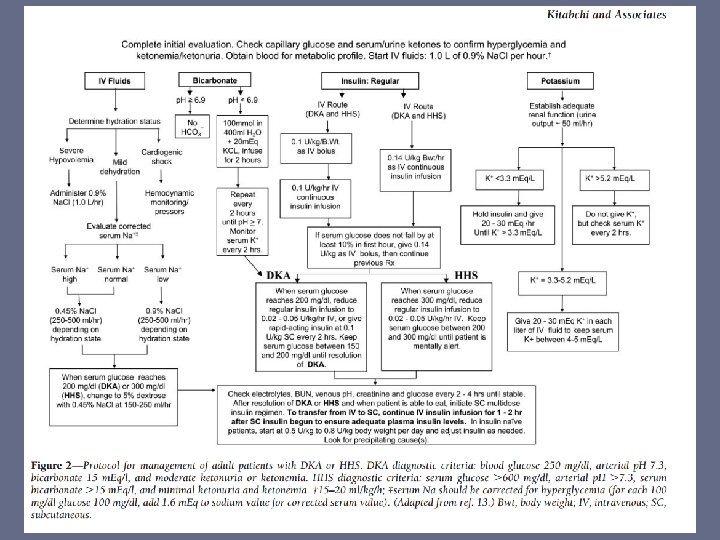
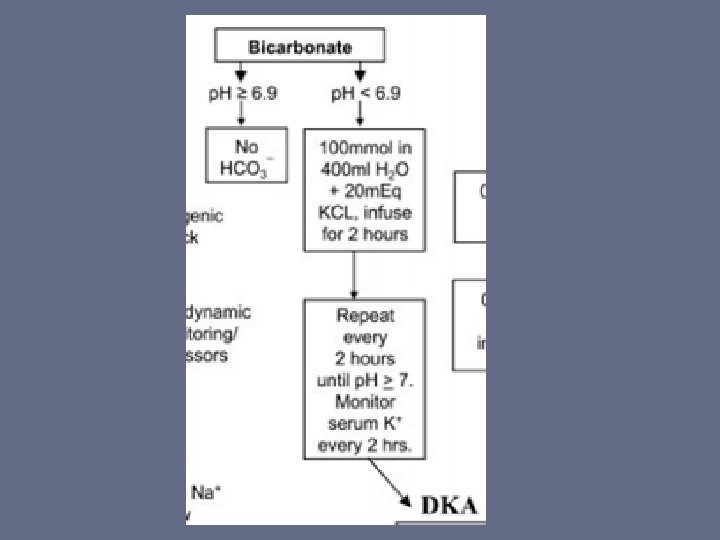
Base Treatment for Metabolic Acidosis due to DKA

Base Treatment for Metabolic Acidosis due to DKA and Sepsis Nicholas Busch Henry Ford Hospital Emergency Medicine Grand Rounds September 17 th, 2015

So who should get an AMP or two? • 24 yo male with DKA – p. H 6. 90 – p. CO 2 45 – HCO 3 8

So who should get an AMP or two? • 65 yo with septic shock – p. H 7. 10 – p. CO 2 42 – HCO 3 10

Objectives • Quick Acid-Base review • Discuss the hemodynamic effects of base therapy • Discuss evidence for base therapy in: – DKA – Lactic acidosis/sepsis • Not covered: Pediatrics, respiratory acidosis, toxic ingestions, RTA and other non-AG acidosis

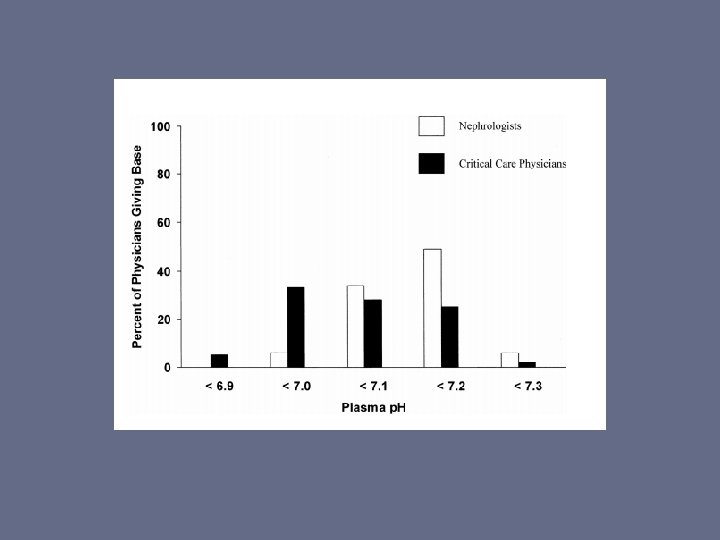
Who gives sodium bicarb therapy?

