Basic HIV Course for Health Professionals Session 7

Basic HIV Course for Health Professionals Session 7 b: Prevention and Management of Opportunistic Infections

Learning Objectives By the end of this session participants should be able to: • Describe common opportunistic infections • Discuss the prevention of opportunistic infections • Explain the management of common opportunistic infections
 • Cryptococcal meningitis")
What are The Most Common Opportunistic Infections? • Pneumocystis pneumonia (PCP) • Cryptococcal meningitis • Tuberculosis (TB)
 • Pneumocystis jiroveci pneumonia (PCP) is WHO stage 4 and requires")
Pneumocystis Pneumonia (PCP) • Pneumocystis jiroveci pneumonia (PCP) is WHO stage 4 and requires ART fast tracking • Commonly occurs when a person has a CD 4 count below 200 • Mainly a clinical diagnosis • Signs and symptoms include fever, cough, tachypnoea, and dyspnoea.

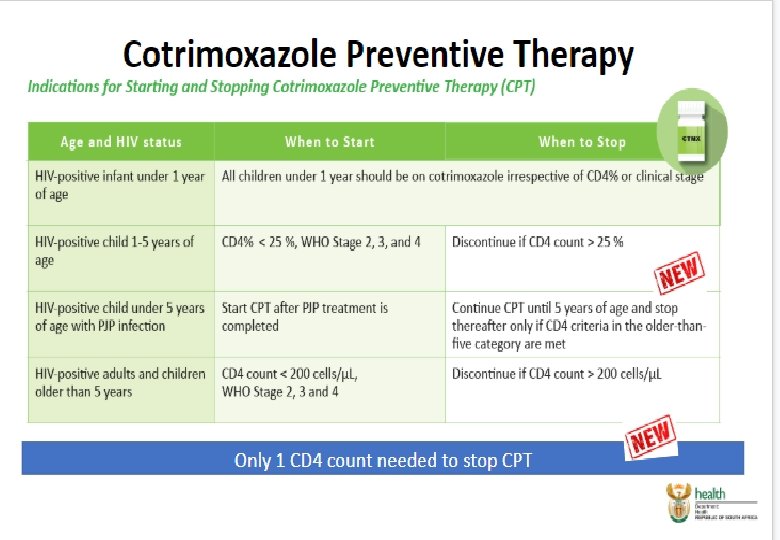
Recommended Prophylaxis for PCP • Co-trimoxazole prophylaxis markedly reduces hospitalization and mortality and provides protection against: • • Pneumocystis pneumonia (PCP) Toxoplasmosis malaria and many other bacterial infections

Recommended Treatment for PCP Adults: Co-trimoxazole, oral, 6 hourly for 3 weeks Recommended treatment for PCP in Adults Approx. weight kg Use one of the following tablets <40 kg >40– 56 kg >56 kg 80/400 mg 2 tablets 3 tablets 4 tablets 160/800 mg 1 tablet 1½ tablets 2 tablets

Referral • • All children Breathing rate > 24 breaths/minute Shortness of breath with mild effort Cyanosed patients

Secondary Co-trimoxazole Prophylaxis Use one of the following tablets 80/400 mg 2 tablets 160/800 mg 1 tablet
 • Safe to use in pregnancy • CPT should")
More on Co-trimoxazole Prophylaxis (1) • Safe to use in pregnancy • CPT should be taken until CD 4 rises above 200 • Prescribe 160/800 orally once daily • Monitor patient clinically every 3 months • Do not delay ART in favour of CPT initiation • Most common side effect is rash • Rare side effect: neutropenia
 • Use dapsone 100 mg a day for patients")
More on Co-trimoxazole Prophylaxis (2) • Use dapsone 100 mg a day for patients who have had a mild reaction to co-trimoxazole • Stop CPT only once well on ART and CD 4 >350 on more than two occasions • Recommence co-trimoxazole when CD 4 drops below 350 cells/µl or if ART fails or a new opportunistic infection develops
 Screening and Treatment • Found in soil from bird droppings that are")
Cryptococcus (Crypto) Screening and Treatment • Found in soil from bird droppings that are breathed in as dust • Cannot be passed in air from one infected person to another • Infection can be dormant for many years • Cryptococcus is only a problem if a person’s CD 4 count drops below 100 • Smokers and people who work outdoors have a higher risk of cryptococcus
 • Screen HIV-positive adults with CD 4")
Screening for Cryptococcal Disease in Adults (1) • Screen HIV-positive adults with CD 4 <100 for crypto before starting ART • Screen for cryptococcal antigenaemia by reflex laboratory/ clinician-initiated testing • No need to screen patients with prior diagnosis of cryptococcal meningitis • Patients with a positive cryptococcal antigen (Cr. Ag) blood test have disseminated cryptococcal disease - should be specifically evaluated for symptoms/ signs of meningitis
 • Pregnancy: Women of child-bearing age who")
Screening for Cryptococcal Disease in Adults (2) • Pregnancy: Women of child-bearing age who screen Cr. Ag-positive should have a pregnancy test prior to starting fluconazole (teratogenic) • Liver disease: Patients with evidence of clinical liver disease deserve careful monitoring because fluconazole may cause liver injury

