Bacterial GI Infections Introduction Gastroenteritis also known as

Bacterial GI Infections
, is inflammation of the")
Introduction • Gastroenteritis, also known as infectious diarrhea (GI Flu), is inflammation of the gastrointestinal tract • Gastroenteritis can be due to infections by viruses, bacteria, parasites, and fungus • It is estimated that three to five billion cases of gastroenteritis resulting in 1. 4 million deaths occur globally each year. • Children and those in the developing world are most commonly affected and associated with high mortality rates • It is less common in adults, partly due to the development of immunity

• Signs and symptoms include some combination of diarrhea, vomiting, and abdominal pain. Fever, lack of energy, and dehydration may also occur. • Gastroenteritis typically involves both diarrhea and vomiting • Less commonly, presents with only one or the other. • Abdominal cramping may also be present.

• Signs and symptoms usually begin 12– 72 hours after contracting the infectious agent. • If due to a viral agent, the condition usually resolves within one week. • Some viral causes may also be associated with fever, fatigue, headache, and muscle pain. • If the stool is bloody, the cause is less likely to be viral and more likely to be bacterial. • Some bacterial infections may be associated with severe abdominal pain and may persist for several weeks

• In the developed world Campylobacter jejuni is the primary cause of bacterial gastroenteritis, with half of these cases associated with exposure to poultry. In children, bacteria are the cause in about 15% of cases, with the most common types being Escherichia coli, Salmonella, Shigella, and Campylobacter species. • In the developing world, especially sub-Saharan Africa and Asia, cholera is a common cause of gastroenteritis.

Bacterial gastroenteritis • Bacterial intestinal infection: usually following contaminated water/food • Some foods commonly associated with illness include raw or undercooked meat, poultry, seafood, and eggs; raw sprouts; unpasteurized milk and soft cheeses • rarely involve other organs and systems • Watery diarrhea: involve small and large intestines • Bloody-diarrhea: (Dysentery ) mostly Large intestine • Enterocolitis: inflammation of mucosa of both small & large intestines due to bacterial cytotoxin

Bacteria Food poisoning • Bacterial food intoxication is another common cause GI illness associated with the presence of a preformed toxin in food • Mostly associated first with vomiting & later diarrhea. . No fever. . • Short incubation period. . 2 -8 hours • In many cases the toxin is produced in the food by bacteria during storage or preparation due to hand or environmental contamination.

Causative agent • • • • Common Gram-ve : Salmonella spp. , Shigellae Various types of diarrheagenic E. coli, Campylobacter spp. , V. cholerae Listeria Aeromonas Gram-positive : Cl. perfingens Cl. difficile, Staphylococcus aureus Bacillus cereus

Salmonella spp • Small, gram-negative rods • Widely distributed in nature • Humans and animals being their primary reservoirs • Salmonella food infection results from ingestion of foods containing appropriate strains of this genus in significant numbers

Salmonella Group • Salmonella: Gram-negative bacilli, Facultative anaerobes, of the Enterobacteriaceae family • By current classification there is only one major species of Salmonella: S. enterica The taxonomic group contains more than 2500 serovars, defined on the basis of presence of a specific set of O ((lipopolysaccharide) , H (flagellar), Vi (Virulence) antigens Salmonella serovars can be divided into two main groups—typhoidal and nontyphoidal Salmonella.

• Nontyphoidal serovars are more common, and usually cause self-limiting gastrointestinal disease. • They can infect a range of animals, and are zoonotic, meaning they can be transferred between humans and other animals. • Typhoidal serovars include Salmonella Typhi and Salmonella Paratyphi A, which are adapted to humans and do not occur in other animals.

• Strains of Salmonella cause illnesses such as typhoid fever, Enteric Fever Salmonellas • and Gastroenteritis/Food-poisoning (salmonellosis) • Typhoid Salmonella infect only humans. . Gastroenteritis Salmonellas infect both humans & Animals and it is widely distributed in nature

Salmonella-Typhoid Fever -1 • S. enterica subtype. Typhi & Paratyphi cause severe human systemic illness, including enteric fever (typhoid fever), blood sepsis. • may be associated with bloody enterocolitis, meningitis, pneumonia, endocarditis, osteomyelitis, septic arthritis, hepatic abscesses, soft tissue abscesses in any body part. • Typhoidal Salmonella develop following invading GI

• sources contaminated water Less by Food Less direct contact highly virulence factors. . Proteinous capsule (Vi antigen), Cell wall Lipopolysaccharides, cytotoxin. . Incubation period 1 -3 weeks. .

• The organisms enter the body in water or food • They invade the mucosa of the upper small intestine • From there it invades lymphoid tissues and are phagocytized and disseminated • The organism multiply in the phagocytes emerge and continue to multiply intracellularly • Bacteremia and septicemia occur at the same time as symptoms appear • During the first week the patient suffers from, headache, malaise, and fever (endotoxin effect)
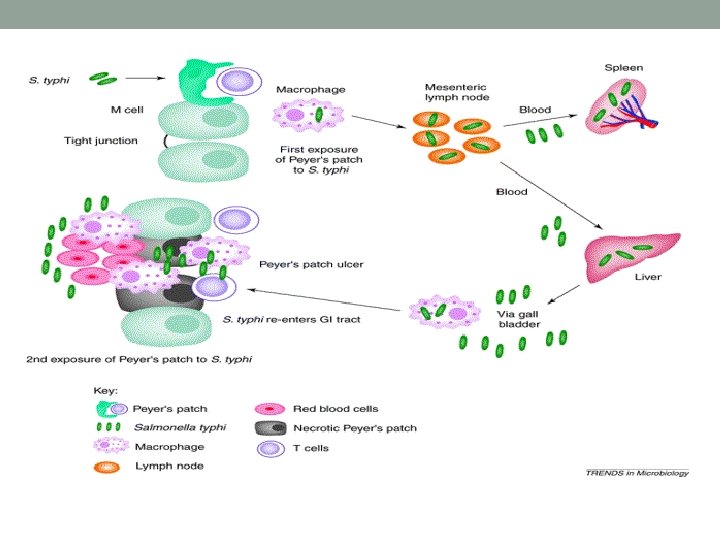