Patient’s with lactic acidosis -67% of critical care physicians -86% of nephrologists Patient’s with ketoacidosis -28% of critical care physicians -60% of nephrologists

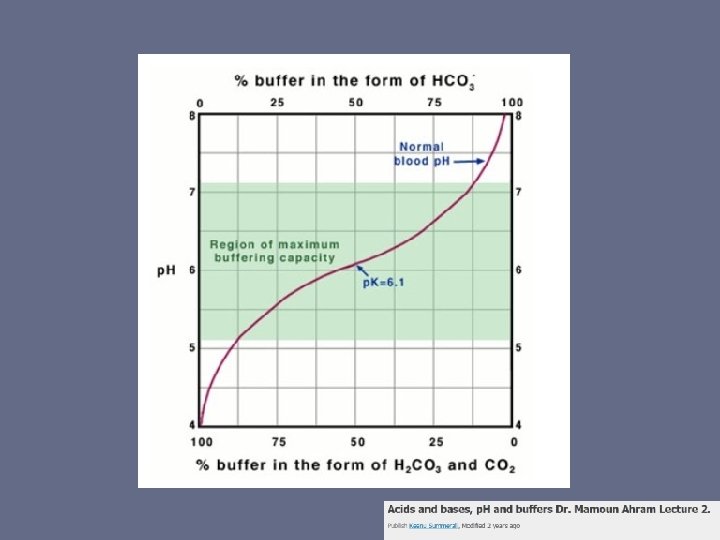
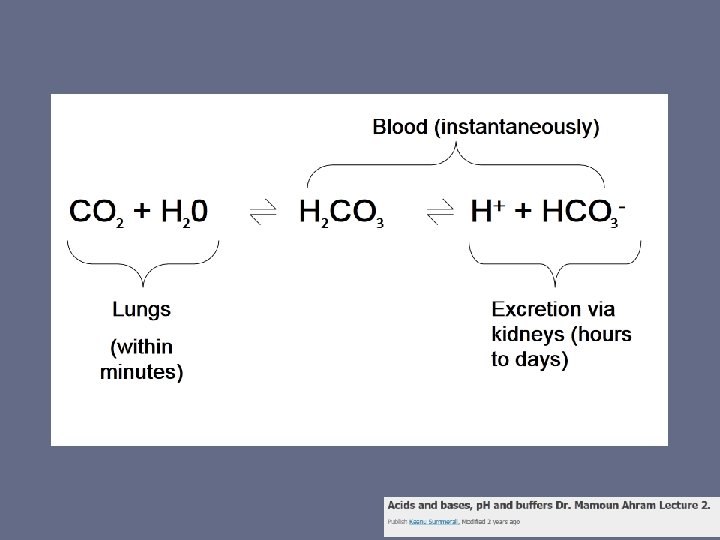
VERY Quick Acid-Base Review • CO 2 + H 20 H 2 CO 3 HCO 3 + H+ • Henderson Hasselbalch • p. K curve
 – NOT standardized unit of")
Also what’s an AMP? ? • Ampule (amp, ampoule) – NOT standardized unit of measure – “Single dose of medication pre-packaged in an injectable glass or plastic vessel”

An “amp” of Bicarb • 8. 4% Sodium Bicarbonate – 50 m. Eq Na+, 50 m. Eq HCO 3– p. H 8. 0 – 1 m. L is 84 mg

Framing the Question

Proposed Rationale for Base Therapy Use: 1. A low p. H, in and of itself, is harmful (most notably by impairing cardiovascular function). 2. Sodium bicarbonate can increase the p. H when infused IV. 3. Raising the p. H with sodium bicarbonate improves cardiovascular function or some other relevant outcome. 4. Any adverse effects of sodium bicarbonate are outweighed by its benefits

