BALANCED OCCLUSION Contents Introduction Definition Difference between natural

BALANCED OCCLUSION

Contents Introduction Definition Difference between natural and artificial occlusion Sear’s axioms Ideal requirements Types of complete denture occlusion Balanced occlusion Requirements Controversies General considerations/ principles Advantages Disadvantages

Various concepts proposed to attain balanced occlusion Factors influencing balanced occlusion Arrangement of teeth in balanced occlusion Summary Conclusion

Introduction Occlusion in CD has been a concern since ancient times when attempts were made to replace lost teeth. Teeth carved from ivory and fastened to gold plates have been found in mummies dating back to more than 2500 years Edward angle made the first description of the occlusion relationship of the teeth in 1809. Then occlusion became a topic of much interest and discussion

There are a number of prominent factors in the making of dentures of which one is occlusion Today there are numerous techniques, concepts and philosophies regarding CD occlusion

Definitions Occlusion: “The act or process of closure or being closed or shut off” The static relationship between the incising or masticating surfaces of the maxillary or mandibular teeth or tooth analogues (GPT 8)

“The bilateral, simultaneous, anterior and posterior occlusal contact of teeth in centric and eccentric positions “(GPT 8) “Occlusal contacts of maxillary and mandibular teeth initially in maximum intercuspation and their continuous contacts during movements from this position along specific working, balancing and protrusive guidance pathways developed on the occlusal surfaces of the teeth” (BOUCHER)

Differences Between Natural & Artificial Occlusion NATURAL TEETH ARTIFICIAL TEETH Natural teeth function independently Artificial teeth function as a group and each individual tooth disperses the occlusal loads are not individually the occlusal load managed Malocclusion can be problematic for a long time non- Malocclusions invokes an immediate response and involves all of the teeth and base Non-vertical tolerated well Non-vertical forces supporting tissues forces are damage the Incising does not affect the posterior Incising will lift the posterior part of teeth. the denture Essentials of Complete Denture Prosthodontics, 2 nd Edition, Sheldon-Winkler.

NATURAL TEETH ARTIFICIAL TEETH The second molar is the favored area Heavy mastication over the second for heavy mastication for better molar can tilt or shift the denture base leverage and power Bilateral balance is not necessary and Bilateral balance is mandatory to is usually considered a hindrance produce stability of the denture Proprioceptive impulses give feedback to avoid occlusal prematurities. This helps the patient to have a habitual occlusion away from centric relation There is no feedback and the denture rests in centric relation. Any prematurities in this position can shift the base Teeth are retained by perio. tissues. Teeth are on bases seated on slippery When teeth are lost, occlusion and bases attachment with its proprioceptive feedback mechanism is lost Essentials of Complete Denture Prosthodontics, 2 nd Edition, Sheldon-Winkler.

Sear‘s Axioms of Complete Denture Occlusion Sears published the following factors to be considered that helps to plan a complete denture occlusion Smaller the area of the occlusal surface, the lesser is the amount of occlusal load transmitted to the supporting structures Vertical force on a tilted occlusion surface will produce a nonvertical force on the denture Vertical forces acting on a tilted tissue support will produce a nonvertical force on the denture base Vertical force on the denture base lying over the resilient tissues will produce lever forces on the denture Vertical forces acting outside the ridge crest will produce tipping of the denture

Ideal Requirements of Complete Denture Occlusion Stability of the denture and its occlusion when the mandible is in both centric and eccentric relations Balanced occlusal contacts (tripod contact) during all eccentric movements Unlocking (removing interferences) the cusps mesiodistally so that the denture can settle The cuspal height should be reduced to control the horizontal forces Essentials of Complete Denture Prosthodontics, 2 nd Edition, Sheldon-Winkler.

Functional lever balance should be obtained by vertical tooth to ridge crest relationship Cutting, penetrating and shearing efficiency of the occlusal surface is equivalent to that of natural dentition Incisal clearance during posterior functions like chewing Minimal area of contact to reduce pressure while crushing food (Lingualized occlusion) Sharp ridges, cusps and sluiceways to increase masticating efficiency Boucher’s Prosthodontic Treatment for Edentulous Patient”, 12 th edition, Zarb-Bolender

Concepts of Occlusion Balanced occlusion Monoplane occlusion Lingualized occlusion Organic occlusion Neutrocentric occlusion

Balanced Occlusion Balanced occlusion can be described as the position of the teeth such that they have simultaneous contact in centric relation and provide a smooth sliding motion to any eccentric position A three-point contact (usually one anterior and two posterior) at centric relation is not sufficient for balanced occlusion instead there should be simultaneous contact of all the teeth Balanced occlusion is absent in natural dentition

Characteristic Requirements of Balanced Occlusion A balanced occlusion should have the following characteristics: All the teeth of the working side (central incisor to second molar) should glide evenly against the opposing teeth No single tooth should produce any interference or disocclusion of the other teeth There should be contacts in the balancing side, but they should not interfere with the smooth gliding movements of the working side There should be simultaneous contact during protrusion.

