Balance Exercise with Myasthenia Gravis John Utz MSPT

Balance & Exercise with Myasthenia Gravis John Utz, MSPT, CSCS Owner
")
MG Workshop - 2017 �Objectives: Participants will… Understand the mechanism behind Myasthenia Gravis (MG) and how that relates to symptoms. Relative to MG, understand what role exercise and balance training can have in helping improve functional capacity. Define balance and understand the functionally significant components. 1. 2. 3. 1. 2. 4. 5. Discuss the sensory systems involved with establishing your “reference of correctness” (sensory perception). Learn about the conscious and unconscious mechanisms involved with preventing a fall (motor execution). Participate in interactive balance drills. Q &A – Advice

MG at the Neuromuscular Junction

Cellular Mechanism of MG � 50 -80% reduction in the number of receptor sites. �Reduction caused by an antibody that destroys or blocks the receptor site. �Antibodies usually attack foreign proteins like bacteria and viruses. (which is good. ) �For reasons not well understood, in MG, the immune system makes antibodies attack receptor sites at muscle (which is bad) �The antibodies destroy the receptor sites more rapidly than the body can replace them. �Muscle weakness occurs when acetylcholine cannot activate enough receptor sites at the neuromuscular junction.

Neuromuscular Junction with MG

So What? �MG will effectively weaken any voluntary muscle being overused. Two types: �Ocular � Ptosis (drooping eyelid), Diplopia (double vision) �Generalized � Slurred speech � Difficulty chewing and swallowing � Weakness in the arms and legs � Chronic muscle fatigue � Difficulty breathing �Symptoms can improve with rest of fatigued muscle.

“Snowflake disease” �Each presentation of MG is unique to the individual. �What muscles affected �What creates symptom exacerbation (heat, humidity, time of day, duration of sleep, stress, colds/flu/illness, nutrition, medication, etc) �Other pre-existing or health concerns – LBP, OA, anything… �Lifestyle, Habits and Hobbies �Occupation �Social situation – family support?

So if rest is good, why exercise? �If stable, then consistent, appropriate/moderate exercise tailored for the individual can elevate your baseline functional capacity and lessen the effects of MG exacerbation. Naumes et al. , Int J Neurorehabilitation Eng 2016, 3: 3 �Always consult with your doctor before starting any exercise. �If MG is not stable or medically managed, then unsupervised exercise could make symptoms worse.

Benefits of moderate exercise Naumes et al. , Int J Neurorehabilitation Eng 2016, 3: 3 �Improve body mechanics and posture �Improve balance and decrease fall risks �Breathing efficiency �Reduce potential for injury �Maximize energy conservation �If done correctly, same benefits for those without MG Time Magazine – “The Science of Exercise” �“Professional supervision is recommended to individualize the program. Rehabilitation professionals are highly trained to accommodate for fatigue and weakness. ”

Exercise considerations �During an Exacerbation, Exercise is not appropriate. �Energy Conservation is essential. Be Safe. Rest! �Mobility utilizing assistive devices if necessary �Fall Prevention �Home Modification (grab bars, decreasing fall risks, removing throw rugs)

Exercise Considerations �Stable MG patients looking to exercise should consider these 5 suggestions: 1. Dollar a day rule (start day at 100%) 2. Exercise at your best time of day (usually am) 3. Exercise at peak dose of MG medication (pyridostigmine) 4. Exercise large proximal muscle groups, short periods, only to moderate intensity. 5. Do not exceed moderate intensity

Exercise considerations �What constitutes moderate? �HR not to exceed 30 BPM above resting �No SOB (shortness of breath) �No symptom exacerbation (drooping eyes, double vision for example) �Should not be tired 2 hours after exercise �No DOMS (delayed onset muscle soreness)

")
Stay cool - (inhibit acetylcholinesterase)

Exercise Options: �To improve respiratory endurance: � Pursed lip breathing �Abdominal Breathing �To Improve Posture: �Scap setting (no shugging) �Grow Talls (cervical retraction)

