Bariatric Surgery in the Waikato The 360 o

Bariatric Surgery in the Waikato: The 360 o View J Wu*, D Schroeder, ** B Gibbison, * J Mc. Clymont* Waikato Adult Weight Management Programme* Surgical Obesity Service**


Roux-en Y Gastric Bypass Surgery l Restrictive: – l 15 ml gastric pouch Malabsorptive – Bypass to ~50 cm distal to DJ flexure
 31% men: 69% women")
Quantity & Demographics l l l 45 patients (2005 -2009) 31% men: 69% women Age: 25 -64 y/o (48+/-10) BMI: 44 +/-6. Ethnicity: NZ Europ. 60. 0% NZ Maori 31. 1% Pacific Is. 6. 7% Unspecified 2. 2%

Obesity Related Disorders l Diabetes: 90% – – – l l l Diet: 4% Orals: 30% Insulin: 66% IGT: 7% OSA: 40% HTN: 93%

Patient Tracking post Surgery l l Weight Loss Health Benefits Quality of Life (SF 36) (2007 onwards) Complications
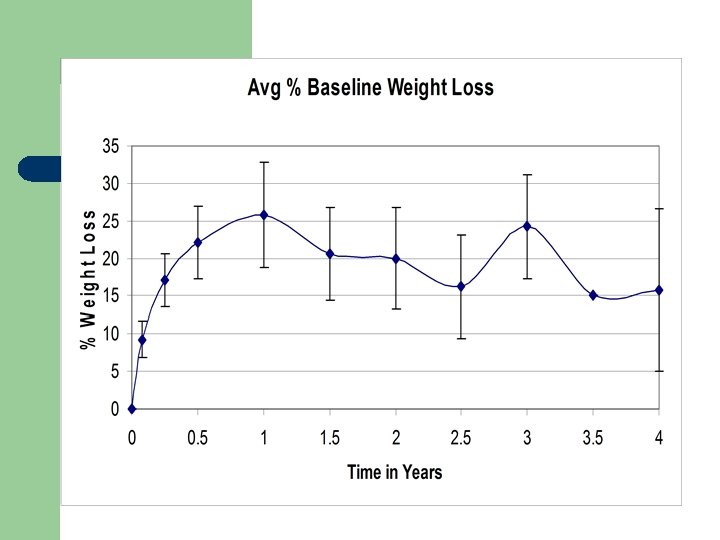

Weight Loss l l l Peaks at 1 yr at ~25% of Baseline Weight Loss Trend to regain some weight long term. At > 2 Y post surgery: % Base. Wt. <10% >10 - <20 >20 - <30 >30 % of Patients 13 60 20 7

Good Losers vs Poor Loosers: What’s the difference? l Formally compared weight loss between: – – – Ethnic groups +/- previous AWMP participation Male vs. Female Age groups Baseline Quality of Life Measurements (SF 36)

What’s the difference? l Formally compared weight loss between: – – – Ethnic groups - none +/- previous AWMP participation Male vs. Female Age groups Baseline Quality of Life Measurements (SF 36)

What’s the difference? l Formally compared weight loss between: – – – Ethnic groups - none +/- previous AWMP participation - none Male vs. Female Age groups Baseline Quality of Life Measurements (SF 36)

What’s the difference? l Formally compared weight loss between: – – – Ethnic groups - none +/- previous AWMP participation - none Male vs. Female - none Age groups Baseline Quality of Life Measurements (SF 36)

What’s the difference? l Formally compared weight loss between: – – – Ethnic groups - none +/- previous AWMP participation - none Male vs. Female - none Age groups - Yes Baseline Quality of Life Measurements (SF 36)


What’s the difference? l Formally compared weight loss between: – – – Ethnic groups - none +/- previous AWMP participation - none Male vs. Female - none Age groups - Yes Baseline Quality of Life Measurements (SF 36) - Yes

Physical Function & Bodily Pain Scores: Negative Correlation with Future Wt Loss? l l r = - 0. 68 (rsq=0. 47) Increased physical limitations & bodily pain may predict better future weight loss.

Role Limitation due to Emotional & General Mental Health Sum of Scores: Positive Correlation with Future Wt Loss? l r = 0. 52 (rsq = 0. 27) l Suggests that poor mental health may carry a risk of poor future weight loss.