Recommended Cryptococcal Prophylaxis Screening Antifungal prophylactic treatment ART Crs. Ag Screening test positive (bloodstream disease) but no evidence of meningitis Screening test positive with evidence of meningitis Oral fluconazole (800 mg per day) for 2 weeks, followed by standard consolidation and maintenance antifungal treatment) Intravenous antifungal treatment for 2 weeks, followed by standard consolidation and maintenance antifungal treatment Start after 2 weeks of antifungal treatment Start after 4 -6 weeks of antifungal treatment

Recommended Tuberculosis Prophylaxis • All HIV-positive adults and adolescents with no signs or symptoms suggestive of active TB are eligible for TB preventive therapy • Refer to page 90 of your participant manual to see a chart on IPT eligibility criteria

All HIV-infected non-pregnant adults and adolescents, whether on ART or not on ART, who have not completed a course of IPT before, and who have no signs or symptoms of active TB Pregnant women who have a negative TB Gene. Xpert, no TB symptoms, and a CD 4 less than 100 Former TB patients, provided TB treatment was completed successfully Who is not eligible for TPT? Who is eligible for TPT? Summary: TPT eligibility Confirmed or suspected active TB Pregnant women with CD 4 counts above 100 Active acute or chronic liver disease Symptoms of peripheral neuropathy History of adverse reaction to INH Excessive ETOH use

TPT Regimen and monitoring in Adults and Adolescents Dosage INH 5 mg/kg/day (max 300 mg/day) For 12 months in adults Pyridoxine 25 mg/day Comments No TST required to determine IPT duration Prevents peripheral neuropathy Clinical monitoring Adherence: Check adherence to TPT and provide ongoing counselling and patient education Side Effects: Early identification and management of side effects TB symptom screening: If symptoms positive, do a sputum TB Gene. Xpert and LPA, or culture and DST to detect any INH resistance Ensure IPT visits coincide with ART visits

IPT and children • Screen all children for TB at every visit. This should include: – Asking about TB contacts • Contact with a TB infected person within the last 12 months – Asking about TB symptoms • • Cough / fever / loss of weight / night sweats If positive TB contact and no active disease then offer IPT for 6 months – In all children <5 years – In all HIV-positive children up to 15 years • • Dose 10 mg/kg of INH with pyridoxine for 6 months Repeat with every TB exposure

Summary of the Differences in TPT for Adults and Children Adults • A child with a positive TB contact may be eligible for IPT, if less than 5 years old or HIV positive • IPT for 6 months • IPT with every new exposure to TB • Any HIV positive adult may be eligible for IPT, regardless of presence of known TB contact or not • IPT for 12 months • Usually only given once per lifetime
: 5")
Dosing Guide for Standard Regimen for TB Preventive Therapy Adolescents/Adults/Pregnant women Isoniazid (INH): 5 mg/kg/day (maximum 300 mg per day) Vitamin B 6 (pyridoxine): 25 mg/day Vitamin B 6 given with INH to prevent peripheral neuropath Issue 1 -month drug supply for 3 months, thereafter a 3 month supply can be issued Children INH 10 mg/kg/day Crush appropriate fraction of the 100 mg INH tablet and dissolve in water or multi-vitamin syrup before giving it to the child HIV-positive or malnourished, add pyridoxine daily for 6 months at the following dosages: <5 years of age: 12. 5 mg daily >5 years of age: 25 mg daily

Infants Born to Mothers with TB • The following neonates are eligible for IPT: • If they have been excluded on basis of clinical, radiological (CXR) and bacteriological (gastric aspirates) assessments and • Mother is non-infectious and has drug susceptible TB • If eligible, prescribe INH 10 mg/kg daily for 6 months

Who is not Eligible for TB Isoniazid Preventive Therapy? • People with confirmed or unconfirmed active TB • Patients with: • • active liver disease (acute or chronic) symptoms of peripheral neuropathy a history of adverse reaction to Isoniazid excessive alcohol use • People who are HIV positive but TST negative in pre. ART care • People who completed treatment of MDR- or XDR-TB • Patients who are ill and/or are in unstable condition

Isoniazid Side Effects and Management • Refer to page 92 of your participant manual to see a chart on Isoniazid side effects and management

Any Questions? Thank you!
- Slides: 25