Importance of Balanced Occlusion Balanced occlusion is one of the most important factors that affect denture stability. Absence of occlusal balance will result in leverage of the denture during mandibular movement The bilateral balanced occlusion is more important during activities such as swallowing saliva, closing to reseat the denture, and the bruxing of the teeth during times of stress

Application of Physical Laws Wider & larger ridge - closer the teeth to ridge - greater the lever balance Smaller & narrower ridge - farther the teeth from ridge - poorer the lever balance Wider the ridge - narrower the teeth buccolingually - greater the balance Narrower the ridge - wider the teeth - poorer the balance

More centered the force of occlusion – anteroposteriorly - greater the stability More lingual the teeth to the ridge - greater the balance More buccal - poorer the balance

Types of Balanced Occlusion balance or balanced occlusion can be classified as follows: Unilateral lever balance Unilateral occlusal balance Bilateral occlusal balance Protrusive occlusal balance Lateral balance Essentials of Complete Denture Prosthodontics, 2 nd Edition, Sheldon-Winkler.

Unilateral Lever Balance This is present when there is equilibrium of the base on its supporting tissues when a bolus of food is interposed between the teeth on one side and a space exists between teeth on the opposite side This state of equilibrium is encouraged by: 1. Placing the teeth so that the resultant force is over the ridge or slightly lingual to it 2. Having denture base cover as wide area as possible 3. Placing the teeth as close to ridge as possible 4. Using as narrow buccolingual width teeth as possible Essentials of Complete Denture Prosthodontics, 2 nd Edition, Sheldon-Winkler.

Bilateral Balanced Occlusion This is a type of occlusion that is seen when simultaneous contact occurs on both sides in centric and eccentric positions Bilateral balanced occlusion helps to distribute the occlusal load evenly across the arch and therefore helps to improve stability of the denture during centric, eccentric or parafunctional movements For minimal occlusal balance, there should be at least three points of contact on the occlusal plane

More the number of contacts, better the balance. Bilateral balanced occlusion can be protrusive or lateral balance Advantages: Better masticatory efficiency Better stability of denture base Reduced trauma, improved comfort The functional movements are possible Disadvantages: Time consuming Cannot be used in all patients

Protrusive Balanced Occlusion This type of balanced occlusion is present when mandible moves in a forward direction and the occlusal contacts are smooth and simultaneous anteriorly and posteriorly There should be at least three points of contact in the occlusal plane. Two of these should be located posteriorly and one should be located in the anterior region. This is absent in natural dentition

Lateral Balanced Occlusion In lateral balance, there will be a minimal simultaneous three point contact (one anterior, two posterior) present during lateral movement of the mandible Absent in natural dentition Important as it prevents leverage action in dentures

Concepts Proposed to Attain Balanced Occlusion Gysi’s Concept He proposed the first concept towards balanced occlusion in 1914 He suggested that arranging 33° anatomic teeth could be used under various movements of the articulator to enhance the stability of the denture
 He proposed lowering the lower occlusal plane to increase the stability")
French’s Concept (1954) He proposed lowering the lower occlusal plane to increase the stability of the dentures along with balanced occlusion He arranged upper first premolars with 5° inclination, upper second premolars with 10° inclination and upper molars with 15° inclination He used modified French teeth to obtain balanced occlusion

Sears’s Concept He proposed balanced occlusion for non-anatomical teeth using posterior balancing ramps or an occlusal plane which curves anteroposteriorly and laterally

Pleasure’s Concept Pleasure introduced a pleasure curve or the posterior reverse lateral curve to align and arrange the posterior teeth in order to increase the stability of the denture.

