Basic Human Needs Comfort and Pain Management Pain

Basic Human Needs Comfort and Pain Management

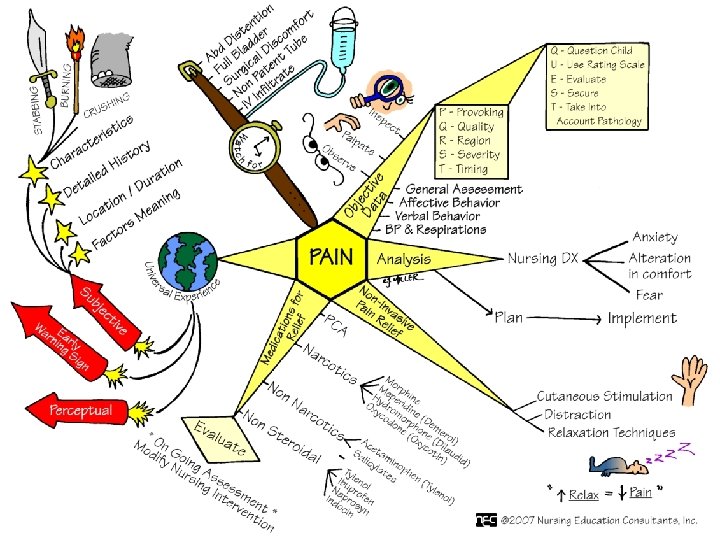
Pain • Unpleasant, subjective sensory and emotional experience associated with an actual or potential tissue damage • Can be a factor inhibiting the ability and willingness to recover from illness • Subjective experience

Comfort • Concept central to the art of nursing • Through comfort measures nurses provide strength, hope, solace, support, encouragement, and assistance • As subjective as pain

Pain • Mc. Caffery on Pain-Pain is whatever the experiencing person says it is, existing whenever the person says it does. (Margo Mc. Caffery, 1979) • Pain relief is a basic legal right (American Bar Association, 2000) • Nurses are ethically and legally responsible for managing pain and relieving suffering.

Pain Management • Effective pain management reduces physical discomfort • Promotes earlier mobilization and return to work • Shortens hospital stay and reduces health care costs

Pain Management

Nature of Pain • Subjective, highly individualized • Stimulus can be physical and/or mental in nature • Pain is tiring, places demands on person’s energy • Can interfere with relationships and influence the meaning of life

Nature of Pain • Cannot be objectively measured • Certain types of pain produce predictable symptoms • Pain Assessment-nurse relies on clients words and behaviors • Protective physiologic mechanism, changes behavior

Physiology of Pain Categories • • • Acute Chronic Idiopathic Pain Cancer pain Pain by Inferred Pathology/Nociceptive & Neuropathic • Pain as a result of a Metabolic Need/Ischemic Pain

Nociceptive Pain • Normal processing of stimuli that damages normal tissue or has the potential to do so if prolonged • Usually responsive to nonopioids or opioids • Somatic or visceral

Somatic Pain • Arises from bone, joint, muscle, skin or connective tissue • Usually aching, throbbing, well-localized pain • Responds to traditional analgesia

Visceral Pain • Arises from visceral organs such as the GI tract, heart, and pancreas. Can be subdivided further: 1. Tumor involvement of organ 2. Obstruction of hollow viscus

