Basic Burn Care A Presentation on Burn Products

Basic Burn Care A Presentation on Burn Products, Dressing Types and an Algorithm to Guide Your Care of the Burn Patient. Crystal Foster BSN, RN

Burn Products Description of commonly used burn dressing products. Xeroform Collagenase Adaptic Bacitracin Medihoney Mepilex AG Sulfamylon Silvadene Kerrafiber Elta Lite Lotion Silvasorb Gel Iodosorb Aloe Vera Gel

Xeroform and Adaptic • Non-adhesive dressings designed to cover a burn or graft protecting the area and helping retain proper moisture level needed for healing. • This are used with various topical agents including: bacitracin, collagenase, and medihoney. • Topicals can be applied directly to a single layer of the nonstick dressing and then applied to the wound.

Collagenase • Enzymatic debriding ointment used on partial thickness burn. • Apply to a single layer of xeroform/adaptic and cover the burn. • If not properly cleaned off daily a protein layer will prevent the wound from healing. • Depending on type of insurance coverage this ointment can be quite costly.

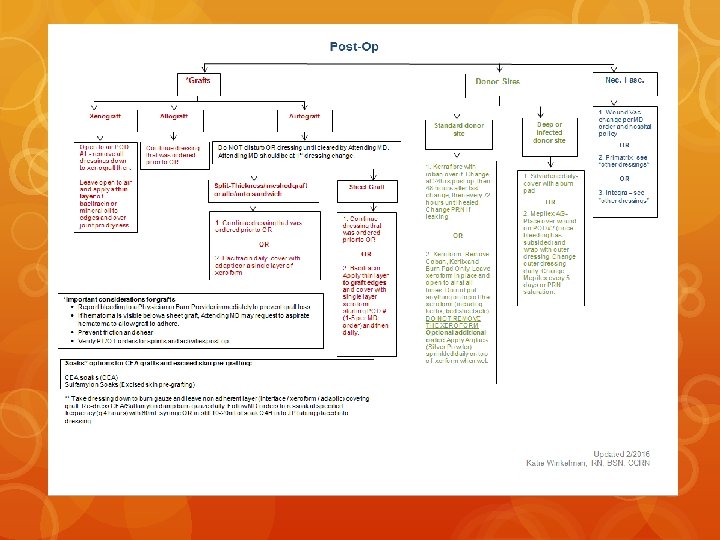
Bacitracin • Anti-bacterial ointment used on superficial burns and auto grafts. • Burns: Use with a single layer of xeroform to keep wound moist as the burn heals. • Meshed Autograft: Apply thin layer to graft and cover with xeroform/adapatic. • Sheet Autograft: Apply thin layer to edges only and cover with xeroform/adaptic.

Medihoney • Medical grade of honey that is used on deep partial thickness burns. • Helps remove dead tissue using autolytic debridement and lowering the p. H of the wound while maintaining a moist wound environment.

Mepilex AG • Antimicrobial silver foam dressing used for medium exudate producing wounds such as superficial/partial thickness burns and donor sites. • Sticky side is applied to the wound and helps adhere to surface, but will not stick to the wound. • Outer dressing is changed daily, but the Mepilex AG can remain in place for 5 days or until saturated.

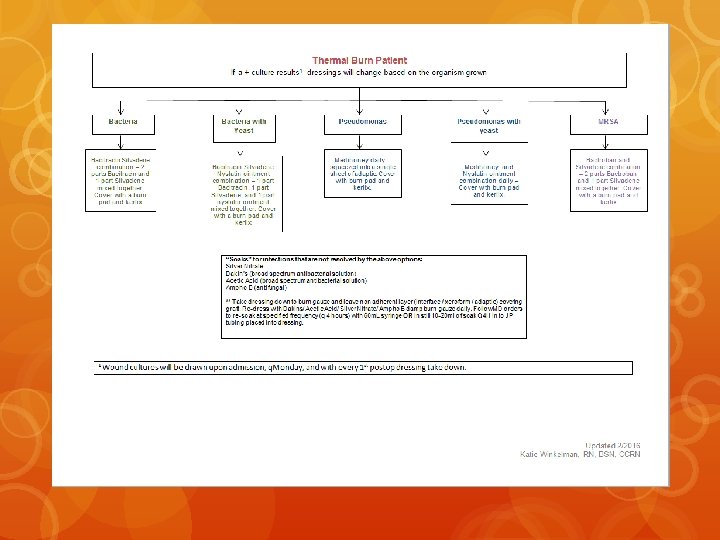
Silvadene • Antimicrobial cream that contains silver and is used on fullthickness burns. • Applied like “cake frosting” and covered with dry gauze. • Can cause pseudo eschar on top of burn if not properly removed daily.

