BASAL CELL CARCINOMA Most common skin cancer A

BASAL CELL CARCINOMA Most common skin cancer A locally invasive, slowly spreading, primary epithelial malignancy that arises from the basal cell layer of the skin Chronic exposure to ultraviolet radiation mutations in the patched(PTCH) gene, SMO, P 53
 basal cell carcinoma Rodent ulcer")
Nodular (noduloulcerative) basal cell carcinoma Rodent ulcer

Pigmented basal cell carcinoma
 basal cell carcinoma Superficial basal cell carcinoma")
Sclerosing (morpheaform) basal cell carcinoma Superficial basal cell carcinoma

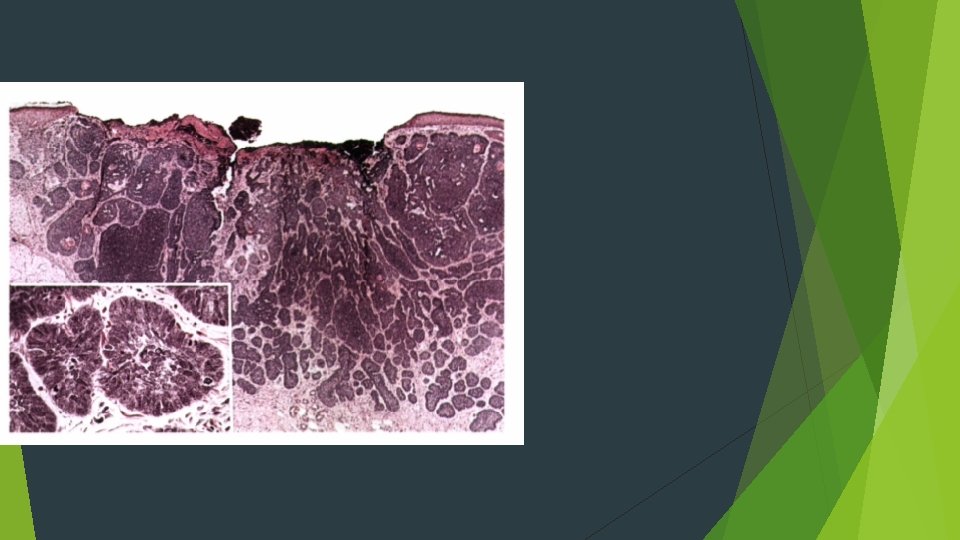
HISTOPATHOLOGIC FEATURES Nests and cords of cuboidal cells arise from the region of the epidermal basal cells Neoplastic cells around the periphery of the invading nests and strands are usually palisaded and often columnar Basosquamous carcinoma

TREATMENT AND PROGNOSIS

Pathologic basics of mucocutaneous lesion
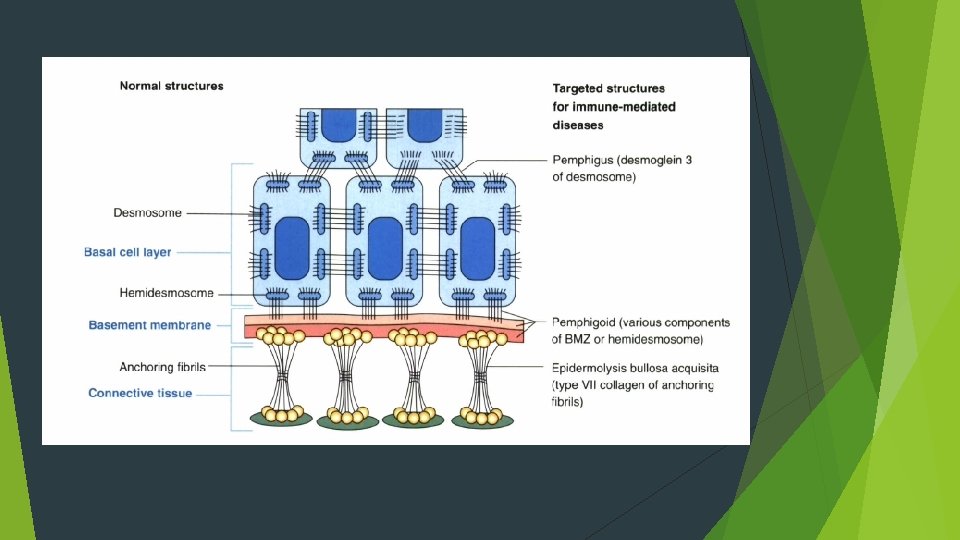

