BAMBOO SPINE Diagnosis Ankylosing Spondylitis Discussion Anterior and


BAMBOO SPINE

Diagnosis: Ankylosing Spondylitis Discussion: Anterior and lateral radiograph of the lumbar spine which reveals near complete fusion of all of the vertebral bodies. Spinal changes which include squaring of the vertebral bodies and fusion between adjacent levels. The fusion is secondary to syndesmophytes and resembles a bamboo stalk. This is most commonly found in ankylosing spondylitis
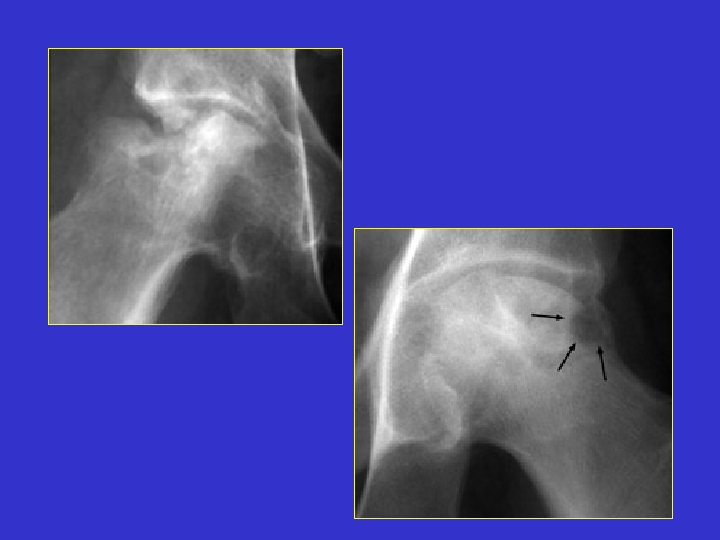

Bite Sign

Diagnosis: Avascular Necrosis Discussion: One image each of two separate patients with collapse and necrosis of the femoral head, both of which are secondary to repeated injection of steroids. A rapid progression of change in a joint secondary to steroid injections. Transition of a joint from one of minor alterations(such as narrowing, sclerosis) to one of significant bony fragmentation and collapse. Gougedout areas of bony destruction may be similar to small animal bites, hence the bite sign.


Blade of Grass Sign

Diagnosis: Paget's Disease Discussion: Paget's disease has three distinct phases visible radiographically: a lytic phase, a sclerotic phase, and a mixed lytic-sclerotic phase. When involvement of the lytic phase is present in a long bone, the lytic changes may advance as a V- or wedge-shaped radiolucent area, clearly demarcated from the adjacent bone. This has been likened to a blade of grass.
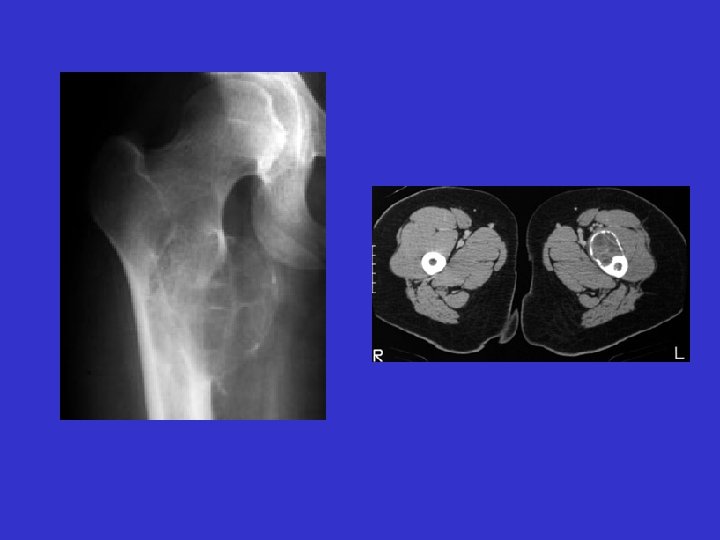

