BASAL GANGLIA MOTOR PATHWAYS DR GALLATZ KATALIN Basal

BASAL GANGLIA MOTOR PATHWAYS DR. GALLATZ KATALIN

Basal Ganglia - Components of the basal ganglia - Functional circuitry of the basal ganglia e. g. , direct and indirect pathways, transmitters - Circuitry involved in movement disorders
")
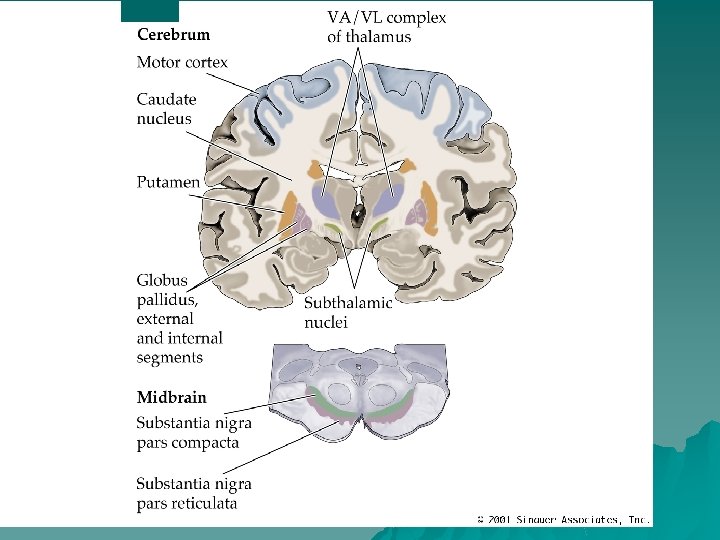
Basal Ganglia 1. Striatum Caudate nucleus Putamen 2. Pallidum Globus pallidus external segment (GPe) Globus pallidus internal segment (GPi) 3. Ventral pallidum accumbens nucleus olfactory tubercle 4. Substantia Nigra Pars compacta (SNc) Pars reticulata (SNr) 5. Subthalamic nucleus (STN)

Main components of basal ganglia: STRIATUM - caudate nucleus, putamen, globus pallidus, - subthalamic nucleus, and the substantia nigra. -nucleus accumbens and ventral pallidum
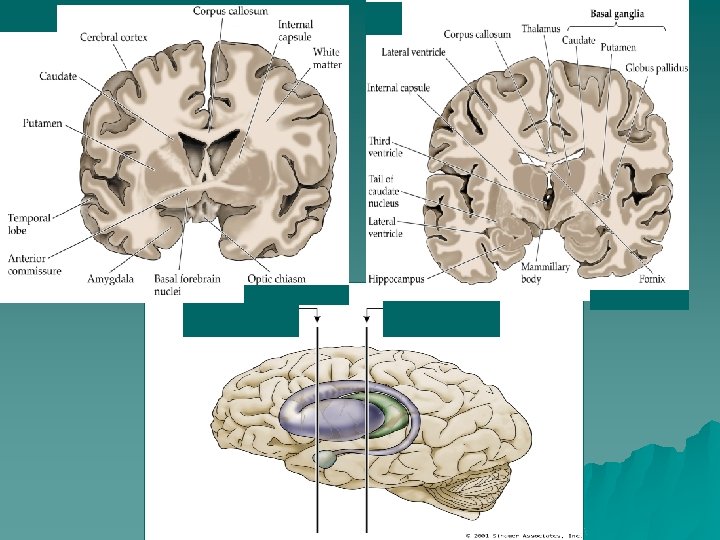

BASAL GANGLIA

Functions of basal ganglia u Motor functions u Control of the eye movements - basal ganglia (BG) have important role in controlling eye movements. SC receives a strong inhibitory projection from the substantia nigra pars reticulata u Motivation - (ventral tegmental area → nucl. accumbens → prefrontal cortex; dopamin; drug abuse and addiction) u Cognitive functions: - decision making, choosing the appropriate behaviour (nucl. basalis; acetylcholin; Alzheimer’s disease) u Emotional reactions (amygdala-ventral striatum)

ROLE OF THE BASAL GANGLIA IN MOTOR SYSTEM Basal ganglia are involved in generation of goal-directed voluntary movements: • Motor learning • Motor pattern selection

Input to basal ganglia

Regions of cortical input to the basal ganglia Lateral view Medial view

Output from the basal ganglia Midbrain

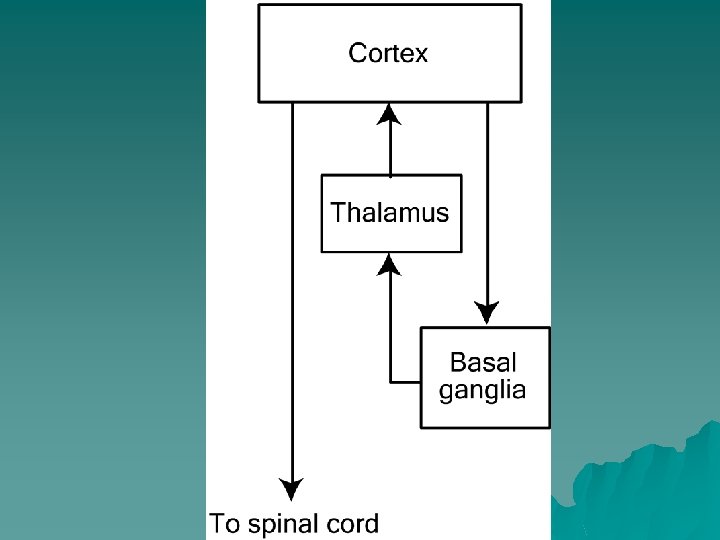
Input Output and internal circuitry

Medium-spiny neuron in the basal ganglia SN

Synaptic input to and output from striatal medium spiny neurons Smith and Bolam 1990

Medium spiny neuron projections
 Inhibition (GABA) * VA/VL GPe Disinhibition")
Direct pathway: Cortex facilitates movements Striatum Excitation (glutamate) Inhibition (GABA) * VA/VL GPe Disinhibition STN *GPi/SNr Brain stem/ Spinal cord * tonically active ~100 Hz Modified from Wichmann and Delong, Curr Opin Neurobiol. 6: 751 -758, 1996.