• During the second week the patients condition worsen, the organisms invade many tissues including the intestinal mucosa and are excreted in the stool • Salmonella typhi thrive and multiply in bile • Organisms from the gallbladder reinfect the intestinal mucosa and lymphoid tissue such as peyer’s patches • Characteristic rose spots often appear on the trunk and abdomen for few days • Abdominal distention and tenderness and enlargement of the spleen are common complaints, but diarrhea usually absent • Leukopenia • Some patients become delirious and suffer from

Lab Diagnosis • Definitive diagnosis Typhoid Fever: Requires culture & isolation of the organism from blood, Feces, CSF, Urine Acute- sub-acute cases. • Chronic cases. . bone marrow, Gallbladder. . Healthy Carriers. . execrete bacteria in stool. • Presence bacteria only in stool without clinical disease indicates often carriage state. • Selective culture media: S-S agar, Heckton-enteric agar… Lactose-non-fermenter bacteria growth • Serological test: Widal test is used for the diagnosis of Typhoid fever. . measures levels of antibodies against (O, H ) antigens. . Titer > 160 or rising titers. . positive (Vi ) antigen indicate S. typhi. . acute infection.

Treatment & Prevention • Antibiotic therapy is essential and should begin empirically if clinical evidence is strong. . Ciprofloxacin 4 weeks. . • Due to resistance to ciprofloxacin ceftriaxone is used • Ceftriaxone for pregnant women & Children. . Chloramphenicol & Amoxacillin/Ampicillin is not more used. • Fatality is high without antibiotic treatment • In endemic countries. . Most developing countries. . public health measures to ensure safe drinking water, proper sewage disposal. . Detection of human carries. . Education programs on food hygiene • Vi antigen is used in preparation of oral & injectable vaccine. . short protection. . endemic region. . Used in

Typhoid Mary Mallon: an immigrant, Irish woman who made her way as a cook Well liked and respected ("good with the children") Probably exposed to typhoid fever around 1900 Between 1900 and 1907, she infected 22 people with typhoid fever; one died Quarantined on North Brother Island (age 37) for three years Released by the new health officer after promising never to cook again Traced to Sloan Maternity Hospital as cook! 25 more people infected 2 died Returned to quarantine on North Brother Island Died of a stroke 23 years later (in 1938)

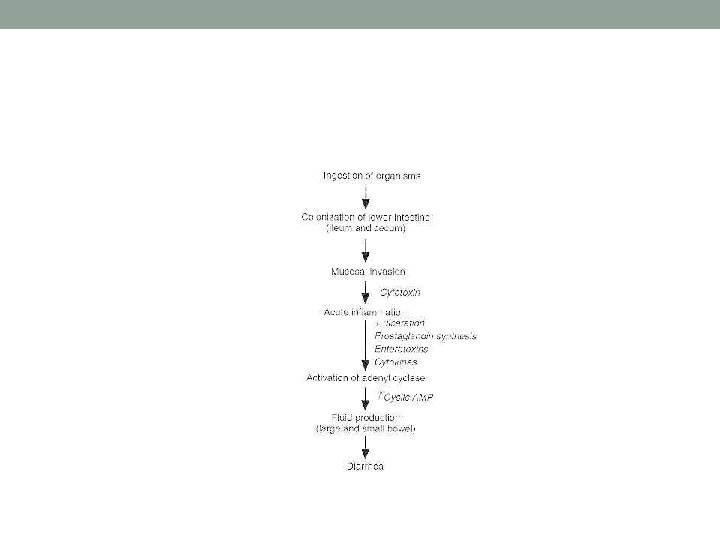
Gastroenteritis/ Food-Poisoning Salmonellas • S. enterica var Typhimurium and S. enterica var Enteritidis are most common serotypes of GI Salmonellosis in humans, chicken, and other animals. . Million of cases each year. Worldwide • Contaminate commonly human fresh food. • After Salmonella ingestion. . invade epithelial cells of small intestine. . multiply in lymphoid follicles. . cause inflammatory response. . Mediates release of prostaglandines. . stimulates c. AMP. . Fluid secretion. . inhibition Na-absorption. Incubation 8 -24 hrs, Waterybloody diarrhea, abdominal pain, fever. . Less vomiting. . Rare complications: septicemia, meningitis developed in neonates, infant, immune- suppression.

Gastroenteritis. Salmonellas-2 • No antimicrobial drugs treatment. . For normal healthy persons. . Only Rehydration. . Antimicrobial drugs used for very young infants & immunosuppressed patients. • Rarely human healthy carriers in intestine. . Clinical cases execrate salmonella for few days-weeks. . • No human vaccine available. • Prevention hand-food hygiene. . often Chicken eggs & meat /Grounded meat. . Dairy Products. • Stool culture. . S-S agar, Heckton-enteric agar • Widal test is not significant in diagnosis of infection.