Pemphigus 1. Pemphigus vulgaris 2. Pemphigus vegetans 3. Pemphigus erythematosus 4. Pemphigus foliaceus Autoantibodies that are directed against the epidermal cell surface glycoproteins, desmoglein 3 and desmoglein 1

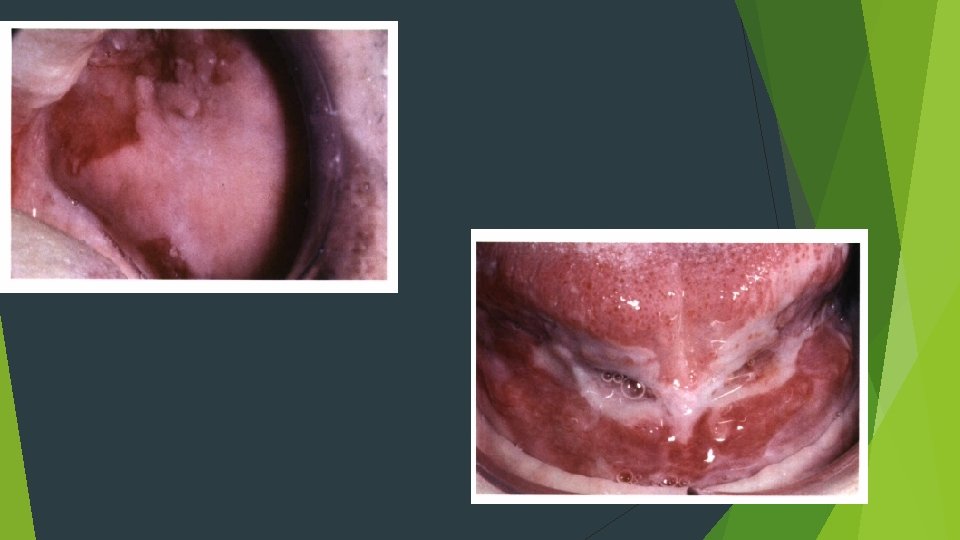
Adults Palate, labial mucosa, buccal mucosa, ventral tongue, and gingiva Rarely report vesicle or bulla formation intraorally Positive Nikolsky sign