Blister of bone

Diagnosis: Aneurysmal bone cyst Discussion: Frontal radiograph of the right hip and CT scan of the hips on a different patient. Both reveal a cystic bubbly lesion with fine internal septations. Additionally, compromise of the cortical margin of the lesion is present as well. The "blister of bone" sign refers to a bubbly cystic lesion with a saccular protrusion of the cortex with multiple fine internal septae. The shell of the lesion may fracture resulting in extravasation of blood into the adjacent tissues. This sign is highly characteristic of aneurysmal bone cyst.
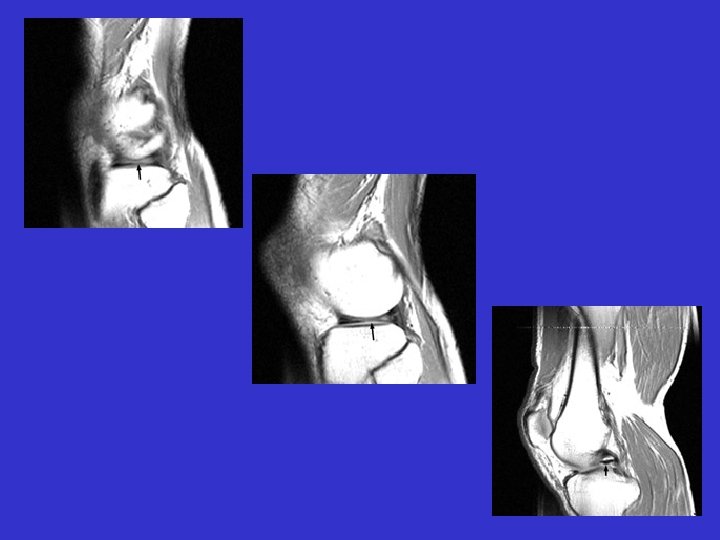

Bucket-handle tear of the menisci

Absent bow tie sign Multiple sagittal T 1 weighted images which reveal loss of the normal bow-tie appearance of the meniscus. The "absent bow tie sign" is another good sign of a bucket handle tear of the meniscus. The absence of the normal bow-tie is secondary to the displaced fragment which makes up the "handle" of the bucket. Requirement for the absent bow tie sign mandates that the normal requirement of at least two adjacent sagittal images with a normal meniscal body segment appearance is not present.
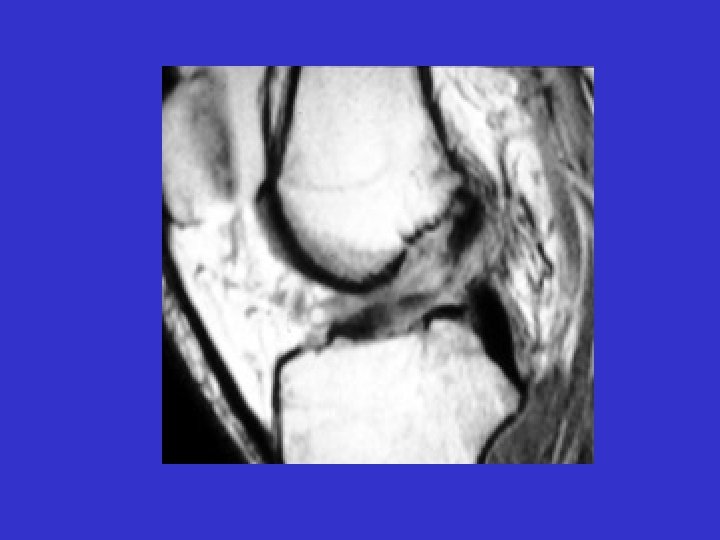
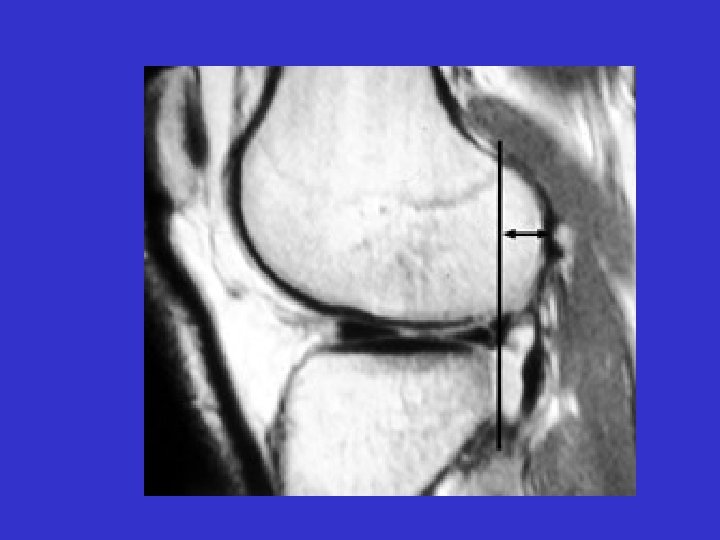

Anterior Drawer Sign ACL Tear The anterior cruciate ligament runs obliquely within the lateral aspect of the intercondylar notch, attaching to the inner aspect of the lateral femoral condyle proximally and to the anterior aspect of the intercondylar eminence of the tibia distally. An anterior cruciate ligament-deficient knee allows the tibia to undergo subluxation anteriorly relative to the femur. This is the MR equivalent of the anterior drawer sign.