Exercise Options �To improve Balance: �Definition: Ability to control body’s mass or center of gravity (COG) relative to the base of support (BOS). �It is an automatic and unconscious process that allows individuals to resist the destabilizing effect of gravity.
 How big is the problem? �One in three people over 65")
Balance: Statistics (CDC) How big is the problem? �One in three people over 65 will fall during the next year. �Among older adults, falls are the leading cause of injury deaths. �Falls are the most common cause of nonfatal injuries and hospital admissions. Almost half of hospital admissions from falls become SNF residents (47%). �In 2005, 15, 800 people 65 and older died from injuries related to unintentional falls. �In 2000, direct medical costs totaled $0. 2 billion ($179 million) for fatal falls and 19 billion for nonfatal fall injuries (Stevens et al. 2006).
 How big is the problem? � 1 in 4 people who")
Balance: Statistics (CDC) How big is the problem? � 1 in 4 people who fall suffer injuries severe enough to limit independent living. (Alexander et al. 1992; Sterling et al. 2001). �Most fractures among older adults are caused by falls (Bell et al. 2000). �The most common fractures are of the spine, hip, forearm, leg, ankle, pelvis, upper arm, and hand (Scott 1990). �Many people who fall, even those who are not injured, develop a fear of falling. This fear may cause them to limit their activities, leading to reduced mobility and physical fitness, and increasing their actual risk of falling (Vellas et al. 1997).

Functionally Significant Components of Balance: �Sensory input and processing. �Recognition of body position in relation to self and the environment. “reference of correctness” �Motor planning and execution. �Generation of movement sufficient to maintain balance and perform the chosen task.

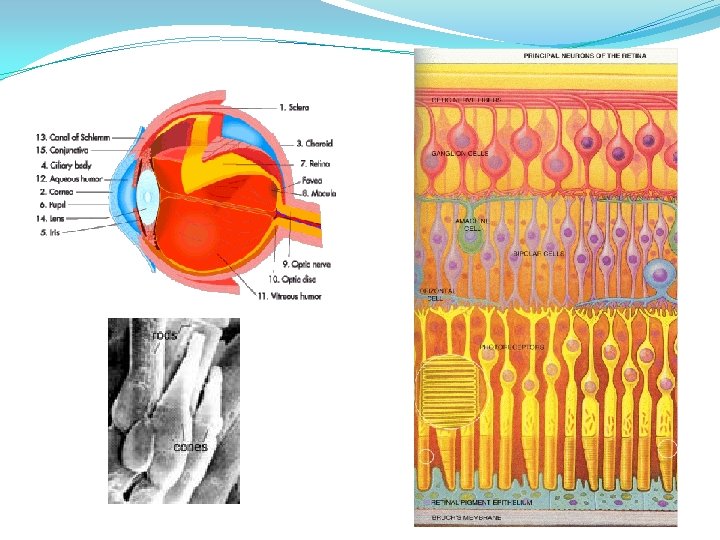
Sensory Input and Balance �Three peripheral sensory systems involved with determining your “reference of correctness” �Vision – rods and cones �Somatosensation / Proprioception – GTO’s, Jt. Receptors, MM Spindles, Corpuscles, and Discs. �Vestibular – semicircular canals, utricle, and saccule. �Central mechanisms are involved with comparing the bilateral input from the peripheral systems above. �Sensory Conflict?

Sensory Input Vision �Rods and Cones - Contain photoreceptors (pigments that change their 3 -D structure when hit by light). �Rods – pigment most sensitive to black and white (night vision mostly). �Cones – pigment most sensitive to particular wavelengths of light (red, green and blue) and used during the day.

Sensory Input Vision – eye movement � 5 types of eye movement that each serve a unique function. 1. Saccades 1. Vergence 1. Persuit 1. VOR 1. OKR (optokenetic response) assists VOR when image falls on larger part of retina – not just fovea.

Sensory Input Vision

Sensory Input Somatosensation / Proprioception �Afferent Nerve Fibers – toward the SC / Brain Light touch � Sharp / dull � Hot / Cold � Vibration � Pressure � Pain � Position sense � Stereognosis � Graphesthesia � �Info goes into the posterior root of a spinal nerve. �Efferent Nerve Fibers – toward the muscles / extremities. � Motor Unit – a group of muscle fibers under the control of ONE nerve fiber.

