BASAL INITIATION AND KNOWLEDGE SHARING LINKS INSULIN INITIATION
 INSULIN INITIATION AND OPTIMIZATION STRATEGIES WITH BASAL INSULINS")
BASAL INITIATION AND KNOWLEDGE SHARING (LINKS) INSULIN INITIATION AND OPTIMIZATION STRATEGIES WITH BASAL INSULINS Dr. Ravi Kant M. D (Medicine), P. Gd(Preventive cardiology), Master (European and American Heart Association), P. Gd. Diabetology (Boston University) Associate Professor Department of Internal Medicine All India Institute of Medical Sciences Rishikesh, Uttarakhand Chair Texila American University

STARTING BASAL INSULIN THERAPY IN DIABETES

When to Consider Starting Insulin Anytime a patient with diabetes. . . • Is significantly hyperglycemic • Has inadequate glycemic control on otherapies • Is intolerant of oral hypoglycemic/other agents

• • • Requires high-dose glucocorticoids Is hospitalized with an acute myocardial infarction or another acute illness Is in a perioperative/intensive care setting

Decline in -Cell Function with Diabetes Progression: UKPDS • • At diagnosis of diabetes: Explain the natural history of progressive decline in beta-cell function That insulin is one of the options available to manage diabetes Insulin may the best way for maintaining glucose control in the longer term Most people with diabetes eventually require insulin therapy

What do the guidelines state about when to start insulin therapy? All guidelines suggest insulin as an option for initial therapy in those with very high A 1 c (> 9 – 10%), especially with symptoms. ADA/EASD: Consider as option if A 1 c > target after metformin ± 1 or 2 otherapies AACE: Generally recommended after metformin + 2 otherapies IDF: As an option as third or fourth line therapy NICE: Start after metformin and sulfonylurea
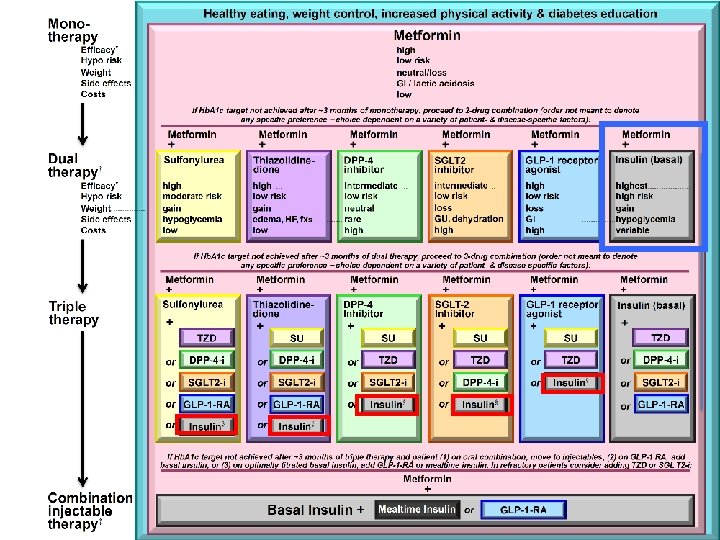

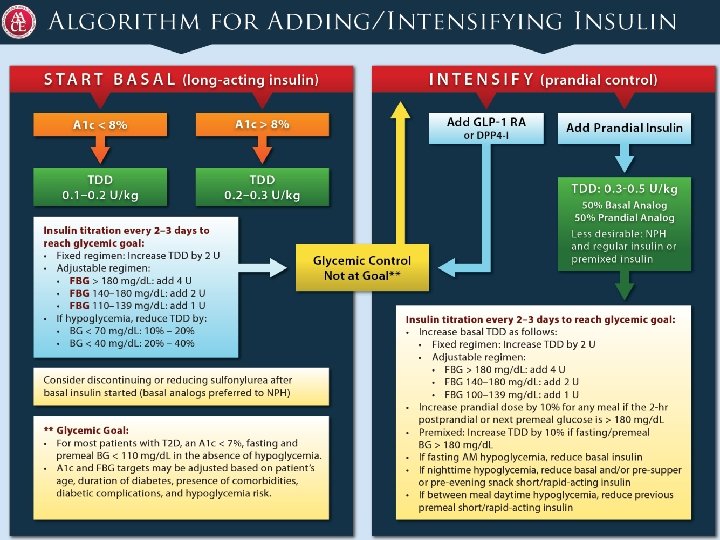
ADA/EASD Approach to starting & adjusting insulin in T 2 DM