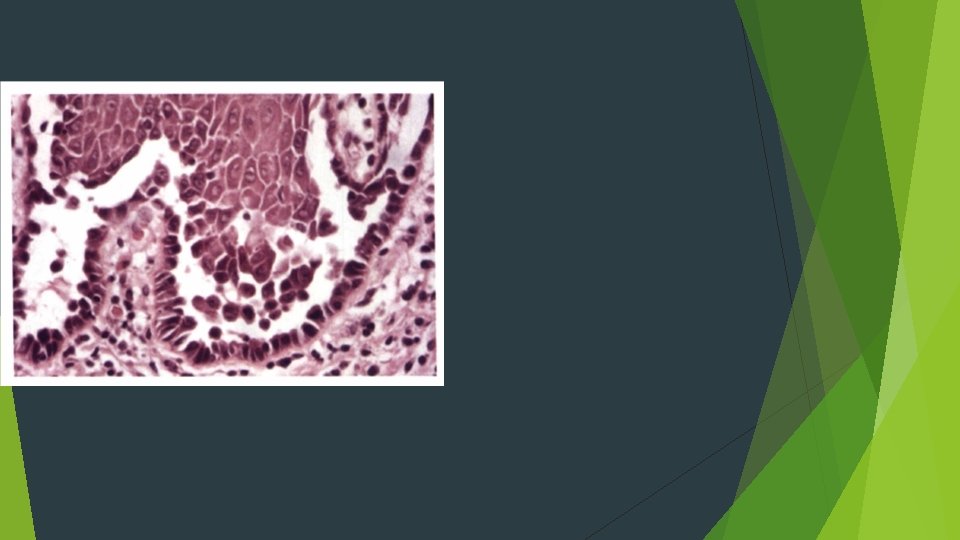
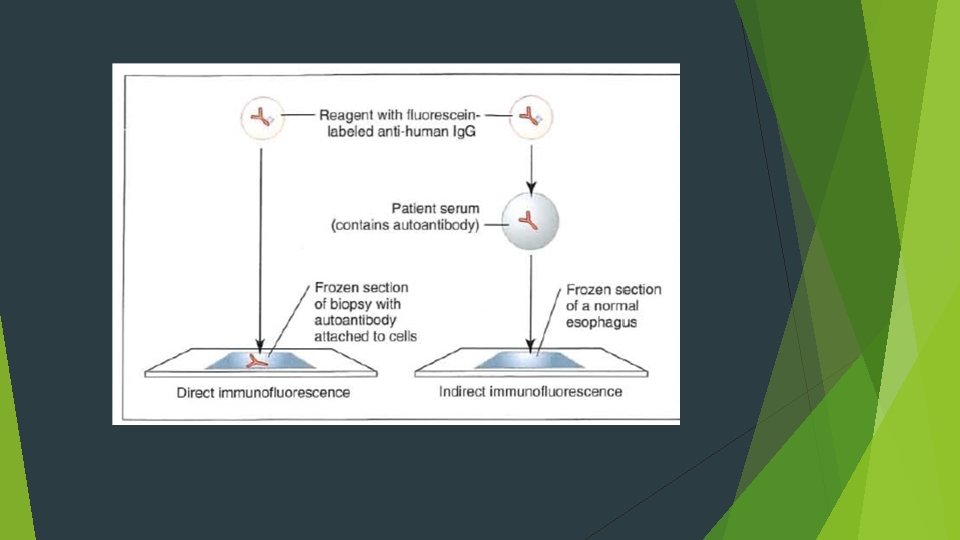
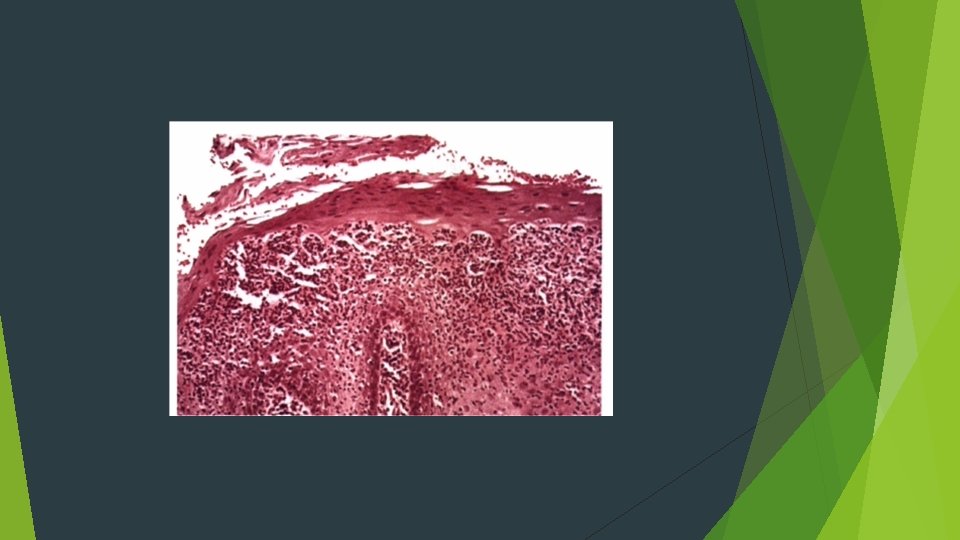
HISTOPATHOLOGIC f. EATURES Characteristic intraepithelial separation, which occurs just above the basal cell layer of the epithelium Row of tombstones Acantholysis Tzanck cells Mild-to-moderate chronic inflammatory cell infiltrate
 and complement components (usually C")
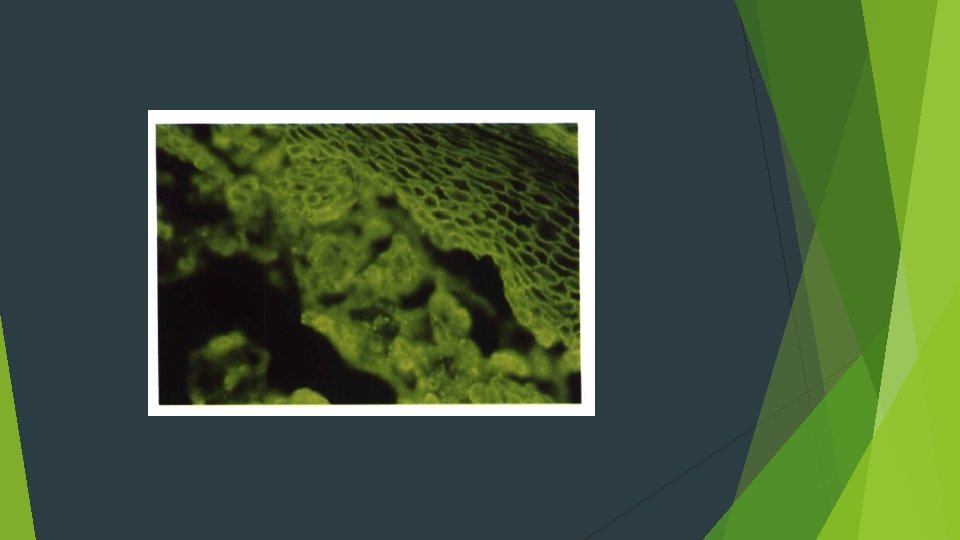
Direct immunofluorescence examination Ig. G or Ig. M) and complement components (usually C 3)