Shigella • Shigella spp continue to be a major health problem worldwide, causing an estimated 1 million deaths and about 150 million cases of diarrhea annually.
 • Caused by several serovars of Shigella 1. 2. 3. 4.")
Shigellosis (bacillary dysentery) • Caused by several serovars of Shigella 1. 2. 3. 4. Shigella dysenteriae (serovar A) Shigella flexneri (serovar B) Shigella boydii (serovar C) Shigella sonnei (serovar D)

Shigellosis-1 • Shigella are Gram-negative, Lactose non fermenter non motile bacilli • Facultative Anaerobes • Highly susceptible to dryness and Acidity. . killed within 1 hour in stool. • Clinical disease ranges from mild diarrhea to dysentery. . • Most deaths occur in children or elderly persons due to dehydration. . • Infection limited to humans. . • Incub period within 24 hours. . highly communicable . . Person to person contact. . contaminated Water, fresh green leaf vegetables.
, largely because of")
Transmission and Epidemiology • Oral-fecal route • Direct person-to-person contact (hand-to-mouth), largely because of the small infectious dose required (from 10 to 200 bacteria). • The disease is mostly associated with lax sanitation, malnutrition, and crowding; and it is spread epidemically in day care centers, prisons, mental institutions, nursing homes, and military camps. • As in other enteric infections, Shigella can establish a chronic carrier condition in some people that lasts several months.

Signs and Symptoms • Signs and symptoms of Shigellosis can range from mild abdominal discomfort to full-blown dysentery characterized by cramps, diarrhea, with slimy-consistent stools, fever, blood, pus, or mucus in stools or tenesmus

Pathogenesis and Virulence Factors • Shigellosis is different from many GI tract infections in that Shigella invades the villus cells of the large intestine rather than the small intestine. It is not as invasive as Salmonella Does not perforate the intestine or invade the blood It enters the intestinal mucosa by means of lymphoid cells in Peyer’s patches. Once in the mucosa, Shigella elicits an inflammatory response that causes extensive tissue destruction

Virulence factors The release of endotoxin causes fever Enterotoxin, an exotoxin that affects the enteric (or GI) tract, damages the mucosa and villi. Local areas of erosion give rise to bleeding and heavy secretion of mucus Shigella dysenteriae (and perhaps some of the other species) produces a heat-labile exotoxin called shiga toxin, which seems to be responsible for the more serious damage to the intestine as well as any systemic effects, including injury to nerve cells.

Shiga toxin It is an A-B toxin The B portion of the toxin attaches to host cells, and the whole toxin is internalized. • Once inside, the A portion of the toxin exerts its effect. • In the case of the shiga toxin, the A portion of the toxin binds to ribosomes, interrupting protein synthesis and leading to the damage

Diagnosis • Acute case. . Direct stool examination for presence of numerous WBCs and blood cells • Directal swab. . or rapid stool culture of feces on SS agar, Heckton-enteric agar. . Shigella Isolation & confirmation by biochemical tests and serotyping.

Prevention and Treatment • The only prevention of this and most other diarrheal diseases is good hygiene and avoiding contact with infected persons. • Antibiotics is recommended. . ciprofloxacin, doxycycline, cotrimoxazole. . Shorten the diarrhea duration. . Rehydration is important but not enough • Most physicians recommend prompt treatment of shigellosis with trimethoprim-sulfamethoxazole (TMPSMZ).

Diarrheagenic Escherichia coli • Enterohemorrhagic E. coli, or EHEC E. coli O 157: H 7 • Enterotoxigenic E. coli, • Enteroinvasive E. coli, • Enteropathogenic E. coli, • Enteroaggregative E. coli.
. E. coli O 157:")
Enterohemorrhagic E. coli, or EHEC or Vero-toxigenic E. coli (VTEC). E. coli O 157: H 7 • In January of 1993, this awkwardly named bacterium burst into the public’s consciousness when three children died after eating undercooked hamburgers at a fast-food restaurant in Washington State. The cause of their illness was determined to be this particular strain of E. coli, which had actually been recognized since the 1980 s. Since then, it has led to approximately 73, 000 illnesses and about 50 deaths each year in the United States. It is considered an emerging pathogen.

• Dozens of different strains of E. coli exist, many of which cause no disease at all • Some cause various degrees of intestinal symptoms • . Some of them cause urinary tract infections • E. coli O 157: H 7 are the most virulent of them all • The group of E. coli of which this strain is the most famous representative is generally referred to as enterohemorrhagic E. coli, or EHEC

• E. coli O 157: H 7 is the agent of a spectrum of conditions, ranging from mild gastroenteritis with fever to bloody diarrhea • About 10% of patients develop hemolytic uremic syndrome (HUS) A severe hemolytic anemia that can cause kidney damage and failure • Neurological symptoms such as blindness, seizure, and stroke (and long-term debilitation) are also possible. These serious manifestations are most likely to occur in children younger than 5 and in elderly people.

Pathogenesis and Virulence Factors • This bacterium owes much of its virulence to shiga toxins identical to the shiga exotoxin secreted by virulent Shigella species). • Sometimes this E. coli is referred to as STEC (shiga-toxinproducing E. coli). phage-mediated transfer. • As described earlier for Shigella, the shiga toxin interrupts protein synthesis in its target cells. It seems to be responsible especially for the systemic effects of this infection. • .