ADA/EASD: Approach to starting basal insulin Start: 0. 1 – 0. 2 U/kg/day. Higher doses 0. 3 – 0. 4 U/kg/day may be used when severely hyperglycemic Adjust 10 – 15% (2 – 4 units) once or twice weekly to reach FBG goal Hypoglycemia: Determine and address cause. Decrease dose by 10 – 20%

Addition of Basal Insulin Basal insulin will counteract hepatic glucose output between meals and overnight Use of NPH, glargine, or detemir insulins recommended by ADA/EASD, AACE, IDF � NICE recommends NPH as initial basal. Analogues can be used in pts needing BID NPH, with hypoglycemia or need of assistance with injections Most individuals with type 2 diabetes will achieve adequate control with the addition of basal insulin alone NICE: consider twice-daily premixed particularly if A 1 c≥ 9. 0%

A Balanced Approach for Insulin Therapy in T 2 DM

Relevance of Different Components of Dysglycemia: FPG & PPG contributions by Hb. A 1 c level Total hyperglycemia (%) Postprandial Hyperglycemia Fasting or Basal Hyperglycemia On baseline OADs, fasting hyperglycemia dominates over a wide range of A 1 C levels Total hyperglycemia (%) A 1 C <8. 0–<8. 5–<9. 0–<9. 5 Following treatment intensification, fasting hyperglycemia contributes >40% to overall hyperglycemia A 1 C <6. 5–<7. 0–<7. 5–<8. 0

Fix Fasting First PP BG Basal Insulins Elevated Fasting Hyperglycemia and HGO Normal Fasting Blood Glucose Hence need to fix fasting first

Glycemic Changes with Basal Insulin by Baseline OAD Use† -1. 4 8. 9 0/1 OAD Hb. A 1 c -1. 6 -1. 8 8. 7 2 OADs 9. 1 MET only -1. 7 p = 0. 0198 8. 8 SU only 8. 7 MET + SU -1. 7 Mean Hb. A 1 c at baseline -2. 0 p = 0. 0006 -2. 2 7. 1 7. 0 6. 9 7. 1 7. 0 54. 7 52. 7 68. 1* 50. 4 56. 4 † Pooled analysis , * p = 0. 0001 vs all taking SU Mean Hb. A 1 c at 24 weeks Hb. A 1 c <7% (% patients)

Hypoglycemia and Weight with Basal Insulin by Baseline OAD Use: Pooled Analysis 40 p=0. 0006 35. 4 34. 7 30 20 10 0 18. 8 17. 3 9. 0 0/1 2 MET SU MET OAD only + SU Baseline OAD number/class (kg) p=0. 0122 4 Change in body weight (% pts with BG < 50 mg/d. L) Confirmed hypoglycemia 50 No significant difference in change in body weight Significantly less hypoglycemia in MET only patients p=0. 9547 p=0. 1830 3 2 2. 3 2. 1 2. 0 1. 6 2. 0 1 0 0/1 2 MET SU MET OAD only + SU Baseline OAD number/class p values were calculated from an analysis of variance model with study and baseline OAD class as factors and baseline Hb. A 1 c or bodyweight as a covariate

When starting insulin therapy Patient education � Proper technique for administration of insulin � Frequent self-monitoring � Teach dose titration � Prevention and management of hypoglycemia � Management of acute changes in glucose Continuous telephone support

What to do with Other Medications? When basal insulin is added: � Provided no contraindications to continued use � Continue metformin � Probably continue incretin-based therapy, SGLT-2 inhibitor � Reduce (or discontinue) thiazolidinedione � Most recommend continue sulfonylurea therapy (but discontinue if hypoglycemia)