A bone-in-bone sign

Diagnosis: Osteopetrosis Discussion: Single lateral lumbar spinal x-ray revealing increased sclerosis in the superior and inferior portions of the midbody of the vertebra. This is seen in vertebrae that have a small replica of the vertebral body inside the normal one, giving a bone-in-bone sign. It is produced by failure of osteoclastic activity causing abnormally dense bone that occurs intermittently producing zones of abnormal density alternating with relatively more normal bone. This is a characteristic finding seen in osteopetrosis.
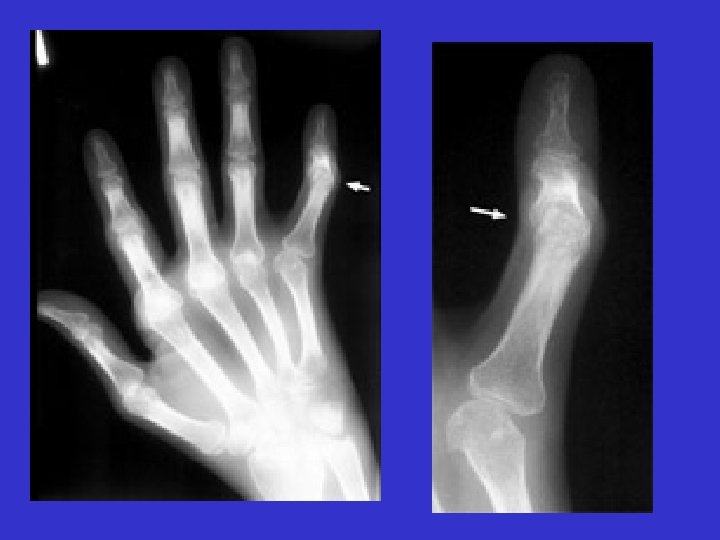

Boutonniere deformity

Diagnosis: Rheumatoid arthritis Discussion: Among the many osseous abnormalities that may be seen in Rheumatoid Arthritis, the boutonniere deformity is the culmination of multiple abnormalities in the hand. Specifically, the deformity arises from hyperextension of the distal interphalangeal joint, while the proximal interphalangeal joint is flexed.
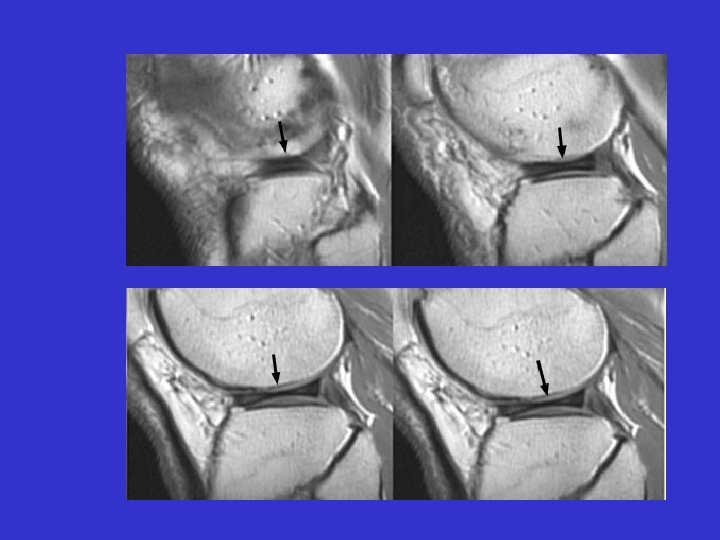