TREATMENT AND PROGNOSIS

Paraneoplastic Pemphigus

Mucous Membrane Pemphigoid Autoantibodies are directed against one or more components of the basement membrane twice as common as pemphigus vulgaris Cicatricial pemphigoid Older adults Females Oral lesions are seen in most patients


Gingival involvement produccs a clinical reaction pattern termed desquamative gingivitis The most significant complication of mucous membrane pemphigoid, however, is ocular involvement



HISTOPATHOLOGIC f. EATURES split between the surface epithelium and the underlying connective tissue in the region of the basement membrane A mild chronic inflammatory cell infiltrate

Direct immunofluorescence studies of perilesional mucosa show a continuous linear band of immunoreactants at the basement membrane zone Ig. G and C 3, although Ig. A and Ig. M

TREATMENT AND PROGNOSIS

ERYTHEMA MULTIFORME A blistering, ulcerative mucocutaneous condition Herpes simplex or Mycoplasma pneumoniae, or exposure to anyone of a variety of drugs and medications, particularly antibiotics or analgesics Minor Major (traditionally thought to be synonymous with Stevens- Johnson syndrome) Toxic epidermal necrolysis (Lyell's disease)

Acute onset young adults in their 20 s or 30 s Men Prodromal symptoms include fever, malaise, headache, cough, and sore throat Target lesions



HISTOPATHOLOG'C FEATURES Subepithelial or intraepithelial vesiculation may be seen in association with necrotic basal keratinocytes A mixed inflammatory infiltrate is present, consisting of lymphocytes, neutrophils, and often eosinophils Perivascular orientation