• Another important virulence determinant for EHEC is the ability to efface (rub out or destroy) enterocytes, which are gut epithelial cells. The net effect is a lesion in the gut (effacement), usually in the large intestine. The microvilli are lost from the gut epithelium, and the lesions produce bloody diarrhea

Transmission and Epidemiology • The most common mode of transmission for EHEC is the ingestion of contaminated and undercooked beef, although other foods and beverages can be contaminated as well Bacterium is a natural inhabitant of the GI tracts of cattle. • The disease can also be spread via the fecal-oral route of transmission, especially among young children in group situations. • Even touching surfaces contaminated with cattle feces can cause disease, since ingesting as few as 10 organisms has been found to be sufficient to initiate this disease.

Culture and Diagnosis • Infection with this type of E. coli should be confirmed with stool culture or with ELISA or PCR.

Prevention and Treatment • The best prevention for this disease is never to eat raw or even rare hamburger. The shiga toxin is heat-labile and the E. coli is killed by heat as well. No vaccine exists for E. coli O 157: H 7. Antibiotics are contraindicated for this infection. • Even with severe disease manifestations, antibiotics have been found to be of no help, and they may increase the pathology. • Supportive therapy is the only option.

Other E. coli • At least four other categories of E. coli can cause diarrheal diseases. • Enterotoxigenic E. coli, • Enteroinvasive E. coli, • Enteropathogenic E. coli, • Enteroaggregative E. coli. • In clinical practice, most physicians are interested in differentiating shiga-toxin-producing E. coli (EHEC) from all the others.
 • The presentation varies depending on which type of E.")
Enterotoxigenic E. coli (ETEC) • The presentation varies depending on which type of E. coli is causing the disease. • Traveler’s diarrhea, characterized by watery diarrhea, low grade fever, nausea, and vomiting, is usually caused by enterotoxigenic E. coli (ETEC). These strains also cause a great deal of illness in infants in developing countries. • The bacterium is transmitted through the fecal-oral route or via contaminated vehicles or even fomites (such as a dirty glass).

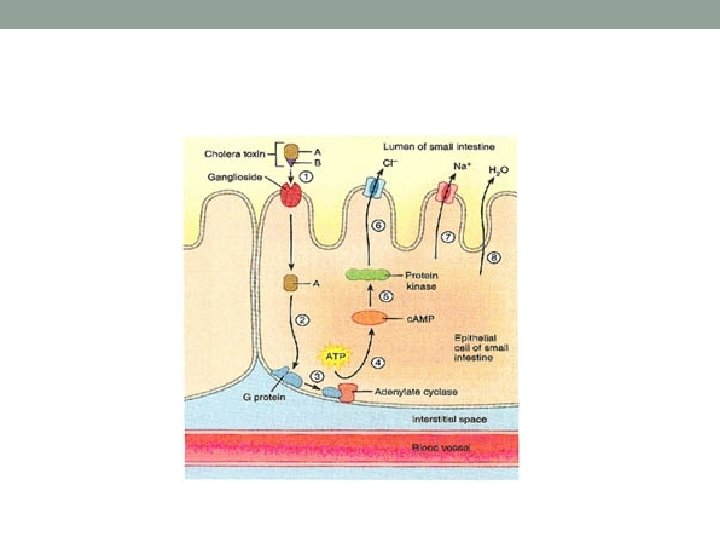
Travelers are susceptible to these strains because they are likely to be new to their immune systems. As the name suggests, the virulence of the bacterium derives from its ability to secrete two types of exotoxins that act on the enteric tract (enterotoxin). One toxin is a heat labile; A-B toxin, and it acts like the cholera toxin • Another toxin, actually a group of toxins, is heatstable. • These toxins are very small proteins that alter host cell function in order to cause large amounts of fluid secretion into the intestinal tract. The bacterium mainly affects the small intestine.

• Most infections with ETEC are self-limiting • They are treated only with fluid replacement • In infants, ETEC can be life-threatening, and fluid replacement is vital to survival
 • These strains cause a disease that is very similar")
Enteroinvasive E. coli (EIEC) • These strains cause a disease that is very similar to Shigella dysentery • The bacteria invade gut mucosa and cause widespread destruction • Blood and pus will be found in the stool • Significant fever is often present • EIEC does not produce the heat-labile or heat-stable exotoxins just described and does not have a shiga toxin, despite the clinical similarity to Shigella disease.

• EIEC does seem to have a protein that is expressed inside host cells, which leads to its destruction • Disease caused by this bacterium is more common in developing countries • It is transmitted primarily through contaminated food and water. Treatment is supportive (including rehydration)
 • These strains result in a profuse, watery diarrhea. Fever")
Enteropathogenic E. coli (EPEC) • These strains result in a profuse, watery diarrhea. Fever and vomiting are also common. • The EPEC bacteria are very similar to the EHEC E. coli described earlier—they produce effacement of gut surfaces • The important difference between EPEC and EHEC is that EPEC does not produce a shiga toxin and, therefore, does not produce the systemic symptoms characteristic of those bacteria

• Common infection in neonates. . Outbreaks in babies nurseries aged less 6 months. . watery diarrhea & vomiting. . Chronic diarrhea • Most disease is self-limiting • It can be life-threatening in young babies • Rehydration is the main treatment
 • These bacteria are most notable for their ability to")
Enteroaggregative E. coli (EAEC) • These bacteria are most notable for their ability to cause chronic diarrhea in young children and in AIDS patients. • EAEC are reported as the second most common cause of traveler's diarrhea, second only to Enterotoxigenic