Insulin Action Profiles Rapid-acting analogues Plasma Insulin Levels Regular insulin NPH Long-acting analogues 0: 00 2: 00 4: 00 6: 00 8: 00 10: 00 12: 00 14: 00 16: 00 18: 00 20: 00 22: 00 24: 00 Time
 7 6")
Currently Available Basal Insulins Insulin Activity, GIR, mg/kg/min Within-Patient Variability (Time-Action Profiles) 7 6 5 4 3 2 1 0 NPH 0 4 8 12 16 20 24 7 6 5 4 3 2 1 0 Detemir 0 4 8 12 16 20 24 Elapsed Time, hours 7 6 5 4 3 2 1 0 Glargine 0 4 8 12 16 20 24

Treat to Target Study Insulin Glargine vs NPH Insulin Added to Oral Therapy • 9 Insulin glargine NPH insulin • 8 Mean A 1 C (%) • 7 Target A 1 C (%) • 6 • 0 • 4 • 8 60% reach target A 1 C < 7% • 12 Weeks • 16 • 20 • 24

Events per Patient-Year Symptomatic Hypoglycemia by Time of Day Glargine Basal insulin 1. 4 1. 2 * * * 1. 0 * 0. 8 NPH insulin * * * 0. 6 0. 4 0. 2 0 20 22 24 2 4 6 8 10 12 14 16 18 Time of Day (hour) Hypoglycemia defined as PG 72 mg/d. L, by hour *P < 0. 05 vs glargine.
 Adequately mix the")
When using Human NPH insulin, patients should be advised to: 1) Adequately mix the suspension to minimize variability 2) Ingest a bedtime snack to avoid nocturnal hypoglycemia

Start Insulin Early: Baseline A 1 c Affects Success of Basal Insulin Rx A 1 c change from baseline % of patients <7% A 1 c 75% of participants with baseline A 1 c <8% attained <7%

ORIGIN Trial: Glargine vs Standard Care in Patients at High Ris for CVD (DM, IFG, IGT) No difference in CV Outcomes

ORIGIN Trial: Median A 1 C Levels Remain relatively stable for up to 7 years

This suggests that early use of insulin can provide durable glucose control with low risk for hypoglycemia and weight gain
 % Any Non-severe 1 or more episodes Severe")
ORIGIN: Hypoglycemia & Weight Glargine (N=6264) % Any Non-severe 1 or more episodes Severe 1 or more episodes Weight Change Since Randomized 57 Standard (N=6273) /100 py % 17 25 /100 py 5 6 1. 0 2 P <0. 001 0. 3 <0. 001 Glargine Standard P 1. 6 kg -0. 5 kg <0. 001

Physicians Delay Intensifying Therapy for Months, Especially Initiating Insulin 9. 5% A 1 C>8% (months) A 1 C>7% (months) N=2319 4 16 N=3394 17 N=513 12 N=982 26 37 26 51

Provider Barriers To Insulin Therapy • Initiating insulin takes time • Management more complicated • Lack of resources • Increased risk for hypoglycemia • Fear of increased CVD risk – ORIGIN study refutes this • Weight gain, worsening insulin resistance • Patient resistance

Reasons Patients Avoid Insulin 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Lack of knowledge/understanding Cultural taboos and family beliefs Fear of needles or injection pain Fear of hypoglycemia Fear of weight gain Inconvenience Diabetes seen as worse or more serious Personal failure Insulin causes complications Insulin will take over my life: constant demands and decision-making

Strategies for Overcoming Barriers Involve patient in therapeutic decision-making process Frame message properly (don’t “blame” patient) Discuss real risk of hypoglycemia (low) Address cultural taboos and family beliefs Fear of weight gain: minimize w/ diet, exercise, other medications Starting insulin: get help from you office staff: consider group instruction Needle phobia: show fine needles, pens Begin therapy with simple regimen