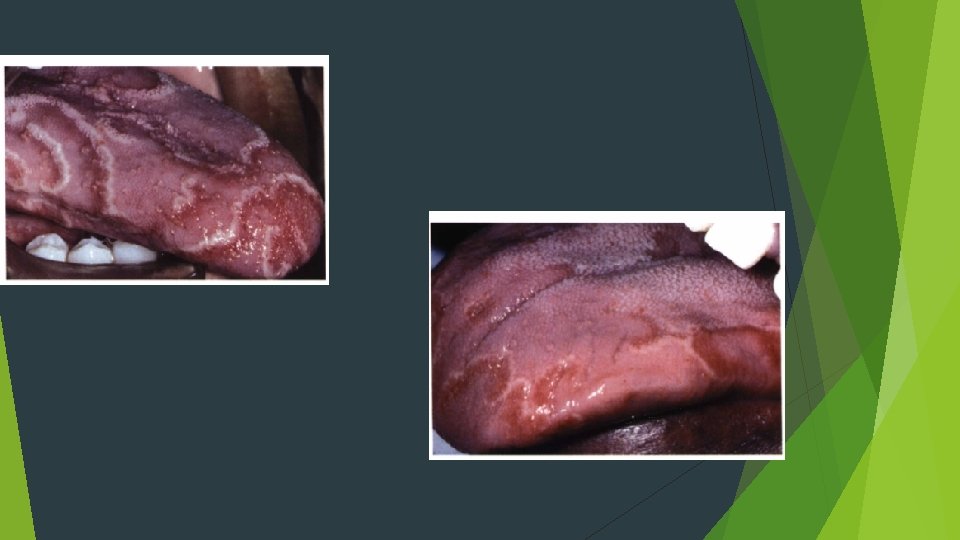
ERYTHEMA MIGRANS GEOGRAPHIC TONGUE common benign condition that primarily affects the tongue Females anterior two thirds of the dorsal tongue mucosa

HISTOPA THOLOGIC FEATURES Hyperparakeratosis, spongiosis, acanthosis, and elongation of the epithelial rete ridges are seen Neutrophils (Munro abscesses) are observed within the epithelium lymphocytes and neutrophils involve the lamina propri a The intense neutrophilic infiltrate may be responsible for the destruction o fthe superficial portion of the epithelium
 Lichenoid foreign body gingivitis hepatitis C infection,")
LICHEN PLANUS Lichenoid mucositis (or lichenoid dermatitis) Lichenoid foreign body gingivitis hepatitis C infection, stress or anxiety middle-aged adults Women Reticular, erosive

RETICULAR LICHEN PLANUS Wickham's striae lateral and dorsal tongue, the gingivae, the palate, and vermilion border