Frush’s Concept He advised arranging teeth in a one-dimensional contact relationship, which should be reshaped during try-in to obtain balanced occlusion

Hanau’s Quint Rudolph L. Hanau proposed nine factors that govern the articulation of artificial teeth. They are: 1. Horizontal condylar inclination 2. Compensating curve 3. Protrusive incisal guidance 4. Plane of orientation 5. Buccolingual inclination of tooth axis 6. Sagittal condylar pathway 7. Sagittal incisal guidance 8. Tooth alignment 9. Relative cusp height Bernard Levin: A reevaluation of Hanau’s laws of Articulation and the Hanau quint, : 3: 39, 1978

These nine factors are called the laws of balanced articulation Hanau later condensed these nine factors and formulated five factors, which are commonly known as Hanau’s quint

Condylar guidance Incisal guidance Compensating curves Relative cusp height Plane of orientation of the occlusal plane
 He reviewed and simplified Hanau’s quint and proposed his")
Trapozzano’s Concept of Occlusion (1963) He reviewed and simplified Hanau’s quint and proposed his Triad of Occlusion According to him, only three factors are necessary to produce balanced occlusion Condylar guidance Incisal guidance Relative cusp height Trapozzano, V. R: Laws of articulation. J Prosthet Dent 13: 34, 1963
 Boucher confronted Trapozzano’s concept and proposed that there are three fixed")
Boucher’s Concept (1963) Boucher confronted Trapozzano’s concept and proposed that there are three fixed factors for balanced occlusion: 1. Orientation of the occlusal plane, the incisal guidance and the condylar guidance 2. The angulation of the cusp is more important than the height of the cusp 3. The compensating curve enables one to increase the height of the cusp without changing the form of the teeth Boucher, C O: Discussion of laws of Articulation. J Prosthet Dent 13: 45, 1963

He also stated that, “the plane of occlusion should be oriented exactly as it was when natural teeth were present” Boucher also emphasized the need for the compensating curve. He stated that, “the value of the compensating curve is that it permits alteration of cusp height without changing the form of the manufactured teeth… If the teeth themselves do not have any cusps, the equivalence of a cusp can be produced by a compensating curve”
 Lott studied Hanau’s work and clarified laws of occlusion by relating")
Lott’s Concept (1962) Lott studied Hanau’s work and clarified laws of occlusion by relating them to the posterior separation that is a resultant of the guiding factors. He stated the laws as follows: The greater the angle of the condylar path, the greater is the posterior separation during protrusion The greater the angle of the overbite, the greater is the separation in the anterior and posterior regions irrespective of the angle of the condylar path The greater the separation of the posterior teeth, the greater, or higher must be the compensating curve J Prosthet Dent. March 1978 vol 39 no 3

Posterior separation beyond the balancing ability of the compensating curve can be balanced by the introduction of the plane of orientation The greater the separation of the teeth, the greater must be the height of the cusps of the posterior teeth
 Bernard Levin believed that it was not necessary to consider the")
Levin’s Concept (1978) Bernard Levin believed that it was not necessary to consider the plane of occlusion Levin also states that the plane of occlusion can be slightly altered by 1 -2 mm in order to improve the stability of a denture He named the other four factors of occlusion as The Quad

The essentials of a quad are: 1. The condylar guidance is fixed and is recorded from the patient. The balancing condylar guidance will include the Bennett movement of the working condyle. This may or may not affect the lateral balance 2. The incisal guidance is usually obtained from patient’s aesthetic and phonetic requirements. However, it can be modified for special requirements. E. g. , the incisal guidance is decreased for flat ridges

1. 3. The compensating curve is the most important factor in obtaining occlusal balance. Monoplane or low cusp teeth must employ the use of compensating curve 2. 4. Cusp teeth have the inclines necessary for balanced occlusion but nearly always are used with a compensating curve

Factors Influencing Balanced Occlusion 1. Inclination of the condylar path or condylar guidance 2. Inclination of the Incisal guidance 3. Orientation of the plane of occlusion or occlusal plane 4. Cuspal angulation 5. Compensating curves Essentials of Complete Denture Prosthodontics, 2 nd Edition, Sheldon-Winkler.

Condylar Guidance Inclination of the condylar path is also called as the first factor of occlusion. This is the only factor, which can be recorded from the patient Inclination of condylar guidance is a definite anatomic feature that depends on inclination of floor of glenoid fossa. Dentist cannot alter this inclination

It is registered using protrusive registration (i. e. the patient is asked to protrude with the occlusal rims) Inter-occlusal record material is injected between the occlusal rims in this position The occlusal rims with the inter occlusal record are transferred to the articulation

Since the occlusal rims are in a protrusive relation, the upper member of the articulator is moved back to accommodate them. The inter-occlusal record is carefully removed and the upper member is allowed to slide forward to its original position. The condylar guidance should be adjusted till the upper member slides freely into position. It is transferred to the articulator as the condylar guidance

Increase in the condylar guidance will increase the jaw separation during protrusion This factor of balance occlusion cannot be modified. All the other four factors of occlusion should be modified to compensate the effects of this factor In patients with a steep condylar guidance, the incisal guidance should be decreased to reduce the amount of jaw separation produced during protrusion.