Sensory Input Vestibular

Sensory Input Vestibular

Sensory Input - Vestibular

Sensory Conflict? �Eyes, Somatosensation and Vestibular all need to work together. - Car analogy. �Compensations visual dependence > look down > postural changes > COG dark rooms? uneven surfaces? shuffled gait?

Motor Execution and Balance �Postural Maintenance �Anticipatory Reactions – postural adjustments during self-initiated movement or in anticipation of destabilizing forces. �Equilibrium Reactions – postural adjustments made in response to an unexpected, external force (aka: balance strategies, automatic reactions).

Motor Execution Postural Maintenance �Quiet stance and sway �Width of support �Deformities (kyphosis or FHP) �Length-Tension of Muscles �Important component to consider when evaluating a patient.

Motor Execution Anticipatory Reactions �Helps counterbalance inertia of self-initiated movement. �Not a reflex. Show specificity to intended movement. �Dependent on: � Initial conditions of body (posture, flexibility, strength, cognition, etc. ) � Speed of movement � Direction of movement � Amplitude of movement �Research regarding � Cordo and Nasher, 1982; Nardone and Schieppati, 1988

Motor Execution Equilibrium Reactions �Four major strategies used in response to unexpected LOB. A. Ankle Strategy B. Hip Strategy C. Suspensory Strategy D. Stepping Strategy
 depends on")
Motor Execution Equilibrium Reactions �The strategy selected (ankle vs. hip vs. step) depends on four things: 1. Position of COG over the base of support. � 2. where is the patient within their cone of stability to start? Type of support surface (environment) soft, narrow, static, dynamic…? � 3. Speed of movement / severity of perturbation 4. Physiologic factors � � Available ROM at joints Strength (especially at ankles and hips) Static postural alignment Neurologic ability to execute appropriate strategy (timing, amplitude, sequencing).

Common Changes with Age �Visual System – decreased visual acuity, contrast sensitivity, dark adaptation, accommodation, color vision, and motor control. �Somatosensory system - ? ? ? Some corpuscles change in morphology. Proprioception loss is controversial and may be joint specific. Decline in afferent fibers within CNS not consistent until 90 years. �Vestibular System – Definite (20 -40%) decline in hair cells of saccule, utricle and semicircular canal. �Presbyastasis – age related dysequilibrium when no other pathology is found. Patients with vertigo, nystagmus, and imbalance must first have vestibular pathology ruled out to ID as presbyastasis.
 �Inner ear dysfunction �BPPV, Hypofunction �Glaucoma and Cataracts �Diabetes")
Common Pathology (Leading to imbalance) �Inner ear dysfunction �BPPV, Hypofunction �Glaucoma and Cataracts �Diabetes / Neuropathy �Stroke / TIA �Head Injury �Medications? �Arthritis �Inflexibility �Osteoporosis �Poor Posture �Muscle Weakness �TKA, THA
 �Exercise regularly; exercise programs like Tai Chi")
How can I prevent a fall? (CDC) �Exercise regularly; exercise programs like Tai Chi that increase strength and improve balance are especially good. �Ask your doctor or pharmacist to review your medicines –both prescription and over-the counter–to reduce side effects and interactions. �Have your eyes checked by an eye doctor at least once a year. �Improve the lighting in your home. �Reduce hazards in their home that can lead to falls. �Participate in vestibular / balance treatment if necessary.

Interactive Drills Feet together, arms crossed. Eyes open. Eyes closed?

Interactive Drills Tandem Stance – heel to toe

Interactive Drills Stand on one foot. Goal = 30 secs

Interactive Drills On toes and reach
. Add coordination drills to increase difficulty.")
Interactive Drills Alternate toe taps on step (book). Add coordination drills to increase difficulty.

Q&A www. UTZPT. com Link to articles under “Services” tab – scroll to bottom of page.
- Slides: 43