EROSIVE LICHEN PLANUS


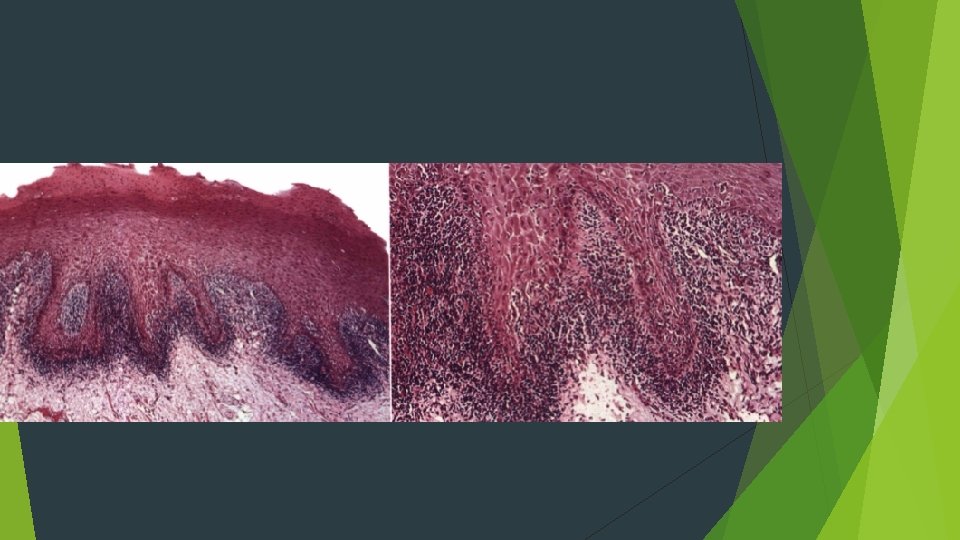
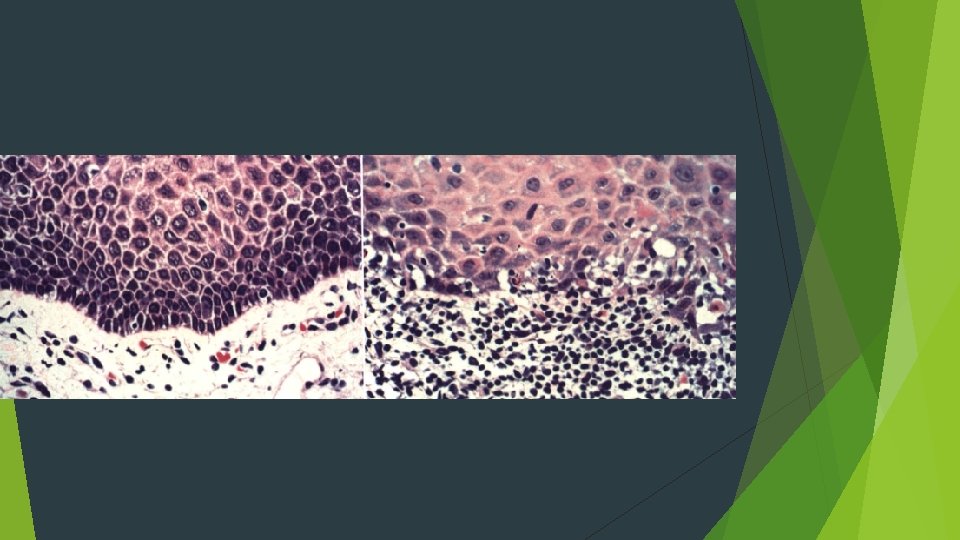
HISTOPATHOLOGIC FEATURES Orthokeratosis and parakeratosis may be present on the surface of the epithelium "saw-toothed" shape Hydropic degeneration bandlike infiltrate of predominantly T lymphocytes immediately subjacent to the epithelium Colloid, cytoid, hyaline, or Civatte bodies