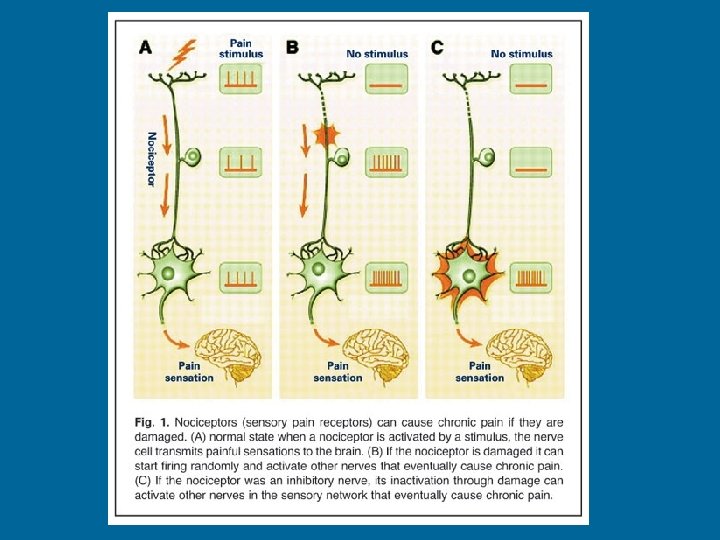
Neuropathic Pain • Abnormal processing of sensory input by the peripheral or CNS • Treatment usually with tricyclic antidepressants, SSRI’s, anticonvulsants • Centrally generated pain • Peripherally generated pain

Idiopathic Pain • Chronic pain in the absence of an identifiable cause • Complex Regional Pain Syndrome • Fibromyalgia

Ischemic Pain • Pain as a result of the metabolic need for oxygen • Warning sign of tissue damage • Cardiac pain (angina, MI) • Vascular pain- Peripheral vascular disease, intermittent claudication

Nociceptive Pain • Transduction • Transmission • Perception • Modulation

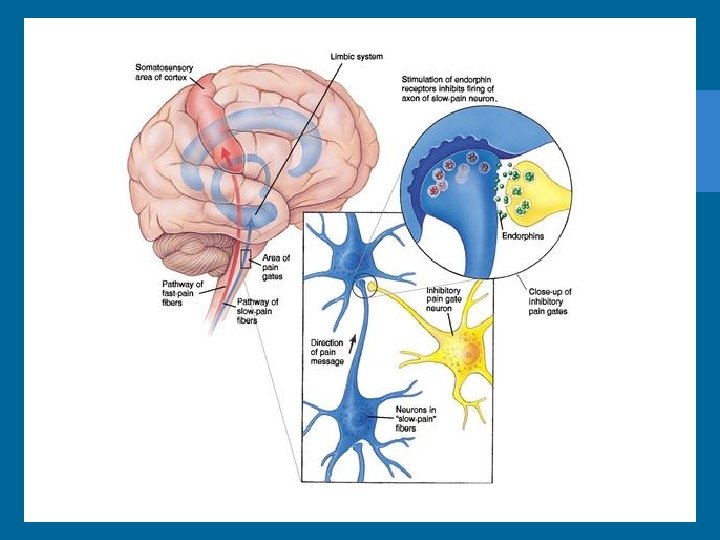
Gate Control Theory of Pain • Pain impulses can be regulated or even blocked by gating mechanism along CNS • Theory suggests that pain impulses pass when gate is open and blocked when gate is closed • Closing the gate is basis for pain relief interventions
, which")
Gate Control Theory of Pain • Involves the addition of mechanoreceptors (Abeta neurons), which releases inhibiting neurotransmitter (Serotonin) • If dominant input is from A-beta fibers, gating mechanism will close, pain reduced, due to release of Serotonin (Back rub) • If dominant input from A-delta fiber, gate will be open and pain perceived • Release of endorphins also close gate

Physiological Response to Pain • ANS stimulated as pain impulses ascend the spinal cord • Pain of low to moderate intensity and superficial pain elicit the “fight or flight” reaction • Sympathetic stimulation results in physiologic responses (Increased heart rate, peripheral vasoconstriction, dilatation of bronchial tubes, increased blood sugar)
 involving organs")
Physiological Response to Pain • Continuous pain or severe, deep pain (visceral) involving organs puts the parasympathetic system into effect • Parasympathetic stimulation results in pallor, muscle tension, decreased heart rate and BP, N/V, weakness, exhaustion

Behavioral Responses to Pain • Pain threatens physical & psychological wellbeing • Some people choose not to express pain (belief, value, cultural influences) • Typical body movements that indicate pain: clenching teeth, grimace, holding area, bent posture