It should be remembered that the incisal guidance cannot be made very steep because it has its own ill effects

Incisal Guidance This is defined as, “The influence of the contacting surface of the mandibular and maxillary anterior teeth on mandibular movements” Is expressed in degrees of angulation from the horizontal by a line drawn in the sagittal plane between the incisal edges of the upper & lower incisor teeth when closed in centric occlusion.

If the incisal guidance is steep: It requires steep cusps A steep occlusal plane or a steep compensating curve — to achieve an occlusal balance

Incisal guidance is determined by relationship of mandibular anterior teeth to lingual surfaces of maxillary anterior teeth This angle is formed by lingual surfaces of incisor teeth and horizontal plane of articulator

Incisal guide angle can be controlled when developing a balanced occlusion With a given amount of vertical overlap the incisal guide angle can be made flatter by increasing the horizontal overlap It can be made less steep by reducing vertical overlap

In a complete denture, the incisal guide angle should be as flat (more acute) as possible Hence, while arranging the anterior teeth, for aesthetics, a suitable vertical overlap and a horizontal overlap should be chosen to achieve balanced occlusion Also, the incisal guidance cannot be altered beyond limits The location and angulation of the incisors are governed by various factors like aesthetics, function and phonetics etc

Plane of Occlusion It is defined as, An imaginary surface which is related anatomically to the cranium and which theoretically touches the incisal edges of the incisors and the tips of the occluding surface of the posterior teeth. It is not a plane in the true sense of the word but represents the mean curvature of the surface.
 refers to the vertical location of")
The term “Plane of orientation” (by Hanau) refers to the vertical location of the anteroposterior alignment of the occlusal plane in the space between the upper and lower ridges

It is established In Anterior region: by the height of the lower cuspid, which nearly coincides with commissures of the mouth In posterior region: by the height of the retromolar pad It is usually parallel to the ala-tragus line or Camper’s line

It can be slightly altered and its role is not as important as other factors. Tilting the plane of occlusion beyond 10° is not advisable

Compensating Curve It is defined as “The antero-posterior and lateral curvatures in the alignment of the occluding surfaces and incisal edges of artificial teeth which are used to develop balanced occlusion” – GPT

It is an important factor for establishing balanced occlusion. It is determined by the inclination of the posterior teeth and their vertical relationship to the occlusal plane The posterior teeth should be arranged such that their occlusal surfaces form a curve This curve should be in harmony with the movements of the mandible guided posteriorly by the condylar path

A steep condylar path requires a steep compensatory curve to produce balanced occlusion. If a shallow compensating curve is given for the same situation, there will be loss of balancing molar contacts during protrusion There are two types of compensating curves namely: Anteroposterior curves Lateral curves Curve of Spee, Wilson’s curve and Monson’s curve are associated only with natural dentition. In complete dentures compensating curves similar to these curves should be incorporated to produce balanced occlusion

Anteroposterior Compensating Curves: These are compensatory curves running in an anteroposterior direction. They compensate for the curve of Spee seen in natural dentition

Compensating Curve for Curve of Spee: It is an imaginary curve joining the buccal cusps of the mandibular posterior teeth starting from the canine passing through the head of the condyle. It is seen in the natural dentition and should be reproduced in a complete denture

The significance of this curve is that, when the patient moves his mandible forward, the posterior teeth set on this curve will continue to remain in contact If the teeth are not arranged according to this curve, there will be disocclusion during protrusion of the mandible (Christensen’s phenomenon)

Lateral Compensating Curves These curves run transversely from one side of the arch to the other. The following curves fall in this category: Compensating curve for Monson Curve: Monson’s curve is defined as, “The curve of occlusion in which each cusp and incisal edge touches or conforms to a segment of the sphere of 8 inches in diameter with its center in the region of the Glabella”. GPT

This curve runs across the palatal and buccal cusps of the maxillary molars During lateral movement the mandibular lingual cusps on the working side should slide along the inner inclines of the maxillary buccal cusp In the balancing side the mandibular buccal cusps should contact the inner inclines of the maxillary palatal cusp. This relationship forms a balance

Compensating Curve for Anti. Monson or Wilson’s Curve Wilson’s curve is defined as, “A curve of occlusion which is convex upwards” – GPT This curve runs opposite to the direction of the Monson’s curve This curve is followed when the first premolars are arranged The premolars are arranged according to this curve so that they do not produce any interference to lateral movements.