Bow-tie sign

Diagnosis: Discoid Meniscus Discussion: Seen on sagittal images, the bow-tie represents the continuity of the meniscus between the anterior and posterior horns. It is normally seen on 2 contiguous sagittal images. When it is seen on 3 or more contiguous 5 mm thick sagittal images is indicative of a discoid meniscus.
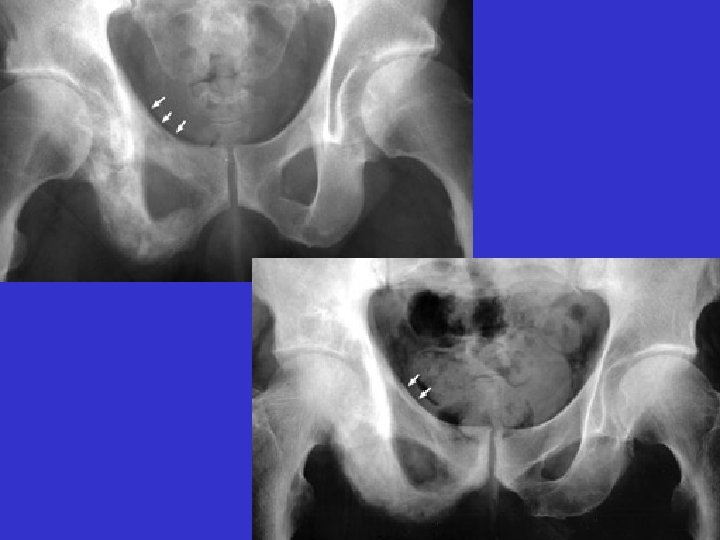

Brim sign

Diagnosis: Paget's Disease Discussion: AP radiographs of the pelvis with changes characteristic of Paget's disease throughout the right hemipelvis. Notice thickening of the right pelvic brim (ileopectineal line) as compared to the left. Thickening of the pelvic brim, or arcuate line (ileopectineal line) seen in patients with Paget's disease. The ridge of bone around the pelvic brim, when osteoblastic reaction occurs, adds to the normal sclerotic density of this area. This is a useful sign in distinguishing Paget's changes from metastatic disease.
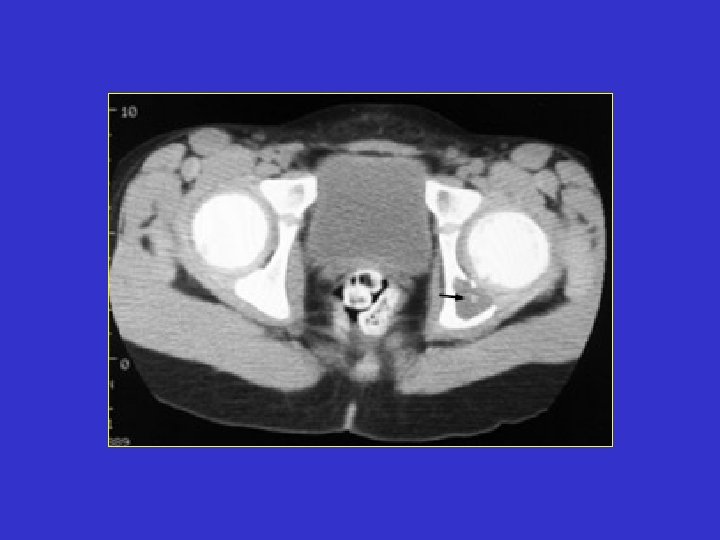

Button sequestrum

Diagnosis: Eosinophilic granuloma Discussion: Single slice of a CT scan of the pelvis with an abnormal lucent area with a sclerotic focus within it in the left hemipelvis. This sign was originally utilized to describe an unusual radiographic manifestation of Eosinophilic Granuloma. It is a round, lucent defect with a bony density, or sequestrum, in its center. This is not pathognomonic as other disease entities such as osteomyelitis can have a similar appearance.


