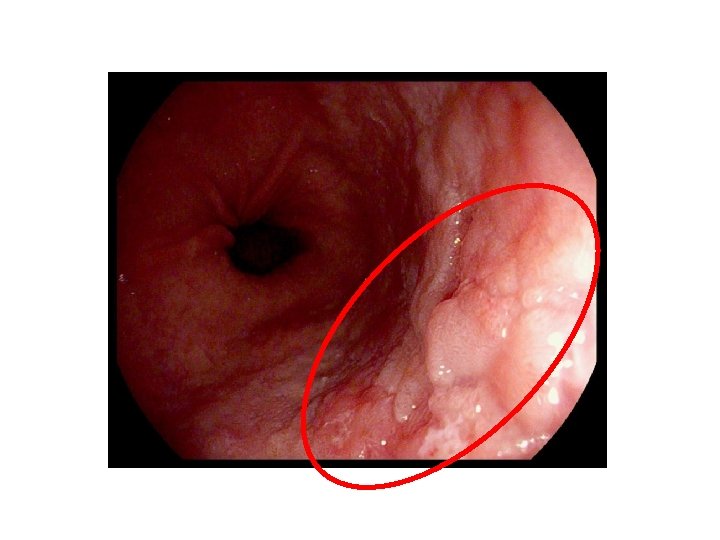
Barretts Esophagus Does that Zline look irregular to

Barrett’s Esophagus: Does that Z-line look irregular to you? Andrew Flynn, MD, Ph. D, FRCPC Sept 22, 2017

Disclosures • None relevant.

Acknowledgments • Dr. Cheryl Wright, PATH

Table of Contents • • Epidemiology Screening/diagnosis Surveillance/management Quiz!

But first. . . the case • 50 y. o. man referred for Barrett‘s screening. • 8 year history of heartburn, well controlled with daily pantoprazole. • No dysphagia or other alarm symptoms. • Otherwise healthy. Smokes occasional cigar. Social Et. OH. • Father and paternal aunt with esophageal adenocarcinoma.

Endoscopy

Barrett’s History • Norman Barrett, 1950 • “. . . in cases of congenital short oesophagus. . . the bare area is larger than usual. ”

Definition • Metaplasia from normal stratified squamous epithelium to columnar epithelium with goblet cells (“intestinal metaplasia”). • May or may not be associated with dysplasia.

http: //medcell. med. yale. edu/systems_cell_biology/gi_tract_lab. php

Pathogenesis? Souza et al. , 2008

Epidemiology • Prevalence = 1. 5% in general population, 15% in those with GERD • RFs = older age, male, smoking, obesity, white ethnicity, FHx

So what s the problem 0. 25% ~0. 55% 4 -8% Conteduca et al. , 2012

Could be worse! 17. 5% 10 year risk of EAC 2. 5% Wani et al. , 2011

Adeno vs squamous • “Lower third” • Barrett’s, GERD, smoking, obesity • Incidence rising • “Upper two thirds” • Smoking, Et. OH, dietary factors, caustic ingestion • Incidence falling

Screening • Points to keep in mind: 1. > 90% of patients with EAC have never been diagnosed with BE 2. 40% of patients with BE do not have a clinical history of GERD 3. The majority of patients with BE will not die of EAC Sikkema et al. , 2010

Screening guidelines • Consider screening patients with > 5 yrs heartburn or acid regurgitation, and 2 of: – Age > 50 yrs – Caucasian race – Central obesity – Smoking history – History BE/EAC in first degree relative • ACG Guideline 2015 – Strong recommendation, moderate (male) or low (female) level of evidence.

Diagnosis • Columnar epithelium ≥ 1 cm above GEJ + biopsy demonstrating intestinal metaplasia. • 4 quadrant biopsies every 2 cm • > 3 cm = long segment Harrison et al. , 2007
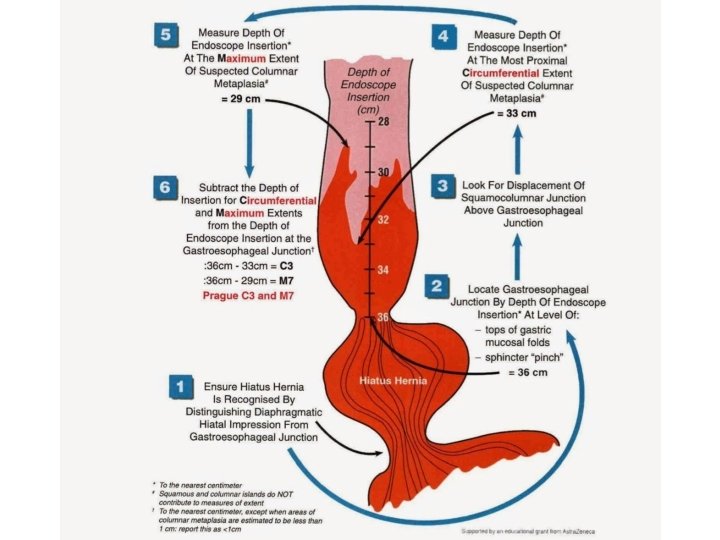

Prague Classification • C 1 M 4 Schoofs et al. , 2017

8 weeks PPI bid

Imaging modalities • Current recommendation: – High-definition white light endoscopy • Goal: – Imaging modality to improve targeted biopsies VLE HD-WLE NBI Chromo CLE Eluri and Shaheen, 2017 Leggett et al. , 2016

Adherence to screening Abrams et al. , 2009

Alternative screening options

Transnasal endoscopy

Cytosponge

Surveillance/Management
 pathologist vs Eluri and Shaheen, 2017")
Confirmed by 2 nd (expert) pathologist vs Eluri and Shaheen, 2017

Radiofrequency ablation Eluri and Shaheen, 2017

RFA results Shaheen et al. , 2009

Recurrence post RFA Pasricha et al. , 2014

Death post RFA EAC Wolf et al. , 2015

RFA for LGD? Phoa et al. , 2014
 ? Esophagectomy Shaheen et al. , 2015")
Surveillance/Management (submucosal invasion) ? Esophagectomy Shaheen et al. , 2015

EMR Sakai and Maluf. Filho, 2015

“Chemoprevention”? No PPI Kastelein et al. , 2013
 is common in older males with GERD •")
Summary • Barrett’s esophagus (intestinal metaplasia) is common in older males with GERD • Screening involves EGD with 4 quadrant biopsies every 2 cm • Dysplasia is a significant risk factor for EAC • RFA +/- EMR is effective at eradicating Barrett’s with/without dysplasia • PPI therapy is recommended for Barrett’s

Back to the case

Quiz time!

Yes!
")
No! (Eo. E)

No!

No!

Yes!
")
No! (sloughing)

No!

Yes!
")
Yes/No (EAC)

What we’re trying to avoid
- Slides: 49