Pleasure Curve A curve of occlusion which in transverse crosssection conforms to a line which is convex upward except for the last molars – GPT It was proposed by Max Pleasure. He proposed this curve to balance the occlusion and increase the stability of the denture

Hence the first molar is horizontal, the second premolar is lingually tilted and second molar is buccally tilted It is a modification of reverse curve, it does not involve the second molars This curve runs from the palatal cusp of the first premolar to the distobuccal cusp of the second molar

Thielmann’s Formula In order to obtain smooth balanced occlusion, the compensating curve must be in harmony with other factors of occlusion This relationship is expressed in Hanau Quint. It is expressed even more clearly by Thielmann’s formula

K. I Balanced occlusion = OP. C. OK K – inclination of condylar guidance I – inclination of incisal guidance C – height of cusps OP – inclination of plane of orientation OK – prominence of compensating curve

With the condylar inclination determined & set and the Incline guidance established, a perpendicular from each guide plane Will intersect at point 0. This point is the radius for the occlusal plane & cusp inclines that must be set to establish balance occlusion.

When the incisal guidance & the condyle inclination are parallel to one another, there is no intersection & the occlusal plane is set parallel to each for balance occlusion. lif the incisal guidance is steeper than the condylar inclination the intersection for the perpendiculars is below the occlusal plane & balance occlusion is not possible. l

Cuspal Angulation Cusp angle is defined as, “The angle made by the average slope of a cusp with the cusp plane measured mesiodistally or buccolingually” – GPT The cusps on the teeth or the inclination of the cuspless teeth are important factors that modify the effect of plane of occlusion and the compensating curves

In cases with a shallow overbite, the cuspal angle should be reduced to balance the incisal guidance. This is done because the jaw separation will be less in cases with a decreased overbite Teeth with steep cusps will produce occlusal interference in these cases In cases with a deep bite (steep incisal guidance), the jaw separation is more during protrusion. Teeth with high cuspal inclines are required in these cases to produce posterior contact during protrusion

Controversies Regarding Balancing Sheppard stated that, “Enter bolus, Exit balance” According to this statement, the balancing contact is absent when food enters the oral cavity This makes us think that balanced occlusion has no function during mastication; hence, it is not essential in a complete denture. But this is not true

The advantage of balanced occlusion however occurs when the teeth do finally penetrate the food in eccentric position the all-around contact reseals the dentures

Brewer and Hudson reported the importance of balanced occlusion. He stated that on an average, a normal individual makes masticatory tooth contact only for 10 minutes in one full day compared to 4 hours of total tooth contact during other functions So, for these 4 hours of tooth contact, balanced occlusion is important to maintain the stability of the denture. Hence, balanced occlusion is more critical during parafunctional movements.

Pleasure curve Its a concept of posterior occlusion � Pleasure suggested this aids in retention of lower denture during those phases of mastication when bolus of food is between teeth and tooth contact has not yet occured � Non anatomic teeth are used � Pre molars and first molars are set in anti monson curve. �

Pressure transmitted through bolus creates a force that eliminates buccal tipping and seats the denture. � To provide eccentric balance the second molars are set in conventional monson curve � This combination of monson and anti monson curve in posterior occlusion is referred to as pleasure �
 in Balanced Occlusion) Cusped artificial teeth are of")
Class I (Arranging Cusped Teeth (33°) in Balanced Occlusion) Cusped artificial teeth are of varying degrees of cuspal angles, usually 20°, 30°, or 33°. The choice will depend on the determinants discussed, but some adjustment to the teeth will be inevitable Anterior teeth – set first to their correct positions as indicated by esthetics

Canine relationship - the distal incline of the lower canine is overlapped by the mesial incline of the upper canine

Setting Mandibular Teeth Before Corresponding Maxillary Teeth are Set It is easier to correct the compensatory curve when the lowers are set first because the determinig factors of the condylar inclination and incisal guidance can be readily analysed st nd l. Mandibular 1 of 2 premolar is set to confirm to the shape of the residual ridge. l. First premolars are the key to relative anteroposterior intercuspation of all the remaining posterior teeth l

The compensating curve will start with the first molar. l. The mesial cusps of the molar are on the plane established by the canines and bicuspids. l. The distal cusp of first molar is raised 0. 5 mm above this plane l. The second molar continues the cuspal elevation of the compensatory curve l