Cockade image

Diagnosis: Intraosseous lipoma Discussion: A classic appearance of intraosseous lipoma of the calcaneus is the presence of a well defined lytic lesion with a central calcification resembling a cockade. A cockade is badge, usually in the form of a rosette, or knot, and generally worn upon the hat.
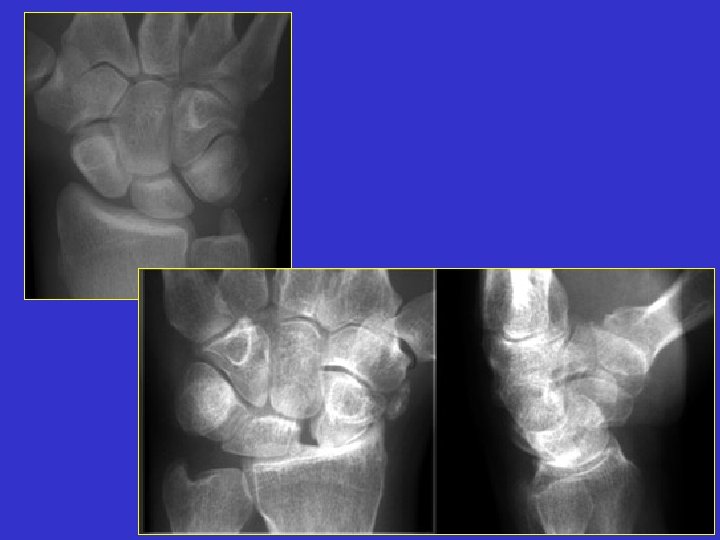

Cortical ring sign

Diagnosis: Rotary subluxation Discussion: Multiple images of navicular disorientation with dislocation of the scapholunate joint. The scaphoid bone, seen along it long axis, has a ringed cortex appearance. This cortical ring sign is a sign of scapholunate dislocation, This sign was first described in 1970 in young patient with bilateral dislocation of the carpal naviculars. This sign (also known as the signet-ring sign) is caused by the abnormal orientation of the scaphoid.
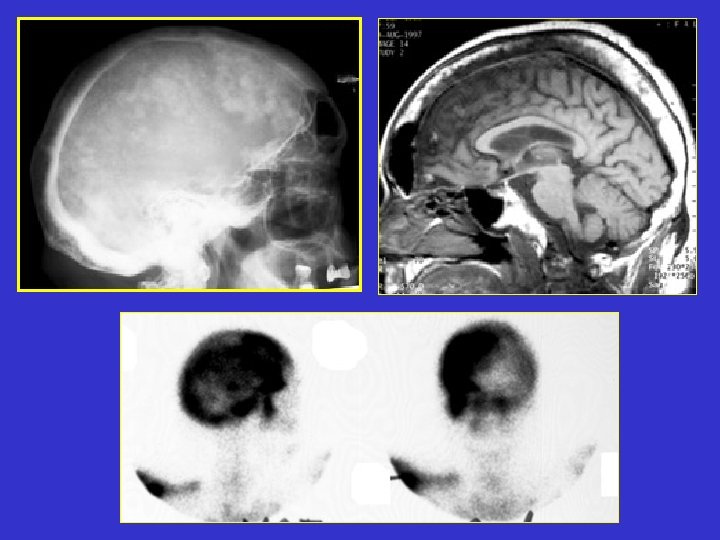

Cotton-wool sign

Diagnosis: Paget's Disease Discussion: Plain film of the skull reveals a large mottled area of radiolucency with small areas of increased density within it. The MR image of the skull reveals a thickened, enlarged cranium with increase in the marrow space. Two bone scan images also reveal increased activity in the skull, more localized to one side, characteristic to the localized disease seen in Paget's. This is classic cranial involvement of Paget's. In the cranium, bone sclerosis may produce circular radiodense lesions in one area, whereas osteoporosis circumscripta is noted elsewhere. In the skull, the common region of involvement is the cranial vault. The osteolytic phase is called osteoporosis circumscripta and appears as multiple geographic, well-demarcated regions of bone resorption that may be mistaken for metastases. Focal radiodensities occur as pagetoid bone is formed. In the quiescent phase, there is a radiodense cotton-wool appearance with a thickened vault.
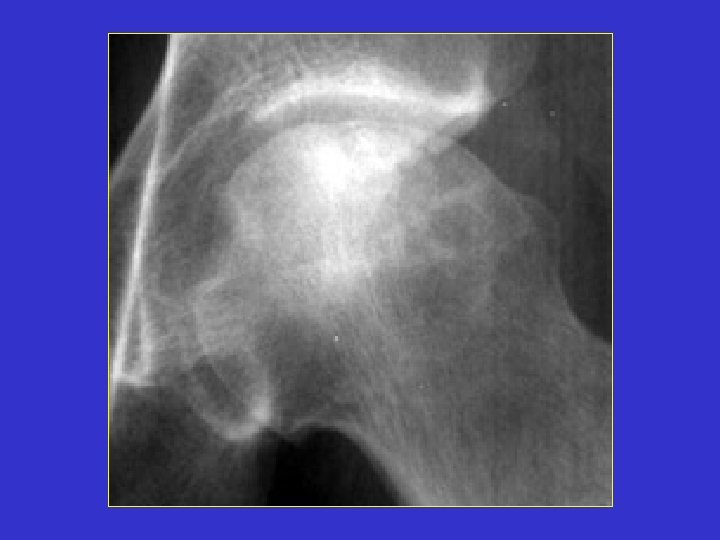