Enterotoxins • Exotoxins that act on the small intestine • Massive secretion of fluids into intestinal lumen • Symptoms: vomiting and diarrhea • Produced by various bacteria 1. 2. 3. 4. 5. Staphylococcus aureus Clostridium perfringens Salmonella enteritidis Escherichia coli Vibrio cholerae

Campylobacter • Campylobacter is considered to be the most common bacterial cause of diarrhea in the United States • The symptoms of campylobacteriosis are frequent watery stools, fever, vomiting, headaches, and severe abdominal pain • The symptoms may last longer than most acute diarrheal episodes, sometimes extending beyond 2 weeks • They may subside and then recur over a period of weeks

• Campylobacter jejuni is the most common cause, although there are other Campylobacter species. • Campylobacters are slender, curved or spiral Gramnegative bacteria propelled by polar flagella at one or both poles • often appearing in S-shaped • These bacteria tend to be microaerophilic inhabitants of the intestinal tract, genitourinary tract, and oral cavity of humans and animals.

Transmission • Transmission of this pathogen takes place via the ingestion of contaminated beverages and food, especially water, milk, meat, and chicken. • Once ingested, C. jejuni cells reach the mucosa at the last segment of the small intestine (ileum) near its junction with the colon • They adhere, burrow through the mucus, and multiply


Pathogenesis • Symptoms commence after an incubation period of 1 to 7 days • The mechanisms of pathology appear to involve a heatlabile enterotoxin that stimulates a secretory diarrhea like that of cholera • In a small number of cases, infection with this bacterium can lead to a serious neuromuscular paralysis called Guillain-Barré
 is the leading cause of acute paralysis in the")
• Guillain-Barré syndrome (GBS) is the leading cause of acute paralysis in the United States since the eradication of polio there • Many patients recover completely from this paralysis • It seems to be an autoimmune reaction • The single most common precipitating event for the onset of GBS is. Campylobacter infection. • Twenty to forty percent of GBS cases are preceded by infection with Campylobacter

Diagnosis • Diagnosis of C. jejuni enteritis requires isolation of the bacterium from stool samples • Rapid diagnosis can be obtained from direct examination of feces with a dark-field microscope showing the characteristic curved rods and motility • This procedure is difficult to perform and not often used except in specialized labs

Management • Resolution of infection occurs in most instances with rehydration and electrolyte balance therapy. • In more severely affected patients, it may be necessary to administer erythromycin • Antibiotic resistance is growing in these bacteria. • Because vaccines are yet to be developed, prevention depends on rigid sanitary control of water and milk supplies and care in food preparation

Vibrio cholerae • Cholera has been a devastating disease for centuries • These days we have come to expect outbreaks of cholera to occur after natural disasters, war, or large refugee movements, especially in underdeveloped parts of the world.

Cholera around the world • 1892; German hygienist Max von Pettenkofer • In one specific case, Pettenkofer swallowed large dose of Vibrio cholerae bacteria from Robert Koch, the proponent of theory that the bacteria was the sole cause of the disease. He consumed it in a self-test in the presence of several witnesses on 7 October 1892. • He also took bicarbonate of soda to neutralise his stomach acid to counter a suggestion by Koch that the acid could kill the bacteria. • Pettenkofer suffered mild symptoms for nearly a week but claimed these were not associated with cholera. The modern view is that he did indeed have cholera, but was lucky to just have a mild case and he possibly had some immunity from a previous episode

• In February 1991, Peruvians saw a similar scene broadcast on their TV. • The president of the country and his wife were filmed eating raw fish and proclaiming it was safe to eat

• The bacterium's natural habitat and the main reservoirs of V. cholerae are people and brackish or saltwater • Vibrios are Gram negative comma-shaped rods with a single polar flagellum • They belong to the family Vibrionaceae. • Vibrio shares many cultural and physiological characteristics with members of the Enterobacteriaceae, a closely related family • They possess unique O and H antigens and membrane receptor antigens that provide some basis for classifying members of the family

• Only toxigenic strains of serogroups O 1 and O 139 have caused widespread epidemics and are reportable to the World Health Organization (WHO) as "cholera" • V. cholerae O 1 has two biotypes, Classical and El Tor (For the city in Egypt), and each biotype has two distinct serotypes, Inaba and Ogawa. The symptoms of infection are indistinguishable, although a higher proportion of persons infected with the El Tor biotype remains asymptomatic or have only a mild illness • In recent years, infections with the Classical biotype of Vibrio cholerae O 1 have become quite rare and are limited to parts of Bangladesh and India.

Signs and Symptoms • After an incubation period of a few hours to a few days, symptoms begin abruptly with vomiting, followed by copious watery feces called secretory diarrhea. The intestinal contents are lost very quickly, leaving only secreted fluids • This voided fluid contains flecks of mucus, hence the description “rice-water stool. ” • Fluid losses of nearly 1 liter per hour have been reported in severe cases • Untreated patient can lose up to 50% of body weight during the course of this disease • .

• The diarrhea causes loss of blood volume • Acidosis from bicarbonate loss, and potassium depletion, which manifest in muscle cramps, severe thirst, flaccid skin, sunken eyes, and in young children, coma and convulsions

• Secondary circulatory consequences can include hypotension, tachycardia, cyanosis, and collapse from shock within 18 to 24 hours. • If cholera is left untreated, death can occur in less than 48 hours, and the mortality rate approaches 55%.