Setting Maxillary Teeth Maxillary posterior teeth are set starting with the first premolar and continuing up to the 2 nd molar Teeth are arranged in CR & finally balance is completed after all the posterior teeth is set in position
 Compensating Curve With cuspless teeth, it is")
Arranging Cuspless Teeth in Occlusion (0 °) Compensating Curve With cuspless teeth, it is necessary to use 0° incisal guide table to develop balancing contacts in protrusive relation Difference is due to the absence of cuspal height in non-anatomic teeth. In these situations, protrusive lateral balance can be attained by the use of a 2 nd molar ramp
 Plane of occlusion should have proper orientation A compensating")
Balancing the occlusion (Anterior teeth) Plane of occlusion should have proper orientation A compensating curve must be set Teeth must be modified so that there are no interlocking transverse ridges
 ▪Gently grind")
Selective Grinding – For Anatomic Teeth For Static Centric Contacts (in CO) ▪Gently grind the inclines on the lower cusp ▪Upper lingual cusps should never be ground ▪Lower central fossa (or) marginal ridge should be ground

If any upper buccal inclines or cusps are in contact, they should be ground out of contact Only upper lingual cusp (pestle) of the mortar and pestle type lingual contact occlusion should actuate with the lower posteriors

For Working & Balancing Contacts When the mandible moves to left, this is the working side (upper left lingual cusps should contact the lower left lingual cusp) Right side is then the balancing side and here the upper lingual cusps should contact the lower buccal cusps
 is")
Working side intereference -the non supporting cusps (upper buccal or lower lingual) is adjusted. Non working side interferences -interferences occur between the upper palatal cusp inclines and the inclines of the lower buccal cusps - those parts of the inclines causing the interference are adjusted, and their relationship in intercuspation constantly checked -if cusp heights must be changed, preserve the upper palatal cusp and adjust the lower.

For Protrusive Balance Upper right and left 2 nd molar cusps should slide up the distal inclines of the lower right and left 2 nd molars with no anterior interference Surfaces of any ground teeth should be polished to eliminate friction between occluding surfaces

Anterior interference-the inciso-labial surfaces of lowers are adjusted. � Posterior interference-offending cuspal inclines(distal inclines of upper cusps and mesial inclines of lower cusps) are adjusted �
 Contacts judiciously ground until there are linear contacts")
Selective Grinding (For Non. Anatomic Teeth) Contacts judiciously ground until there are linear contacts from 1 st premolar to 2 nd molar No working or balancing cusp contacts. The left lateral excursion should be a free milling type of occlusion that is free of tipping on the balancing side There should be adequate anterior clearance

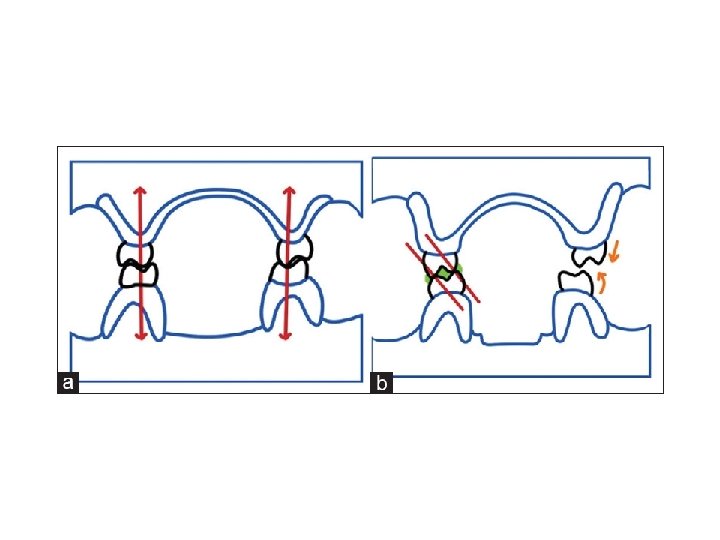
Class II Ridge Relationship When the crest of the lower ridge is placed lingual to the upper ridge Canine relationship Upper canine is placed forward i. e. distal incline of upper canine contacts mesial incline of the lower canine Curtis T. A. , Langer Y. , Curtis D. A. and Carpenter R. (1988): Occlusal considerations for partially or completely edentulous skeletal class II patients. Part I: background information. Journal of Prosthetic Dentistry 60: 202 -211.

Anterior teeth Set first to their correct positions as indicated by esthetics Class II occlusion using either modified anatomic teeth or flat teeth

Setting Mandibular Teeth First Lower anteriors are set first for lip support After the lower premolars are initially set, the upper first premolar is temporarily set to evaluate its position. It’ll have a marked buccal overlap with the opposing lower buccal cusp 2 nd premolar is not placed as buccally as the 1 st premolar. After these, molars are set to create a compensating curve in harmony with condylar inclination and incisal guidance

Setting Maxillary Posterior Teeth Upper 1 st premolar set with its flattened lingual cusp occluding with the flattened buccal cusp of the lower 1 st premolar. In severe retrusions, it may also be out of contact in centric occlusion Upper 2 nd premolar is set with its flattened lingual cusp occluding with the flattened buccal cusp of lower 2 nd premolar, with less buccal overlap and larger area of contact.