Crescent sign

Diagnosis: Avascular Necrosis Discussion: A radiograph of a left hip joint, which reveal a thin, curvilinear lucent line parallel to the cortical margin of the femoral head. Interruption of the blood supply to the femoral head leads to ischemic necrosis of the marrow and bone that it supplies. Eventually, the bone infarcts and insufficiency fractures may ensue. Fractures that occur in the subchondral bone may be recognized by a crescentic lucent zone that separates the fragment from the remainder of the femur.


Fallen Fragment Sign

Diagnosis: Unicameral bone cyst Discussion: Two radiographs of a pathologic fracture in a simple bone cyst of the proximal humerus. Within the cyst is noted a small, thin, linear bony fragment which is displaced from the site of the fracture. An excellent sign of unicameral bone cyst. The fallen fragment secondary to pathologic fracture is pathognomonic for this cyst. A portion of the wall of the cyst has undergone a pathological fracture and subsequently floated down (fallen) via gravity into the dependent portion of the cyst.

Lincoln Log Sign, or H-shaped vertebra.

Diagnosis: Sickle cell anemia Discussion: Lateral radiographs of the spine reveals central endplate depression with sparing of the anterior and posterior margins of the endplate. Several current names have been ascribed to these same changes seen in patients with hemoglobinopathy, such as Lincoln Log Sign, or H-shaped vertebra. Although not pathognomonic, these terms are typically reserved for a patient with Sickle-Cell disease.
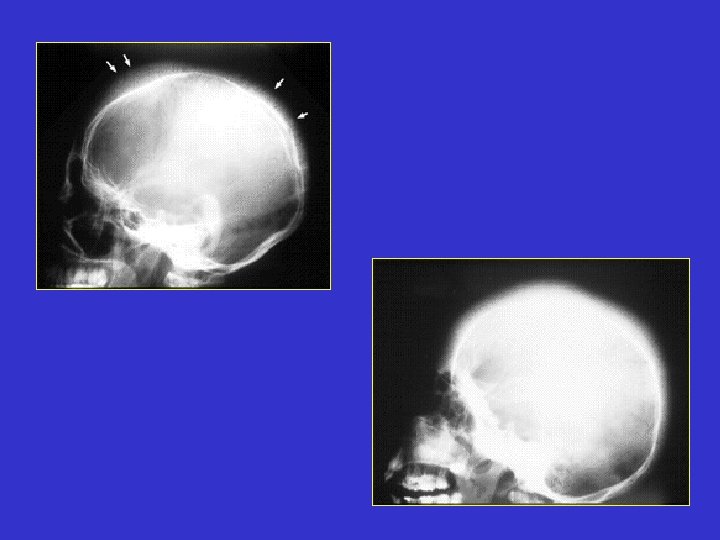

Hair On End

Diagnosis: Hemolytic anemia Discussion: Two lateral skull x-rays with peculiar thin, fine linear extensions radiating out from the skull, appearing as hair standing 'on-end' from the skull. The ‘hair’ represents the accentuated trabeculae extending between the inner and outer skull tables in the expanded diploic marrow spaces. It appears to be ‘on end’ because the trabeculae are oriented perpendicular to the inner and outer tables of the skull. The term is now classically associated with the radiographic changes seen in hemolitic anemia. A. Sickle cell disease. B. Thalassemia.
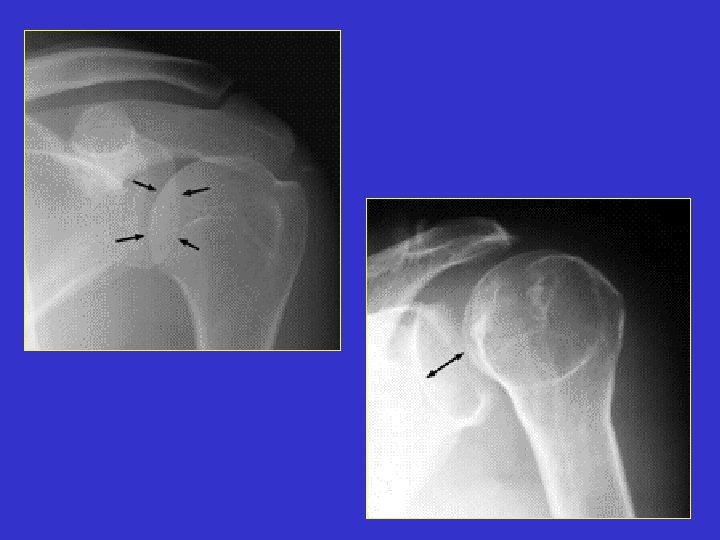