TREATMENT AND PROGNOSIS
 An acute and chronic inflammatory autoimmune disease No known cause")
Systemic Lupus Erythematosus (SLE) An acute and chronic inflammatory autoimmune disease No known cause Affects women 8 times more frequently than men, predominantly during childbearing years Three times more frequent in black women than in white women
 (cont. ) A syndrome with a wide range of disease")
Systemic Lupus Erythematosus (SLE) (cont. ) A syndrome with a wide range of disease activity Usually chronic and progressive Periods of remission and exacerbation Autoantibodies to DNA are present in serum May have a genetic component
 Skin lesions occur in 85% of individuals")
Clinical Features of Systemic Lupus Erythematosus (SLE) Skin lesions occur in 85% of individuals “Butterfly” rash on bridge of nose May be erythematous lesions on fingertips Arthritis and arthralgia are common Oral lesions accompany skin lesions in about 25% of patients with discoid LE Erythematous plaques or erosions May have white striae; resemble lichen planus but are less symmetric
 (cont. )")
Clinical Features of Systemic Lupus Erythematosus (SLE) (cont. )
 (pgs. 101 -102) Usually based on multiorgan involvement")
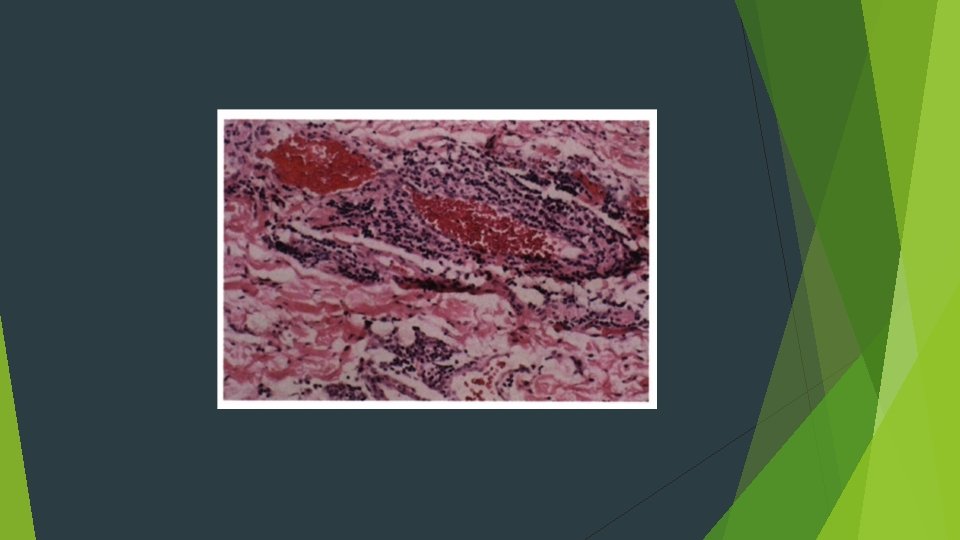
Diagnosis of Systemic Lupus Erythematosus (SLE) (pgs. 101 -102) Usually based on multiorgan involvement and presence of antinuclear antibodies in serum Inflammatory infiltrate is around blood vessels in connective tissue.
 Aspirin and antiinflammatory drugs for mild")
Treatment and Prognosis of Systemic Lupus Erythematosus (SLE) Aspirin and antiinflammatory drugs for mild signs and symptoms Hydroxychloroquine and corticosteroids along with immunosuppressive agents may be used

Aphthous Ulcers Painful oral ulcers with an unclear cause Occur in about 20% of the population Trauma is the most common precipitating factor. May be caused by emotional stress or certain food May be associated with certain systemic diseases Thought to have an immunologic pathogenesis Occur in three forms: minor, major, and herpetiform

Minor Aphthous Ulcers Discrete, round or oval ulcers Occur on movable mucosa Up to 1 cm in diameter with a erythematous halo surrounding a yellowish-white fibrin surface May have single or multiple lesions May have a prodrome of 1 to 2 days
")
Minor Aphthous Ulcers (cont. )
, deeper, and longer lasting than minor aphthous ulcers")
Major Aphthous Ulcers Larger (>1 cm), deeper, and longer lasting than minor aphthous ulcers Very painful Occur in the posterior of the mouth more often than minor aphthous ulcers May require several weeks to heal May require a biopsy
")
Major Aphthous Ulcers (cont. )
 Resemble herpes simplex ulcers Painful, generally")
Herpetiform Aphthous Ulcers Tiny (1 to 2 mm) Resemble herpes simplex ulcers Painful, generally occur in groups
")
Diagnosis of Minor Aphthous Ulcers (Cont. )
 Clinical appearance Location Herpetic lesions appear on")
Diagnosis of Minor Aphthous Ulcers (Cont. ) Clinical appearance Location Herpetic lesions appear on mucosa fixed to bone, aphthous lesions appear on movable tissue Clinical history Aphthous ulcers do not produce systemic signs or symptoms as do herpetic lesions

Treatment of Minor Aphthous Ulcers Treatment There are several OTC medications such as Orabase and Zilactin. Topical or systemic steroids may help. Topical anesthetic may help.
- Slides: 63