Upper molars can be set with their lingual cusps in the modified central fossa of the lower teeth Posterior teeth now should have a centric occlusion with stable non deflective stops

Selective Grinding for Class II Occlusion developed for Class II patient is balanced by selective grinding with the same basic procedures applied to the conventional lingual contact scheme They are: In C. O – selectively grind all contacts in the lower teeth until all of the upper lingual cusps contact Working side contacts are the buccal cusps of the upper and lower posterior teeth, cuspid interference, anterior interference

Balancing side contacts – lingual cusps of the upper on the buccal inclines of the lower teeth. In class II premolars do not make balancing contacts, because of buccal overlap taking them out of range during lateral excursion Upper lingual cusps and the lower centric contacting area should be excluded from grinding In protrusive excursions balance achieved by the bilateral contact of the lingual cusps of the upper 2 nd molars with the distal incline of the lower 2 nd molars

Non-Anatomic Teeth for Class II When the lower ridge is severely resorbed and weak; use of non-anatomic teeth is considered Arrangement of 0° teeth set horizontally to a monoplane occlusion directs the force straight down to the ridge

Setting the Mandibular Posterior Teeth For total lever balance; all of the posterior teeth can be set with buccal tilt (pleasure curve) But this prevents balance on the balancing side So for occlusal balance, a lingual tilt given in the posterior arrangement produces a lingualized occlusion

Buccal tilt for the premolars light to heavy Lingual tilt for the 2 nd molar provides a forces lateral balancing contact

Setting the Maxillary Posterior Teeth 1 st premolar is set with lingual tilt to provide stable contact with the lower 1 st premolar with considerable buccal overlap for a stable contact on the working side 2 nd premolar is set with lingual tilt but not with much overlap 1 st and 2 nd molars are set to occlude with typical nonanatomic tooth contacts Curtis T. A. , Langer Y. , Curtis D. A. and Carpenter R. (1988): Occlusal considerations for partially or completely edentulous skeletal class II patients. Part II: treatment concepts. Journal of Prosthetic Dentistry 60: 334 -342.

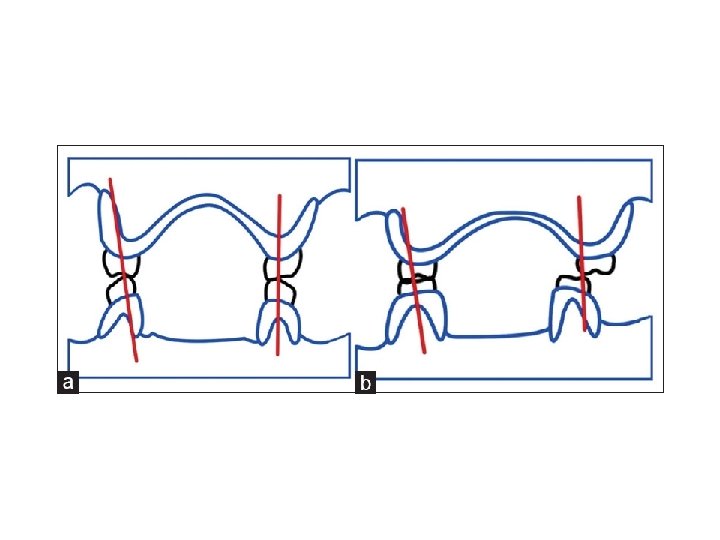
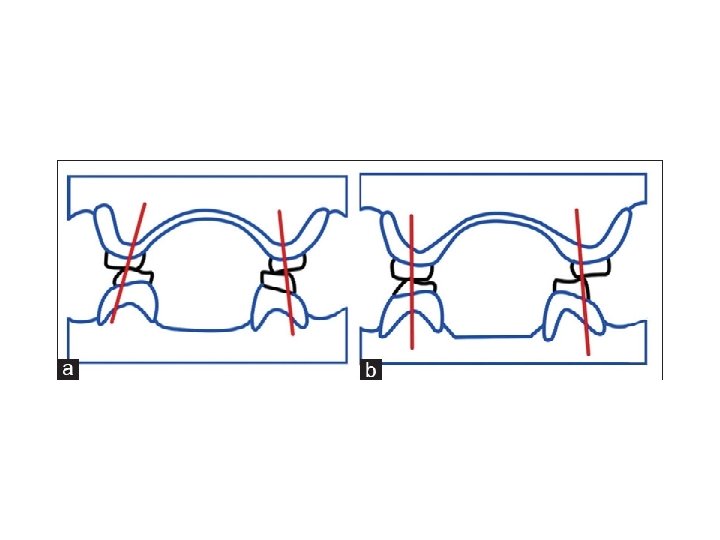
Class III Occlusion Ridge Relationship