The half moon sign
")
Diagnosis: Absent in posterior dislocation of the shoulder Discussion: Normal left shoulder x-ray (A) and second abnormal left shoulder x-ray (B) with posterior dislocation; notice the lack of overlap of the humeral head with the glenoid. Normally the medial part of the head of the humerus overlaps the glenoid fossa to form a shadow shaped like a half-moon which reaches down to the inferior border of the fossa. This disappears in posterior dislocation.


Heel pad sign

Diagnosis: Acromegaly Discussion: Single lateral radiograph of the foot with a grossly enlarged and thickened calcaneal heel pad. Although not pathognomonic, a heel pad thickness greater than 23 mm may indicate acromegaly. The overabundance of growth hormone in acromegaly causes, among other things, gradual enlargement of hands, feet, and exaggeration of facial features. Not limited to the bones, however, enlargement of other parts of the body, such as the soft tissues of the heel may help to diagnose acromegaly.


Hill sach’s sign

Diagnosis: s/p anterior shoulder dislocation Discussion: Frontal film of the right shoulder which reveals a defect of the posterolateral aspect of the humeral head, consistent with a Hill -Sachs deformity. The Hill-Sachs sign represents deformity of the superior, posterior border of the humeral head and is typically a result of impaction of the anterior inferior surface of the glenoid labrum on the posterolateral aspect of the humeral head during dislocation.
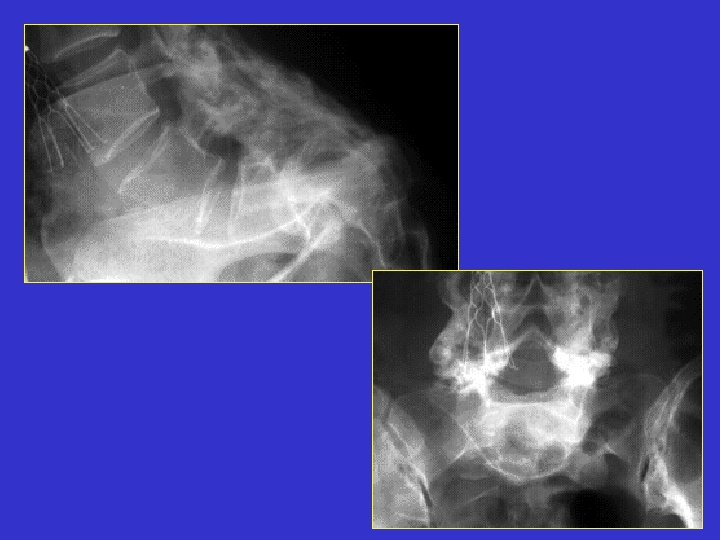

Inverted napoleon hat sign

Diagnosis: Spondylolisthesis Discussion: Frontal and lateral radiographs of the lumbar spine revealing anterolisthesis of the L 5 vertebral body with the typical inverted Napoleon Hat sign. This sign is reserved for spondylolisthesis of the L 5 vertebral body. With a case of spondylolisthesis, the AP radiograph will reveal the anterior border of the transverse process in continuity with the anterior border of the body of the same vertebrae. This continuous anterior border of the L 5 vertebrae will be projected against the shadow of the sacrum, and appear as an upside-down (or inverted) Napoleon hat.


Ivory vertebrae Sign

Diagnosis: Mets, Paget, Lymphoma Discussion: A uniformly white vertebra with no abnormality of its contour or adjacent disks. The vertebra stands out against the adjacent normal, or darker, vertebral bodies. While the list of possible etiologies of ivory vertebrae is extensive, the most common causes of ivory vertebrae are typically metastatic disease, and Paget’s. A-B. Metastatic breast cancer. C-D. Paget's disease







- Slides: 76