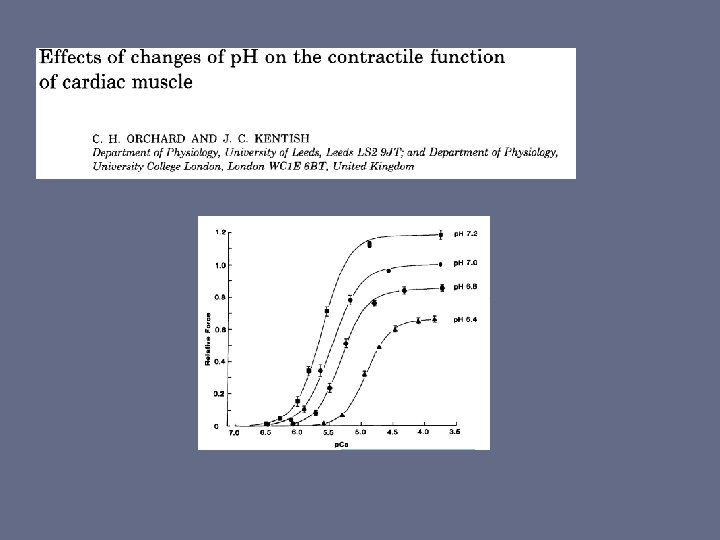
“A low p. H, in and of itself, is harmful (most notably by impairing cardiovascular function)” -Isolated animal heart muscle - acidosis generally reduces contractile function -Human ventricular tissue showed modest reduction in contractility -Whole animal models: contractility constant, decrease slightly or rise and then fall -ARDS treatment : permissive hypercapnia tolerated to 7. 15 and below -Protective effect? – reduced cell death in hepatocytes exposed to anoxia

“Sodium bicarbonate can increase the p. H when infused IV” • Most animal studies show arterial p. H will rise

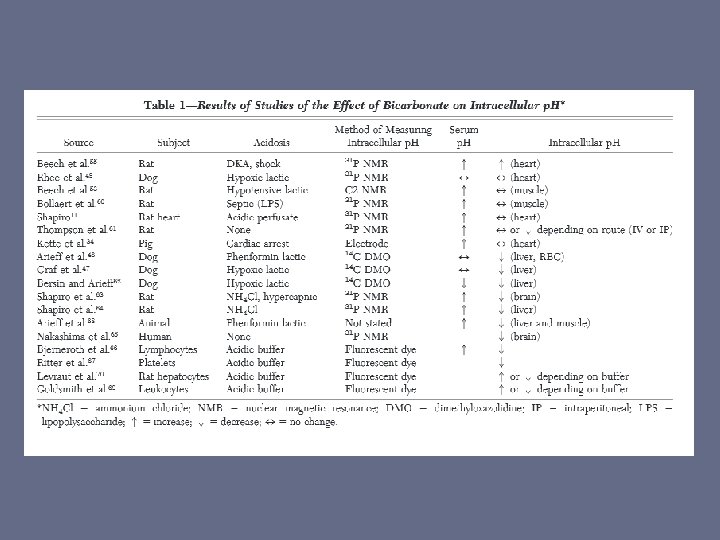
What about the intracellular p. H? • Multiple compartments with different degrees of permeability – Cerebral spinal fluid • Bicarb shown in dog models to LOWER CSF p. H – Intracellular Space

“Raising the p. H with sodium bicarbonate improves cardiovascular function or some other relevant outcome” • 2 studies in humans with lactic acidosis and getting continuous vasoactive infusions – No change in hemodynamics or catecholamine responsiveness – HR, CVP, PAP, Sc. Vo 2, wedge pressure, or CO – Still negative results with most acidotic (6. 9 -7. 2)

“Any adverse effects of sodium bicarbonate are outweighed by its benefits” • Negative side effects – Fluid and sodium overload – Lowers p. O 2 and oxygen delivery – Increased lactate concentrations – Lowers calcium • LV contractility varies directly with ionized calcium concentration • Clinical significance has not been demonstrated

More direct question… • Does Sodium Bicarbonate improve outcomes for patients with severe DKA or lactic acidosis from sepsis?


- 24 patients received 120+/-40 mmol sodium bicarbonate. - Two groups were similar at admission with regard to clinical and biological parameters - Prospective, randomized trial - No difference could be demonstrated between the two groups

- 21 adult patients, DKA with p. H 6. 9 to 7. 14 - No significant differences in - Glucose or ketone levels - Increase in p. H or. HCO 3 in blood or CSF - Time to glucose 250, p. H 7. 3, bicarb to 15

“We conclude that in severe diabetic ketoacidosis (arterial p. H 6. 9 to 7. 14), the administration of bicarbonate does not affect recovery outcome variables as compared with those in a control group. ”

- 12 case control studies - 3 RCT with 73 patients - No Significant Difference: - Hospitalization - Mortality - No studies had any patients with p. H <6. 85 “The evidence to date does not support the use of bicarbonate administration for the emergent treatment of DKA” “There also is insufficient evidence to justify the recommendation of bicarbonate administration in more extreme acidemia of p. H < 6. 90. ”