Additional Observations l l Patient who tend to lose weight well in the first year, tend to do better long term. Patients selected early in the programme tended to achieve less overall weight loss than those selected later in the programme. – Formally compare weight loss at 1 Y for patients who received surgery from 2005 -7 with those who received surgery in 2008.
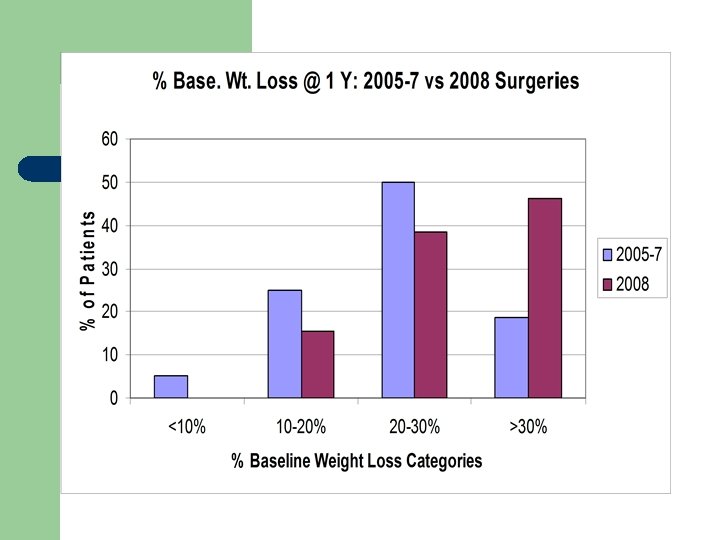

2008 vs 2005 -2007 Surgeries l l Age: No difference SF 36 QOL: – – l l Physical Function Score: 65 (2005 -2007 group) vs 28 (2008 group): p=0. 0004 Addition of Behavioural Therapist at the end of 2007 @ the Surgical Obesity Service. Better selection of patient?
 – –")
Health Improvements: Diabetes l Cure rate (as assessed by HBA 1 c) – – – Diet alone: 100% Oral Rx: 73% (88%: able to D/C meds) Insulin: 0% l l l 60%: able to D/C insulin and onto orals or diet 40%: decrease insulin usage by 62% Improvement in HBA 1 c of those not cured: – 8. 9+/-2. 3% to 7. 4+/-1. 5% (p=0. 02)

Health Improvements: l OSA: – l Hypertension – – l 26% D/C meds 139/79 to 126/71: p=0. 0003 Urine Microalbumin: Cr – l 41% were able to discontinue CPAP machine. 46% had normalisation of ratio CRP – 9. 8 to 2. 8 mg/L: p=0. 015

Health Improvements: Lipids Total HDLC LDL-C C Tg Baseline 4. 43 2. 56 1. 16 2. 09 > 1 Y Post. Surgery 4. 34 2. 47 1. 26 1. 33 0. 05 0. 000 3 p value 0. 68 0. 6

SF 36 QOL Improvements
 OGD")
Surgical Complications l l No mortalities Post-operative infections: 6% Abdominal surgery: 4% (adhesions) OGD for symptoms of obstruction: 16% – 29% of OGD were normal-no cause found

Nutritional Deficiencies l Routine supplementation: – – l All: MVI Women: Ca & Fe/Folate No detectable deficiencies – < 16% Nutrient % of Patients Vitamin B 12 52 Vitamin D 29 Iron 16 Protein 16 Vitamin E 2

Other Complications l l Post-operative gout attack: 7% Renal Nephrolithiasis: 4% Bilateral Peripheral Neuropathy: 2% Psychological: 16% – – DSM Psychological Disorders with MH involvement: 44% Referral to psychologist privately: 56%

Roux en Y Gastric Bypass Surgery: Weight Loss l l ~13% fail to lose weight effectively (~20% in literaturef) Tendency to regain some weight at 2 Y. fj – – – Younger adults do better Increased perceived bodily pain & poor physical function prior to surgery – may do better. Decreased mental health affecting function – may do worse. * FSugerman et al. , Am. J. Surg. 1989. 157: 93; Brolin et al. , Surgery. 1989. 105: 337. j. Maclean et al. , Am. J. Surg. 1993: 165: 155. *Herpertz et al. , Obesity Res. 2004. 12: 1554.

Roux en Y Gastric Bypass Surgery: Health Benefits l l l Diabetes OSA Hypertension Lipids Markers of CV risk Quality of Life

Roux en Y Gastric Bypass Surgery: Complications l Category % of Patients Surgical 26 Nutritional 84 Psychological 16 Other 13 Of the patients who continue to f/u with > 1 Y data, 12% have had no complications to date.

Roux en Y Gastric Bypass Surgery: Conclusions l l l Care with patient selection Care with patient preparation for best results & expectations Continued monitoring for complications – – – Surgical Nutritional Psychological

Acknowledgements l Waikato Diabetes Service – – l Peter Dunn Susie Ryan Adult Weight Management Programme – Sharon Moore l Surgical Obesity Service – – – Carol Stidolph Andrea Schroeder Ann Monahan Donna Southwick Zola Mc. Donald
- Slides: 33