Pathogenesis and Virulence Factors • At the junction of the duodenum and jejunum, the vibrios penetrate the mucus barrier using their flagella, • adhere to the microvilli of the epithelial cells, and multiply there • The bacteria never enter the host cells or invade the mucosa.

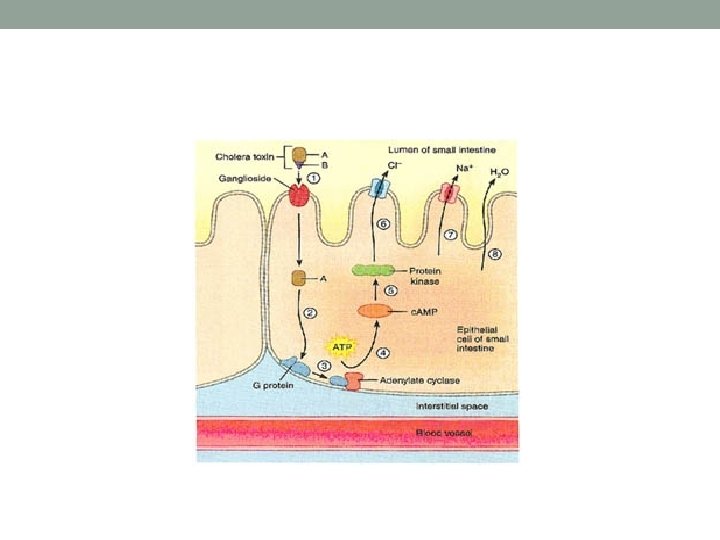
Virulence • The virulence of V. cholerae is due entirely to an enterotoxin called cholera toxin (CT), which disrupts the normal physiology of intestinal cells. It is a typical A-B type toxin When this toxin binds to specific intestinal receptors, a secondary signaling system is activated. Under the influence of this system, the cells shed large amounts of electrolytes into the intestine, an event accompanied by profuse water loss

Transmission and Epidemiology • Cholera ranks among the top seven causes of morbidity and mortality, affecting several million people in endemic regions of Asia and Africa. • In nonendemic areas such as the United States, the microbe is spread by water and food contaminated by asymptomatic carriers, but it is relatively uncommon.

Culture and Diagnosis • During epidemics of this disease, clinical evidence is usually sufficient to diagnose cholera. • V. cholerae can be readily isolated and identified in the laboratory from stool samples. • Direct dark-field microscopic observation reveals characteristic curved cells motility as confirmatory evidence. • Immobilization or fluorescent staining of feces with groupspecific antisera is supportive as well. • Difficult cases can be traced by detecting a rising antitoxin titer in the serum.

Prevention and Treatment • Effective prevention is contingent on proper sewage treatment and water purification • Detecting and treating carriers with mild or asymptomatic cholera are serious goals • Vaccines are available for travelers and people living in endemic regions. • One vaccine contains killed V. cholerae but protects for only 6 months or less • An oral vaccine containing live, attenuated bacteria was developed to be a more effective alternative, but evidence suggests it also confers only short-term immunity.

Treatment • The key to cholera therapy is prompt replacement of water and electrolytes, because their loss accounts for the severe morbidity and mortality • Cases in which the patient is unconscious or has complications from severe dehydration require intravenous replenishment as well • Oral antibiotics such as tetracycline and drugs such as trimethoprim-sulfamethoxazole can terminate the diarrhea in 48 hours. They also diminish the period of vibrio excretion

Gastritis and peptic ulcer • The curved cells of Helicobacter were first detected by J. Robin Warren in 1979 in stomach biopsies from ulcer patients. • He and an assistant, Barry J. Marshall, isolated the microbe in culture

Signs and Symptoms • Gastritis is experienced as sharp or burning pain emanating from the abdomen • Gastric ulcers are actual lesions in the mucosa of the stomach (gastric ulcers) or in the uppermost portion of the small intestine (duodenal ulcers). Both of these conditions are also called peptic ulcers • Severe ulcers can be accompanied by bloody stools, vomiting, or both • The second most common cancer in the world is stomach cancer and ample evidence suggests that long-term infection with H. pylori is a major contributing factor.

• Helicobacter pylori is a curved gram-negative rod, closely related to Campylobacter Previously called Campylobacter pylori