Acute Pain • Follows acute injury, disease, surgical intervention • Rapid onset • Varies in intensity (mild-severe) • Lasts a brief period of time (less than 6 months)

Chronic Pain • • Prolonged Varies in intensity Lasts longer than 6 months Also known as chronic non-malignant pain • Arthritis, headache, myofascial pain, low back pain

Cancer Pain • Pain that is due to tumor progression • Related to pathology, invasive procedures, infection, toxicities of Rx • Can be acute or chronic, nociceptive or neuropathic • At the actual site or distant to the site (Referred pain)

Factors Influencing Pain • • • Age Gender Culture Meaning of pain Attention Anxiety Fatigue Previous Experience Coping Style Family & Social Support

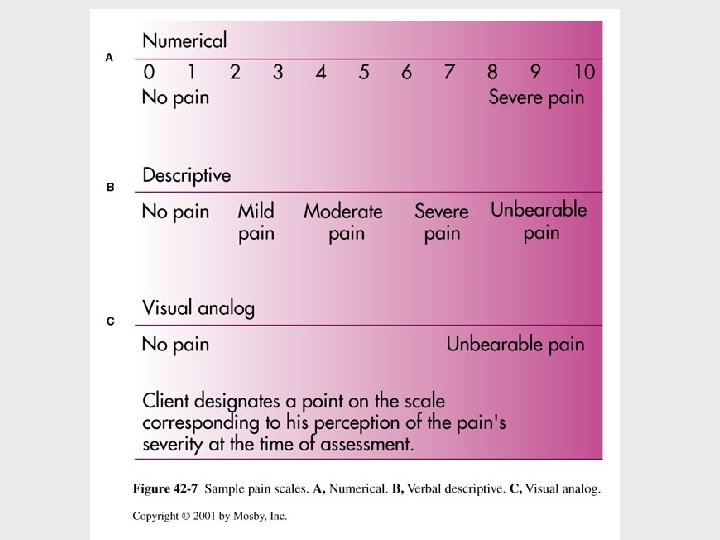
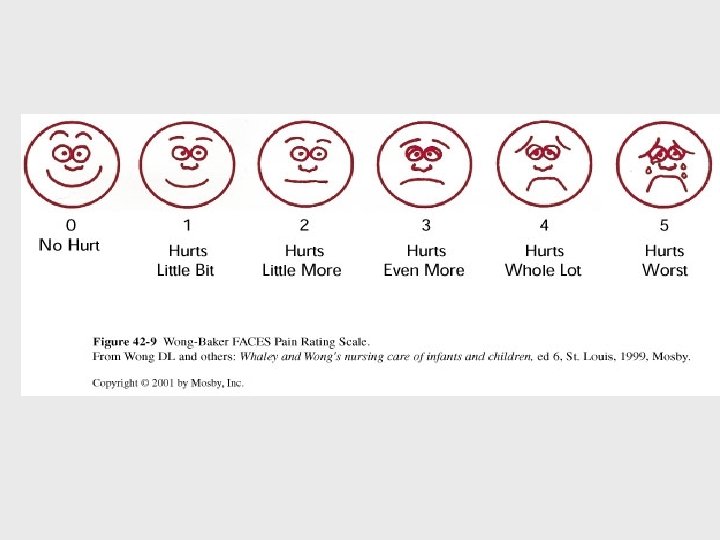
Nursing Process Assessment • • • AHRQ clinical practice guidelines Clients expression of pain Characteristics of pain Onset & duration Location Intensity (Pain scales-numerical, FACES)

Assessment • • Quality Pain pattern Concomitant Symptoms Effect of pain on client (physical, behavioral, effect on ADL) • Cultural Considerations
 Self-care Deficit")
Nursing Process Nursing Diagnosis • • • Anxiety Pain (Acute or Chronic) Self-care Deficit Sleep Pattern Dysfunction Sexual Dysfunction

Nursing Process Implementation • Non-Pharmacological and pharmacological Methods • Non-pharmacologic methods-lessen pain, can be used at home or in hospital • Utilize cognitive-behavioral & physical approaches • Allow patients some control

