotting excess fluid that pools in the wound and cleaning the periwound skin with moist gauze is acceptable. • Contamination of the wound from supplies is avoided by opening and preparing all that is needed before removing the dressing and putting on fresh clean gloves. • Contamination of the local environment and supplies is avoided by organizing the procedure to ensure that anything coming into contact with the wound does not contact jars, bottles, tubes, bedside table or supplies to be kept for use at a later date.

DRESSING CHANGES

I prefer being this walking metamorphosis Than having that old opinion about everything

INTERACTIVE SESSIONS
- Slides: 38