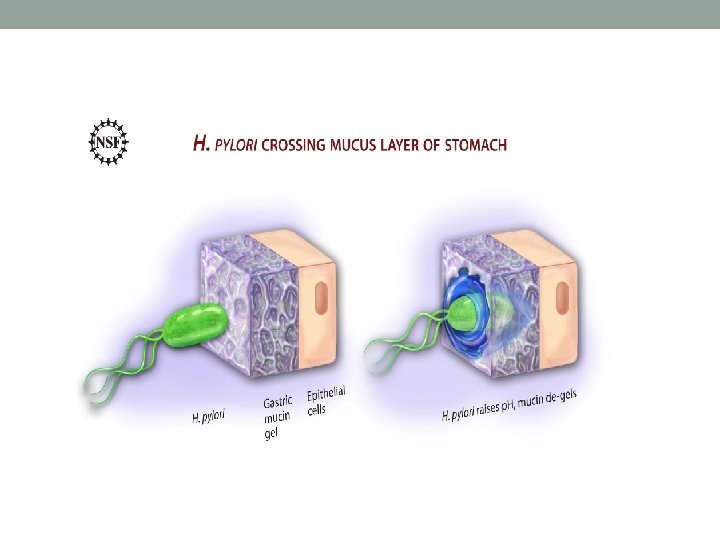
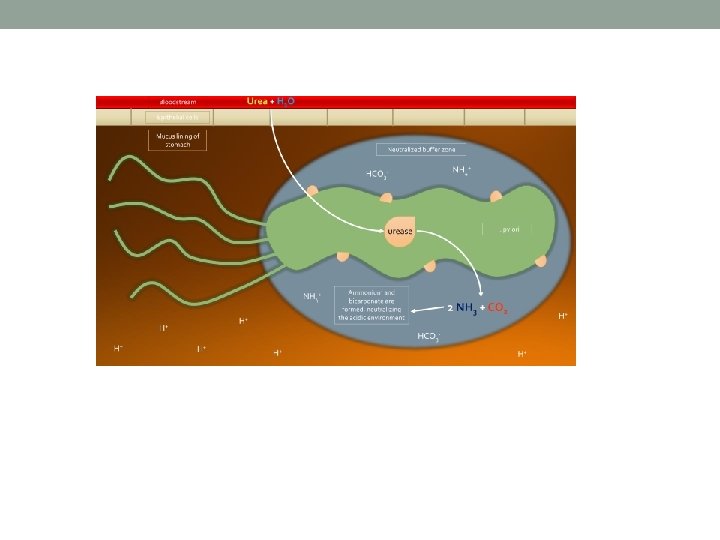
Pathogenesis and Virulence Factors • Once the bacterium passes into the gastrointestinal tract, it bores through the outermost mucous layer that lines the stomach epithelial tissue. Then it attaches to specific binding sites on the cells and entrenches itself. Another protective adaptation of the bacterium is the formation of urease, an enzyme that converts urea into ammonium alkaline compound that can neutralize stomach acid.

• As the immune system recognizes and attacks the pathogen, infiltrating white blood cells damage the epithelium to some degree, leading to chronic active gastritis • In some people, these lesions lead to deeper erosions and ulcers that can lay the groundwork for cancer to develop

Transmission and Epidemiology • The mode of transmission of this bacterium remains a mystery • Studies have revealed that the pathogen is present in a large proportion of the human population • It occurs in the stomachs of 25% of healthy middle-age adults and in more than 60% of adults over 60 years of age • H. pylori is probably transmitted from person to person by the oral-oral or fecal-oral route. • It seems to be acquired early in life and carried asymptomatically until its activities begin to damage the digestive mucosa.

Culture and Diagnosis • Diagnosis typically accomplished with endoscopy • The urea breath test is sometimes used • In this test, patients ingest urea that has a radioactive tag on its carbon molecule. • If Helicobacter is present in a patient’s stomach, the bacterium’s urease breaks down the urea and the patient exhales radioactively labeled carbon dioxide. • In the absence of urease, the intact urea molecule passes through the digestive system • A stool test is also available. The Hp. SA (H. pylori stool antigen test) is an ELISA format test

Prevention and Treatment • Triple therapy a one week or two weeks • Triple therapy for H pylori infection remains an option for first-line therapy in areas of low clarithromycin resistance (<15%) and consists of the following: • Proton pump inhibitor (PPI) (eg, omeprazole 20 mg BID, lansoprazole 30 mg BID, esomeprazole 40 mg QD, pantoprazole 40 mg QD, rabeprazole 20 mg BID) • plus • Clarithromycin 500 mg BID (first-line) or metronidazole 500 mg BID (when clarithromycin resistance is increasing) plus • Amoxicillin 1000 mg BID or metronidazole (if not already selected)
 • If a patient presents with severe nausea")
Acute Diarrhea with Vomiting (Food Poisoning) • If a patient presents with severe nausea and frequent vomiting accompanied by diarrhea, and reports that companions with whom he or she shared a recent meal (within the last 1 to 6 hours) are suffering the same fate, food poisoning should be suspected

• Food poisoning refers to symptoms in the gut that are caused by a preformed toxin of some sort. • In many cases, the toxin comes from Staphylococcus aureus. In others, the source of the toxin is Bacillus cereus or Clostridium perfringens • The toxin occasionally comes from nonmicrobial sources such as fish, shellfish, or mushrooms • In any case, if the symptoms are violent and the incubation period is very short, intoxication (the effects of a toxin) rather than infection should be considered

Staphylococcus aureus Exotoxin • This illness is associated with eating foods such as custards, sauces, cream pastries, processed meats, chicken salad, that have been contaminated by handling and then left unrefrigerated for a few hours. • Because of the high salt tolerance of S. aureus, even foods containing salt as a preservative are not exempt. The toxins produced by the multiplying bacteria do noticeably alter the food’s taste or smell. • The exotoxin is an enterotoxin is heat-stable; inactivation requires 100°C for at least 30 minutes. • Thus, heating the food after toxin production may not prevent disease.