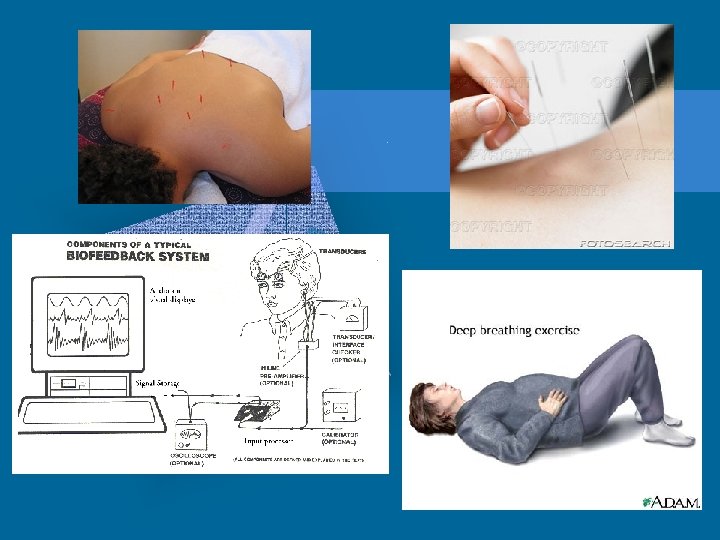
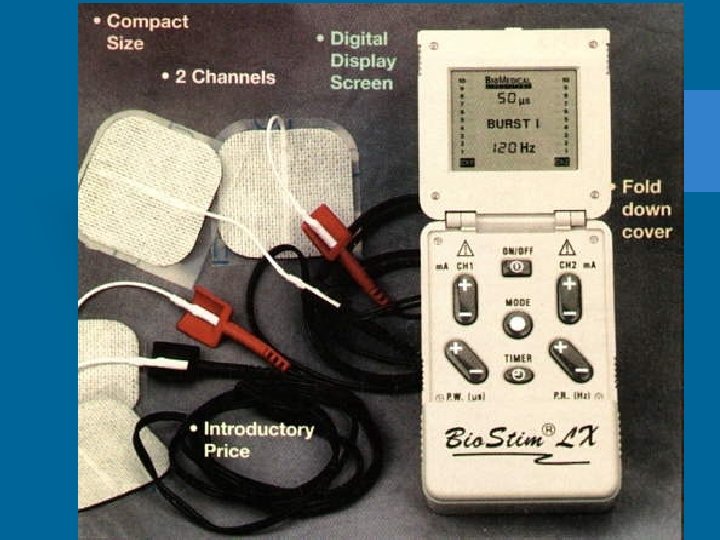
Non-pharmacological Methods • • Acupuncture Relaxation Guided Imagery Distraction Music Biofeedback Self-Hypnosis Reducing Pain Perception Cutaneous Stimulation (Heat or Cold application, massage, TENS unit)