Anterior Teeth It is set as forward as esthetics requires for support of the upper lip and to set the lower teeth as far lingual on the ridge as possible without interfering with the tongue Patient treated with this approach looks less prognathic and the anterior teeth can be set edge to edge

Posterior Teeth It can be set in a cross-bite atypical arrangement either with modified anatomic teeth (or) nonanatomic teeth The Buccolingual and Mesiodistal relation of the upper and lower posteriors is not as critical with this type of occlusal form

Setting Mandibular Posterior Teeth Never should we attempt to set the lower posterior teeth under the upper ridge so that the upper and lower posterior will have a conventional occlusal relationship because teeth will be set too far for lingual which will restrict the tongue movements and cause displacement of the lower denture

Setting Maxillary Posterior Teeth 1 st premolar is usually set to typical anatomic relationship. Upper lingual cusp occludes with the modified centric fossa of the lower premolar 2 nd premolar is the transition tooth – where the cross over starts. For stable CO contacts, upper and lower buccal and lingual cusps are flattened and are set buccal to buccal and lingual to lingual

1 st molar cross-bite in is relation the as buccal cusps of the upper molar teeth are on the central fossa of the lower teeth The crossbite relationship need not necessarily be bilaterally symmetrical

Working Anterior side contacts to cross over – upper lingual opposing lower lingual At crossing point no working contacts for modified anatomic set up Posterior to the cross over upper buccal opposing the lower lingual

Balancing side contacts Anterior to cross over upper lingual cusp opposing lower buccal cusps At crossing point no balance contact, because of the cuspal rise Posterior to the cross over upper buccal cusp opposing lower buccal cusps

Protrusive Cusp Contacts Anterior teeth variable, depending on anterior relationship When the anterior teeth are set edge to edge no balance contacts for protrusive excursions When there is slight horizontal overlap protrusion brings upper and lower anterior teeth edge to edge Posterior teeth – upper 2 nd molar buccal cusps on lower 2 nd molar distal inclines

Summary Balanced occlusion is the simultaneous contacting of teeth in centric and all eccentric positions. It ensures even pressure in all parts of the arch, which maintains the stability of the dentures when the mandible is in centric and eccentric positions. Its importance includes even contacts during parafunctional activities, while closing to reseat dentures and also while swallowing saliva.

Different concepts were given by Hanau, Trappozano, Boucher, Lott and Levin to attain balanced occlusion. The factors influencing balanced occlusion include Inclination of the condylar guidance, Inclination of the incisal guidance, Orientation of the occlusal plane, Inclination of the cusps, and Prominence of the compensating curve.

Conclusion The importance of occlusion and articulation for maintenance of CD stability has never been underestimated, but overlooked No matter how great amount of initial retention, the impression may demonstrate, the occlusion we are going to provide gives more stability which indirectly gives the retention

“Balanced occlusion is making a stumbling prose into a beautiful poem” so dentist (prosthodontist) should provide occlusion, which is compatible with the stomatognathic system and should provide efficient mastication and esthetics, without any physiologic abnormality

References Boucher’s Prosthodontic Treatment for Edentulous Patient”, 12 th edition, Zarb-Bolender. Essentials of Complete Denture Prosthodotics, 2 nd Edition, Sheldon-Winkler. . Text Book of Complete Dentures, 5 th edition, Rahn, Charles Heartwell. Complete Denture Prosthodontics – Sharry.
:")
Curtis T. A. , Langer Y. , Curtis D. A. and Carpenter R. (1988): Occlusal considerations for partially or completely edentulous skeletal class II patients. Part I: background linformation. Journal of Prosthetic Dentistry 60: 202211 l. J Prosthet Dent March 1978 vol 39 no 3 l. Bernard Levin: A reevaluation of Hanau’s laws of Articulation and the Hanau quint, : 3: 39, 1978 l. Trapozzano, V. R: Laws of articulation. J Prosthet Dent 13: 34, 1963 l. Boucher, C O: Discussion of laws of Articulation. J Prosthet Dent 13: 45, 1963 l
- Slides: 120