Basic Circuit of Basal Ganglia Cerebral Cortex + DIRECT PATHWAY Striatum + Gpi Gpe VA/VL thalamus INDIRECT PATHWAY + Subth

Direct and indirect pathways

Involvement of the cerebellum Frontopontine tract Temporooccipitopontine tr. pontocerebellar tract Cerebellothalamic tract
 Limbic loop")
Basal ganglia loops – motor and non-motor Motor loop Prefrontal loop (Associative) Limbic loop

Motor control systems in the cortex PRIMARY MOTOR CORTEX – source of pyramidal tract neurones PREMOTOR CORTEX - important in motor coordination. - lesions cause impairments in stability of stance, gait and hand coordination From: Biopsychology, JPJ Pinel

Primary motor cortex – somatotopic organization From: Biopsychology, JPJ Pinel

MOTOR SYSTEM PYRAMIDAL, EXTRAPYRAMIDAL? ? ?

Motor pathways The alpha-motoneuron is the final common pathway

Pyramidal and extrapyramidal systems can only be separated anatomically but not functionally!! None of the two systems can work properly alone, they constitute one motor system together!!!

PYRAMIDAL SYSTEM ►Pyramidal organizer system is the chief and executor of voluntary movements. CORTICOSPINAL AND CORTICOBULBAR (CORTICONUCLEAR TRACT) TO THE MOTOR NUCLEI OF THE CRANIAL NERVES
 uncrossed (ventral)")
crossed (lateral) uncrossed (ventral)

THE PYRAMIDAL SYSTEM u Pyramidal system is the chief organizer and executor of voluntary movements. u Upper motoneurons are located in the cerebral cortex, while lower motoneurons can be found in the motor nuclei of cranial nerves or in the spinal ventral horn. u Descending axons of upper motoneurons that terminate in the motor nuclei of cranial nerves and in the spinal cord constitute the corticonuclear (corticobulbar) and corticospinal tracts. u The corticonuclear tract reaches the lower motoneurons of both sides (bilateral innervation), while corticospinal fibres target the lower motoneurons of the opposite side only (crossed pathway).
 Rubrospinal tr. u Extrapyramidal system includes all")
Motor pathways from the brainstem (EXTRAPYRAMIDAL TRACTS) Rubrospinal tr. u Extrapyramidal system includes all the motor centres and pathways that lie outside the pyramidal system and are beyond voluntary control.

Efferent extrapyramidal pathways rubrospinal tr. tectospinal tr. reticulospinal tr. Vestibulospinal tr. olivospinal tr. ? ? ? from Dr. Kozsurek

Extrapyramidal pathways Tectospinal Rubrospinal Reticulospinal Vestibulospinal

Spinal motor pathways Pyramidal tract - control most of our fine movements Tectospinal tract - coordinating head and eye movements as part of the optic reflexes Vestibulospinal tract - influences postural muscles Reticulospinal tract - projects from the reticular formation - inhibition or facilitation of movement Rubrospinal tract -from the red nucleus From : The Central Nervous System, P. Brodal Olivospinal tract? ? - from the inferior olive

TRANSVERSE SECTION SPINAL CORD MOTOR PATHWAYS 35

Role of the motor pathways from the brainstem u Extrapyramidal system: – coordinates movements of various groups of muscles both in space and time, – regulates automatic movements consisting of periodic elements (e. g. walking, running, riding, driving a car, handwriting or typing, etc. ), – controls emotional movements, – helps to control posture and balance, – regulates muscle tone.

Overview of motor pathways

MOVEMENT DISORDERS Neuropathology of Parkinson’s disease • nigro-striatal pathway degeneration • leading to a depletion of striatal dopamine • some degeneration of other dopamine pathways too

Human midbrain Parkinson’s disease Normal
 and striatonigral (GABA) tracts X dopaminergi c GABAergi c")
Nigrostriatal (DA) and striatonigral (GABA) tracts X dopaminergi c GABAergi c

Parkinson’s disease Michael J. Fox Muhammad Ali Pope John Paul II Janet Reno Pathophysiology: Primary: - loss of nigrostriatal DA projection Katherine Hepburn
 u Bradykinesia u Rigidity")
Parkinson’s disease Symptoms Motoric u Tremor (~4 -5 Hz, resting) u Bradykinesia u Rigidity u Loss of postural reflexes Depression Dementia

Huntington’s disease u Pathophysiology – Atrophy of striatum – Loss of striatal GABA-ergic, medium spiny Huntington’s neurons Normal

Parkinson's disease - involves major loss of dopaminergic cells in the substantia nigra; Huntington's disease - involves massive loss of medium spiny neurons in the striatum. The symptoms of the two diseases are virtually opposite: Parkinson's disease is characterized by gradual loss of the ability to initiate movement, whereas Huntington's disease is characterized by an inability to prevent parts of the body from moving unintentionally.

Thank you for your attention!
- Slides: 45