Pharmacologic Methods • • Require a physicians order Guidelines set by regulatory agencies Analgesics most common method Tendency to under treat with pain meds
 • Narcotics, Opioids")
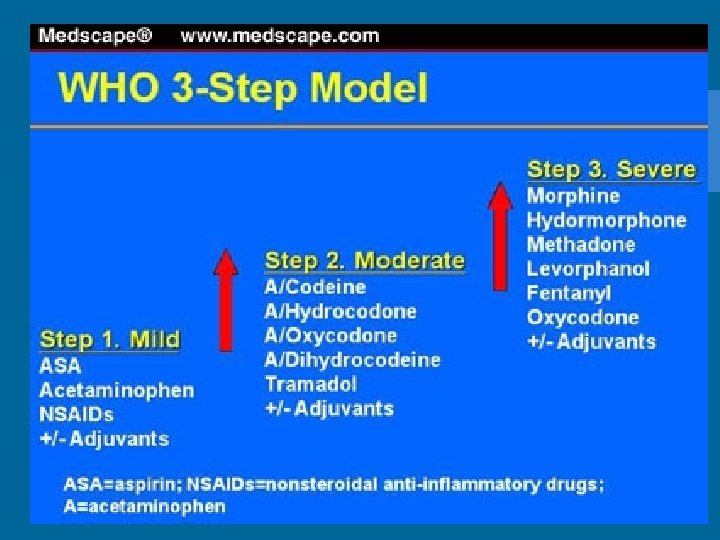
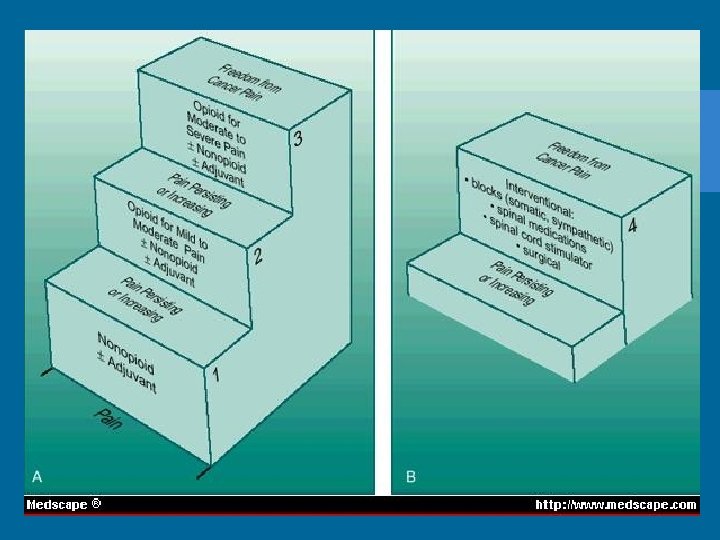
Analgesics • Non-opioid or non-narcotic agents & non-steroidal anti-inflammatory agents (NSAIDS) • Narcotics, Opioids • Adjuvants, Co-analgesics

NSAIDS • Relief of mild to moderate pain • Believed to inhibit prostaglandins & inhibits cellular response during inflammation • Acts on peripheral nerve receptors to reduce the transmission & reception of pain • Does not cause sedation or respiratory depression or interfere with bowel/bladder function • Avoid prolonged or overuse in elderly

NSAIDS • Used in arthritic pain, minor surgical, dental procedures, low back pain, should be initially used in mild-moderate post-op pain • Motrin, Naprosyn, Indocin, Toradol

Opioids • Moderate to severe pain • Act on CNS, act on higher brain centers & spinal cord binding with opiate receptors to modify perception of or reaction to pain • Risk for depression of vital nervous system functions

Opioids • If pain is anticipated for longer than 12 -24 hours, ATC timing should be used instead of PRN timing • Opioids can be used effectively with elderly, START LOW & GO SLOW • Morphine, Demerol, Codeine, Percocet, Fentanyl, Hydromorphone • Opioid antagonist- NARCAN-reverses effect

Adjuvant Therapy • Sedatives, anti-anxiety, & muscle relaxants • Enhance pain control or relieve symptoms associated with pain • Vistaril, Elavil, Thorazine, Valium, Ativan, Xanax

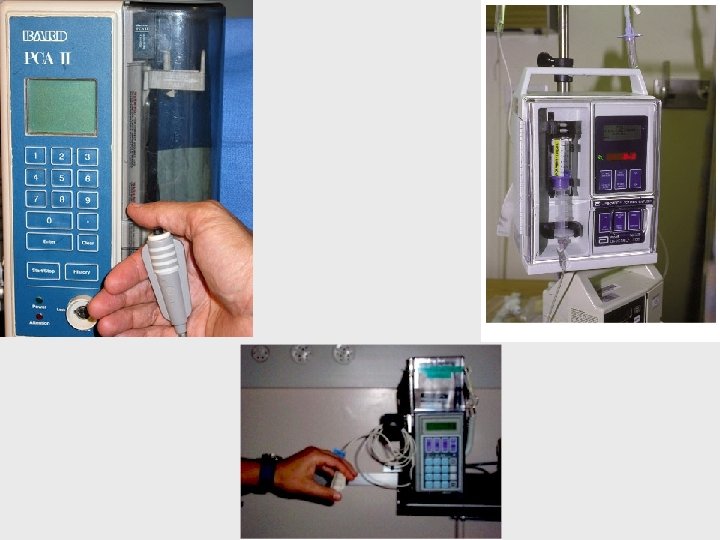
Patient-Controlled Analgesia PCA • Drug delivery system • Patients have control over pain therapy • Safe method for post-op, traumatic, or cancer pain • Self-administration without risk of overdose • IV administration
 On demand dose Hourly maximum")
PCA Prescription • • Loading Dose Basal (Continuous rate) On demand dose Hourly maximum amounts can be prescribed