Kerra. Fibre • Absorbent fibrous gel dressing that is used for moderate to high exudate producing wounds such as a donor site. • Kerra. Fibre is covered with a tegaderm and changed 24 hours post-op, then every 48 hours, and then every 72 hours until healed.

Elta Lite Lotion • Fragrance free lotion that is applied to healed burns, grafts and donor sites. • Apply as often as needed throughout the day. • Use with scar massage, circular medium pressure with pad of finger, to help with re-training nerve receptors for “normal touch”.

Silvasorb Gel • Silver impregnated gel used to manage bacterial burden. • Applied liberally and covered with xeroform and burn pads. • Used on TENS and Stevens Johnsons Syndrome patients.

Iodosorb • Antibacterial and absorbent paste applied to mild exudate producing wounds. • Used on patients with frostbite. • Covered with dry gauze and changed daily.

Aloe Vera Gel • Used on frostbite patients. • Covered with adaptic and changed daily.

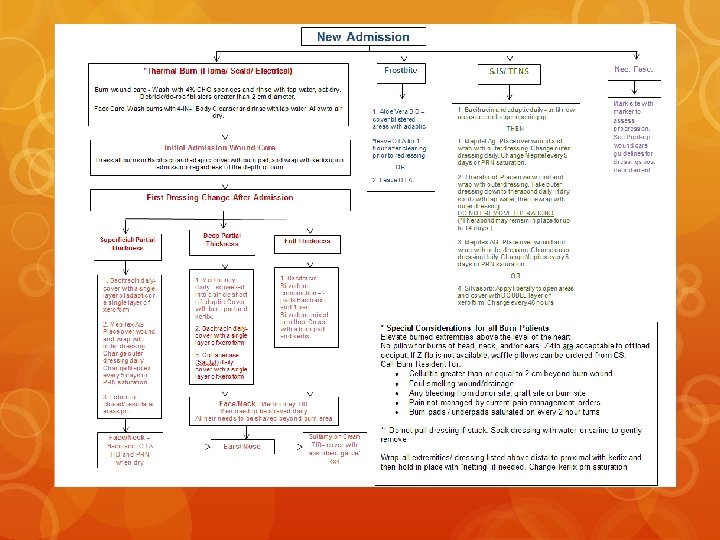
Basic Burn Care • We see various types of burns/grafts in the outpatient burn setting. • Burn care can be performed by RNs and medical assistants that have completed the competency. • RNs are responsible for the first post-operative dressing take down. • After this point the skin graft is adhered and can be considered new skin. The MA can perform dressings at this point.

Basic Burn Care Dressing Removal/Cleaning • When removing any dressing-”If it sticks, quit!” Get some water or saline and wet the dressing, let it sit and then gently continue to remove. • If it is still difficult to remove or too painful for the patient alert the charge nurse. • All burns/graft sites/donor sites from the neck down should be cleansed with 4% chlorhexidine gluconate sponges. • Rinse thoroughly Above the neck wounds should be washed with gentle soap and water to prevent eye injury. • Remember to change gloves before applying new dressing.

Basic Burn Care Debridement • Gentle debridement with the washcloth during cleansing can be performed by medical assistants. • Mechanical debridement should be performed only by RN or medical provider.

Basic Burn Care Reapplying the Dressing • Ointments such as bacitracin, collagenase and medihoney can be applied directly to non-adherent dressings xeroform or adaptic. • This is not as painful for the patient and ensures adequate coverage of the affected area. • Secure with conform, better for fingers/hands, or kerlix. ACE wrap is also commonly used. Wrap from distal to proximal using “Figure 8” wrapping style.

Questions and Answers! Please ask me anything you don’t understand-there is no such thing as a stupid question! This is intended to be an introductory teaching tool. Medical assistants and new Burn Clinic nurses will be required to have more in-depth teaching and competency check-offs with clinic charge nurse.
- Slides: 23