Starting Insulin: Talking Points Insulin is most “natural” therapy, replacing what is missing (use thyroid hormone analogy). No drug interactions It prevents complications It can be successfully used in most patients with minimal weight gain and hypoglycemia (especially when given early) Offer to let them stop in a month, if they don’t feel like it is helping them

Optimizing medication adherence in type 2 diabetes Patient education Role of medications, hypoglycemia, need for SMBG � Essential for successful implementation of insulin therapy Incorporation of medication regimen into daily routine Established patterns help patients remember to take meds Assess patient’s preferences and provide strategies to tailor the timing of taking his medication to fit their lifestyle Medication adherence is higher in QD vs more frequent
")
Practical Pointers Insulin pens preferred 3: 1 by patients (Don’t forget the pen needles) Have patient give first injection in the office Discuss prevention and treatment of hypoglycemia Provide a self titration schedule Follow up in 1 -2 weeks to review SMBG, dosing data (good time to have patient see a staff person to reinforce education and evaluate titrations

Cases

Case 1 Mrs. S is a 63 year old female with 8 year history of type 2 diabetes, with past history of congestive heart failure, hypertension, hyperlipidemia Current treatment: Metformin 850 mg BID, Glipizide 10 mg QD, Losartan 100 mg daily, Furosemide 20 mg QD, Atorvastatin 20 mg QHS Testing BG QD, ranging 160 – 200 She is reluctant to start insulin

Case 1 - continued Ht – 157 cm, Wt – 64 kg, BMI – 26 BP – 134/75, P – 76, normal eye grounds, cardiac exam, 1+ pedal edema, intact sensation Labs - A 1 c – 8. 1%, e. GFR – 59, Lipids – TC – 155 mg/dl, HDL-C – 37 mg/dl, TG – 185 mg/dl, LDL-C – 81 mg/dl

What is your recommendation? Titrate glipizide Add pioglitazone Add premix insulin Add basal insulin

What is your recommendation? Titrate glipizide – A 1 c very unlikely to reach target Add pioglitazone – relatively contraindicated with CHF Add premix insulin – at her current A 1 c, associated with higher weight gain and hypoglycemia, with no glycemic advantage over glargine Add basal insulin – best choice for her

How would you try to convince her to start insulin?

Strategies for Overcoming Patient Barriers for Starting Insulin Involve patient in therapeutic decision-making process Frame message properly (don’t “blame” patient) Discuss real risk of hypoglycemia (low) Address cultural taboos and family beliefs Fear of weight gain: minimize w/ diet, exercise, other medications Needle phobia: show fine needles, pens Begin therapy with simple regimen Offer a one month trial

Starting Insulin Glargine Starting Dose? Timing of Insulin Administration? Instructions for SMBG? Instructions for self-titration? Follow up?
 Timing of Insulin Administration?")
Starting Insulin Glargine Starting Dose? 12 units (0. 2 U/kg) Timing of Insulin Administration? Help her determine the time that fits into her schedule Instructions for SMBG? Test daily in AM Instructions for self-titration? Set target BG Depending upon her comfort level: � 2 units very 3 days OR � 1 units every day

Starting Insulin Glargine – Follow up � Recommend follow up in 1 – 2 weeks by telephone, email or in person to make sure she is titrating appropriately � Next visit in 4 – 6 weeks to review progress

Case 2 Mr. K is a 62 year old male with 9 year history of type 2 diabetes, complicated by neuropathy and coronary artery disease. Also has hypertension and hyperlipidemia Current medications: Metformin 500 mg BID, Glimepiride 4 mg daily, Insulin glargine 20 units QD, Lisinopril-HCTZ 20/25, Metoprolol XL 50 mg daily, Atorvastatin 40 mg QD, ASA 81 mg QD. Tests BG QAM – range 160 - 200
 He admits that he quit titrating because he was afraid he")
Case 2 (continued) He admits that he quit titrating because he was afraid he was taking too much insulin. Ht – 170 cm, Wt – 73 kg, BMI – 25. 3 BP – 125/70, P – 64, normal eye grounds, cardiac exam, absent pedal sensation Labs - A 1 c – 8. 5%, e. GFR – 60, Lipids – TC – 135 mg/dl, HDL-C – 34 mg/dl, TG – 205 mg/dl, LDL-C – 60 mg/dl