Local & Regional Anesthetics • • Wound suturing Delivery of baby Performing simple surgery Epidural Analgesia for post-op pain management, L&D pain, chronic cancer pain • On-Q Pain Pump
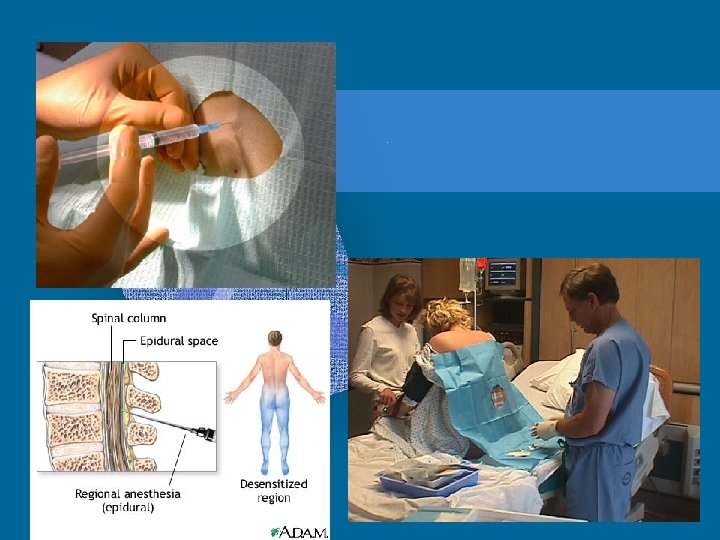