• Retrospective cohort study • 86 adult patients, DKA, p. H <7. 0

Table 2. Outcome Comparison. “…the use of sodium bicarbonate therapy did not improve time to resolution of acidosis or hospital length of stay in severe DKA. ” Bryson Duhon et al. Ann Pharmacother 2013; 47: 970 -975 Copyright © by SAGE Publications

Conclusions on DKA in adults: • No data on p. H <6. 9 – ADA recommends use • No indication for routine use in p. H greater than 6. 9

What about lactic acidosis in sepsis?
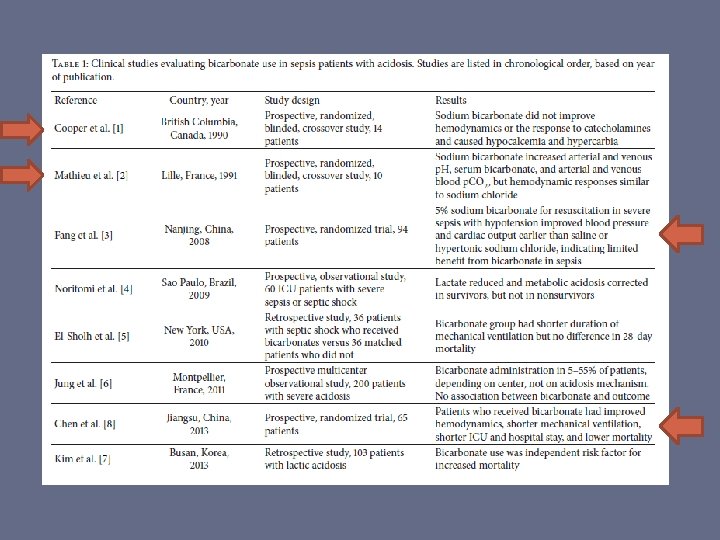

• Double blind, RCT, 65 patients with septic shock • 2 groups – staged and control • Bicarbonate improved lactate, p. H, Sc. VO 2, CI

“We recommend against the use of sodium bicarbonate therapy for the purpose of improving hemodynamics or reducing vasopressor requirements in patients with hypoperfusion-induced lactic acidemia with p. H ≥ 7. 15 (Grade 1 B). ” @2013 Society of Critical Care Medicine, European Society of Intensive Care Medicine. www. survivingsepsis. org

Surviving sepsis sources: • 14 + 10 patients with PA Catheters • Sodium Bicarbonate increased p. H, HCO 3, p. CO 2. Decreased Ca • No difference in any hemodynamic measures HCO 3 vs Na. Cl

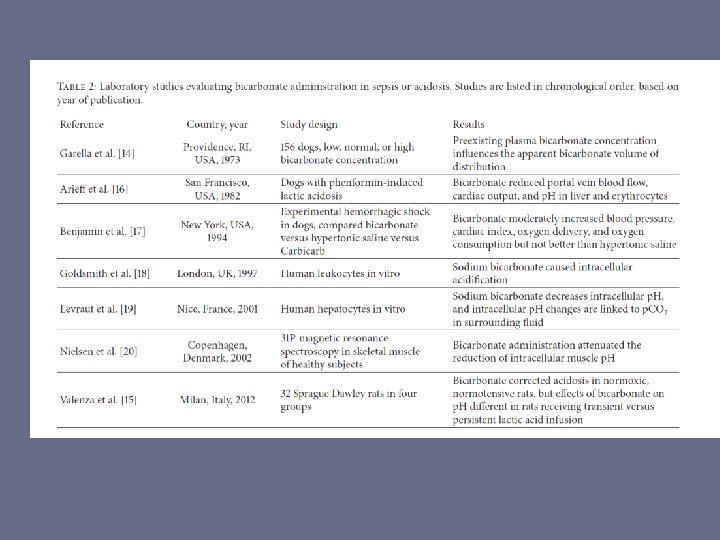
- Review article after surviving sepsis guidelines 2008 - Similar data to previous - Advocate no treatment “p. H <7. 0 or less” - Plan for slow infusion and clearing CO 2

Conclusions in lactic acidosis from Sepsis: • Clinical outcomes not yet shown to be improved • Surviving Sepsis Guidelines recommend considering when p. H <7. 15 • Consider negative effects – Increased p. CO 2, decreased calcium, decreased oxygen delivery

So how to give if you decide to: • Bicarb deficit – Half of deficit in 4 hours, rest over 24 hours

Questions? “IT’S ALL ABOUT THAT BASS” • Sources available upon request.
- Slides: 46