What would you recommend for treatment? What is your A 1 c target? Titrate metformin Titrate glimepiride Add pioglitazone Add rapid acting insulin Titrate glargine insulin further

What do you recommend? What is your A 1 c target? By age, A 1 c < 7%, but with history of CAD, need to avoid hypoglycemia. Titrate metformin – unlikely to get to target Titrate glimepiride – unlikely to get to target Add pioglitazone – relative contraindication with insulin Add rapid acting insulin – is an option, but glargine is not at optimal goal. Currently at 0. 27 U/kg (Treat to target average 0. 5 U/kg) Titrate glargine insulin further

Titration of Insulin Glargine Ensure that the timing of insulin administration fits into patients lifestyle (AM vs HS) Patients should know their target for fasting SMBG (generally < 100 mg/dl) Instruct them that starting dose is low and that average dose is 0. 5 U/kg Consider using titration of 1 unit per day until fasting BG reaches target

Case 3 Mrs. D is a 72 year old female with 11 year history of type 2 diabetes. She has hypertension, hyperlipidemia, stage 3 CKD, peripheral neuropathy, history of CVA. Current medications: Glipizide 10 mg QAM, NPH 15 units BID, Lisinopril 10 mg QAM, Chlorthalidone 15 mg QD, Atorvastatin 20 mg QD, ASA 81 mg daily She reports awakening frequently at 2 am with tremors and sweats
 Ht – 150 cm, Wt – 62 kg, BMI – 27")
Case 3 (continued) Ht – 150 cm, Wt – 62 kg, BMI – 27 BP – 125/70, P – 64, normal eye grounds, cardiac exam, absent pedal sensation Labs - A 1 c – 8. 8%, e. GFR – 35, Lipids – TC – 148 mg/dl, HDL-C – 40 mg/dl, TG – 195 mg/dl, LDL-C – 69 mg/dl

What is your recommendation? What is your A 1 c target? What would you do with her hyperglycemic regimen? � Add metformin � Titrate Glipizide � Titrate NPH � Switch to Glargine, with titration to goal

What is your recommendation? What is your A 1 c target? – with her age and comorbidities, it would be appropriate to target an A 1 c < 8. 0% What would you do with her hyperglycemic regimend? � Add metformin – relative contraindication with e. GFR � Titrate Glipizide – unlikely to reach goal – already having probable hypoglycemia � Titrate NPH – likely to increase her probable hypoglycemia � Switch to Glargine, with titration to goal – best answer

Events per Patient-Year Treat to Target: Symptomatic Hypoglycemia by Time of Day Glargine Basal insulin 1. 4 1. 2 * * * 1. 0 * 0. 8 NPH insulin * * * 0. 6 0. 4 0. 2 0 20 22 24 2 4 6 8 10 12 14 16 18 Time of Day (hour) Hypoglycemia defined as PG 72 mg/d. L, by hour *P < 0. 05 vs glargine.

Transitioning from NPH to Glargine If QD – convert 1: 1 and titrate If BID – lower dose by 20% and titrate Older individuals may need additional support for titration – family member, home nurse, more frequent office visits. Reinforce consistency of diet and exercise

Summary Guidelines recommend insulin therapy after failure of one or more non-insulin therapies or when A 1 C ≥ 9% Start simple with basal insulin Treatment with glargine insulin has lower incidence of nocturnal hypoglycemia than human NPH insulin and analogue premix insulin Patient-specific considerations regarding insulin use � Individualized glycemic targets � Availability of glucose monitoring � Socieconomic considerations

Education of prevention and management of hypoglycemia Promote continued adherence to a healthy diet and regular physical activity Be enthusiastic and confident to encourage and empower your patients!

THANK YOU
- Slides: 59