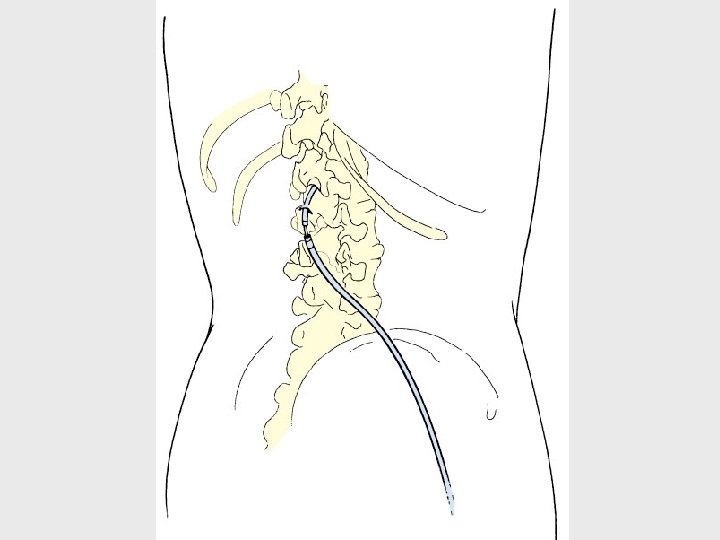
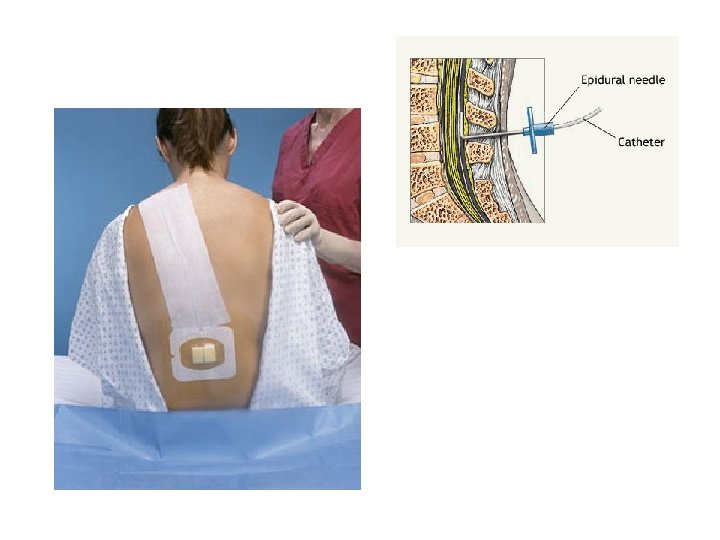
Epidural Pain Management • Short or long term • Administered into spinal epidural space • Catheter is left in place, secured with tape and dressing • Can be continuous infusion or daily injection
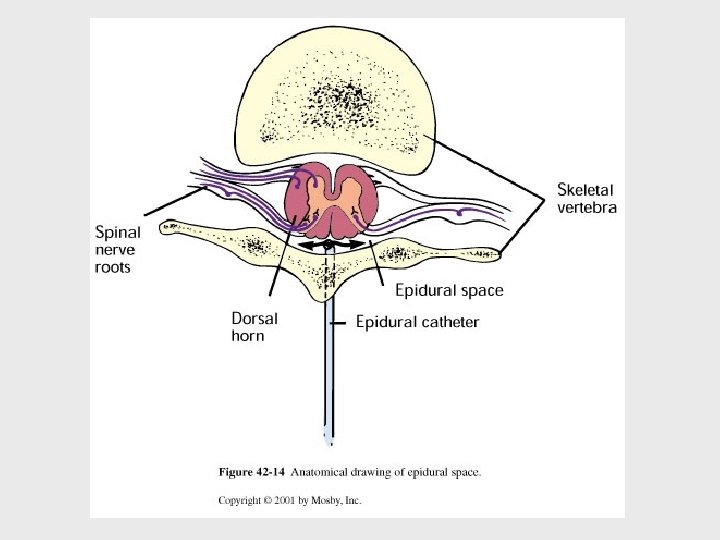

Epidural Pain Management • Monitor hourly for: 1. Catheter Displacement 2. Catheter Function 3. Respiratory Depression 4. Side effects: N/V, itching, urinary retention, constipation 5. Pain effect

Cancer Pain Management • Long acting preparations, sustained release • Drug dependence low in cancer related pain • Can develop tolerance, requiring higher doses • Goal is to minimize pain, rather than cure it

Procedure Pain Management • • • Turning Tracheal Suctioning Placement of central line, chest tubes Dressing changes Getting patient OOB Prior to Physical Therapy

Clicker Question • 1. When a smiling and cooperative client complains of discomfort, nurses caring for this client often harbor misconceptions about the client’s pain. To properly care for clients in pain, nurses need to remember that: • A. Chronic pain is psychological in nature. • B. Clients are the best judges of their pain. • C. Regular use of narcotic analgesics leads to drug addiction. • D. The amount of pain is reflective of actual tissue damage. 43 - 62

Clicker Question • 2. Established pain management guidelines direct nurses to frequently assess the client’s pain. The most appropriate action for the nurse to take when assessing the client’s reaction to pain is to: • A. Ask what precipitates pain. • B. Question the client about the location of pain. • C. Offer the client a pain scale to objectively identify the pain. • D. Use open-ended questions to find out about the client’s pain. 43 - 63

Clicker Question • 3. A client has just undergone abdominal surgery. When discussing with the client several pain relief interventions, the most appropriate recommendation would be: • A. Adjunctive therapy • B. Nonopioids • C. NSAIDs • D. PCA pain management 43 - 64
- Slides: 64