• The ingested toxin acts upon the gastrointestinal epithelium and stimulates nerves, with acute symptoms of cramping, nausea, vomiting, and diarrhea. • Recovery is also rapid, usually within 24 hours. • The disease is not transmissible person to person. Often, a single source will contaminate several people, leading to a mini-outbreak (Common source outbreak)

• This condition is almost always self-limiting, and antibiotics are definitely not warranted

Other Kinds of Food Poisoning • Bacillus cereus secretes a toxin that acts as an emetic and induces vomiting • Clostridium perfringens produces an enterotoxin which is released during sporulation and is produced under anaerobic conditions, as when undercooked meats and gravies are kept warm • Clostridium botulinum is acquired when toxin- contaminated food is eaten. The toxin is a neurotoxin and impairs muscle contraction

• Bacillus cereus. . G+ve Aerobic Spore-Forming Bacilli . . Common in Nature. . Spores survive boiling and cooling in Food. . Various Enterotoxins produced during bacilli sporulation either in Food or Intestine. . Associated with two main gastrointestinal symptoms. • 1 -Intoxication. . Heat-stable Emetic Enterotoxins . . Typically developed within 24 hours of eating contaminated fried rice. . Meat. . last for few hours without diarrhea and fever. • 2 - Diarrheal Toxins. . watery mild diarrhea. . No Fever or Vomiting. • 3 - Both Types of toxins may produce by certain B. cereus strains. . Mostly outbreaks in family, schools. . Commonly associated with Chinese food. . fried Rice

Bacillus cereus Exotoxin • Bacillus cereus is a sporulating Gram-positive bacterium that is naturally present in soil. • As a result, it is a common resident on vegetables and other products in close contact with soil • It produces two exotoxins, one of which causes a diarrheal-type disease, the other of which causes an emetic disease • The type of disease that takes place is influenced by the type of food that is contaminated by the bacterium

• The emetic form is most frequently linked to fried rice, especially when it has been cooked and kept warm for long periods of time These conditions are apparently ideal for the expression of the low-molecular-weight, heat-stable exotoxin having an emetic effect. The diarrheal form of the disease is usually associated with cooked meats or vegetables that are held at a warm temperature for long periods of time. These conditions apparently favor the production of the high-molecularweight, heat- labile exotoxin. The symptom in these cases is a watery, profuse diarrhea that lasts only for about 24 hours.

• Diagnosis of the emetic form of the disease is accomplished by finding the bacterium in the implicated food source • Microscopic examination of stool samples is used to diagnose the diarrheal form of the disease • In every day practice, neither diagnosis nor treatment is performed because of the short duration of the disease • In both cases, the only prevention is the proper handling of food

Clostridium perfringens • Clostridium perfringens. . G+ve Anaerobic Spore- Forming. . Widely distributed in the environment. . Common Intestines of humans and animals. . Produce Various Enterotoxins, Cytotoxins, Enzymes • C. perfringens toxin-type A. . Food-poisoning. . Incubation Period. . 8 -24 Hrs. . Diarrhea. . Nausea. . Abdominal Pain. . Vomiting. . No Fever. . Mostly Selflimited. . 1 -2 Days. . No Antibiotic treatment • C. perfringens toxin-Type C. . Released following multiplication in intestine. . Sever Diarrhea. . No vomiting. . Necrotizing Enteritis. . Rare Sepsis. . Can be fatal in certain Conditions. . Antibiotic treatment • Detection toxin in blood. . Food specimens.

Clostridium perfringens Exotoxin • Another sporulating gram-positive bacterium that causes intestinal symptoms is Clostridium perfringens Endospores from C. perfringens can also contaminate many kinds of foods Those most frequently implicated in disease are animal flesh (meat, fish) and vegetables such as beans that have not been cooked thoroughly enough to destroy endospores When these foods are cooled, spores germinate, and the germinated cells multiply, especially if the food is left unrefrigerated. The clostridium perfringens enterotoxin(CPE) mediating the disease is heat-labile (inactivated at 74 °C (165 °F)). It can be detected in contaminated food (if not heated properly), and feces

• If the food is eaten without adequate reheating, live C. perfringens cells enter the small intestine and release exotoxin • The toxin, acting upon epithelial cells, initiates acute abdominal pain, diarrhea, and nausea in 8 to 16 hours. Recovery is rapid, and deaths are extremely rare. • C. perfringens also causes an enterocolitis infection similar to that caused by C. difficile. This infectious type of diarrhea is acquired from contaminated food, or it may be transmissible by inanimate objects

Botulism • It caused by Clostridium botulinum; G+ve Anaerobic Spore-Forming • Acquired when toxin contaminated food is eaten • The toxin is a neurotoxin • Incubation 1 -24 h • Consumption improperly or inadequately processed canned food. . Spores. . Vegetative cells. . Release highly potent heat-stable neurotoxin ( A-G types). . inactivation 30 min boiling.

• Botulinum toxin binds to presynaptic nerve ending of peripheral nervous system & cranial nerves. . • Inhibits acetylcholine release. . Flaccid paralysis, Respiratory or Cardiac failure. . Death. . Early Specific Antitoxin Treatment may help. . No Antibiotics
. .")
Clostridium difficle • Anaerobic, spore-forming Gram+ve; Part of normal intestinal flora (5 -20%). . Rapidly increased and become danger following antibiotic treatment for more than 1 week. . with all wide-spectrum penicilins. . clindamycin cephalosporins. . Often among hospitalized patients. . Compromised. . Antibiotic-associated enterocolitis . . nosocomial infection. • Produce two exotoxins types A, B. . Bloody diarrhea. . Pseudomembranous colitis. . Discontinue potential causative antibiotics. . use oral metronidazole or vancomycin. . to stop disease complication.
- Slides: 102