Autonomic nervous pharmacology 2 Acetylcholine v Has little














 v. Urinary retention (Bethanechol) v. Glaucoma")




 v Treatment of MG (Pyridostigmine)")
 v. Autoimmune (autoantibodies to NM in NMJ) v. Reduction in receptor")

")
 v")

")


 compounds. v. Irreversibly inhibit CE. v. Covalent bond")
 v OP compound. v Irreversibly inhibits CE. v Insecticide. v Toxicity: excessive")
.")



- Slides: 40
Autonomic nervous pharmacology 2
Acetylcholine v. Has little therapeutic value. v. Has multiple actions. v. Has short t ½ v. Activates muscarinic & nicotinic receptors. 12/5/2020 2
Pharmacodynamics of Ach q. Muscarinic stimulation: v. On the CVS: Ø-ve chronotropic & inotropic effects. ØDecrease stroke volume & cardiac output. ØDecrease ABP: ØStimulation of vascular M 3 receptors ØIncrease NO release from endothelium 12/5/2020 3
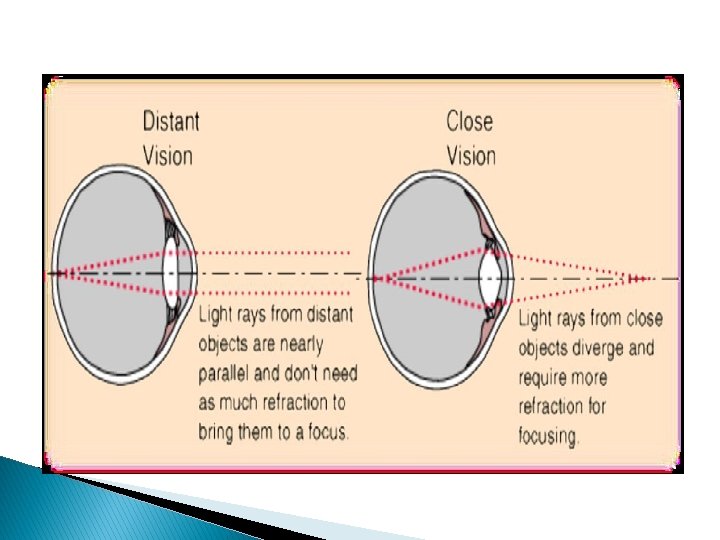
Pharmacodynamics of Ach v. Eye: ØMiosis: ØContraction of circular muscle of iris. ØAccommodation to near vision: ØContraction of ciliary muscle of the eye ØDecrease IOP( intra-occular pressure) 12/5/2020 4
Pharmacodynamics of Ach v. Exocrine glands & GI secretion: ØIncrease secretion. v. Contraction of intestinal wall & relaxation of sphincters: ØDefecation v. Contraction of bladder wall & relaxation of sphincter: ØUrination 12/5/2020 5
Pharmacodynamics of Ach v. Bronchi: ØBronchoconstriction. ØIncrease mucosal secretion. v. Penile erection: ØIncrease release of nitric oxide. 12/5/2020 6
Pharmacodynamics of Ach q. Nicotinic receptor stimulation: v. Autonomic ganglia: ØStimulation v. Adrenal medulla: ØIncrease noradrenaline & adrenaline secretion v. NM Junction transmission: ØMuscle contraction 12/5/2020 7
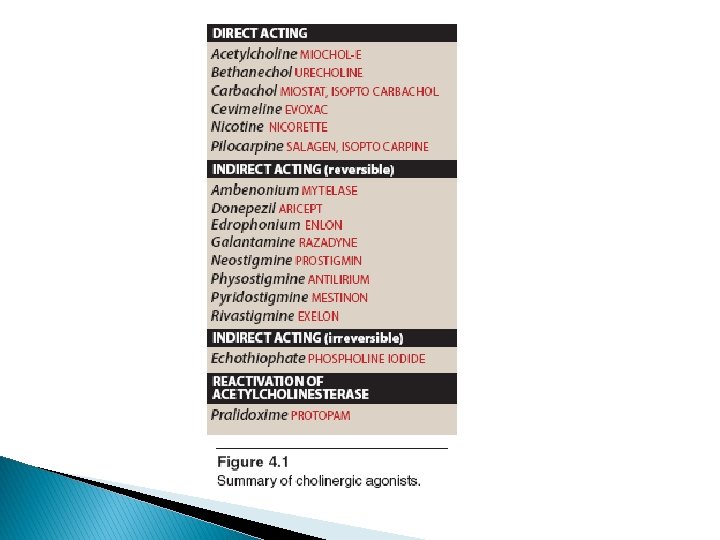
Cholinomimetics q. Mimic or simulate actions of Ach: v. Direct-acting. v. Indirect-acting. 12/5/2020 8
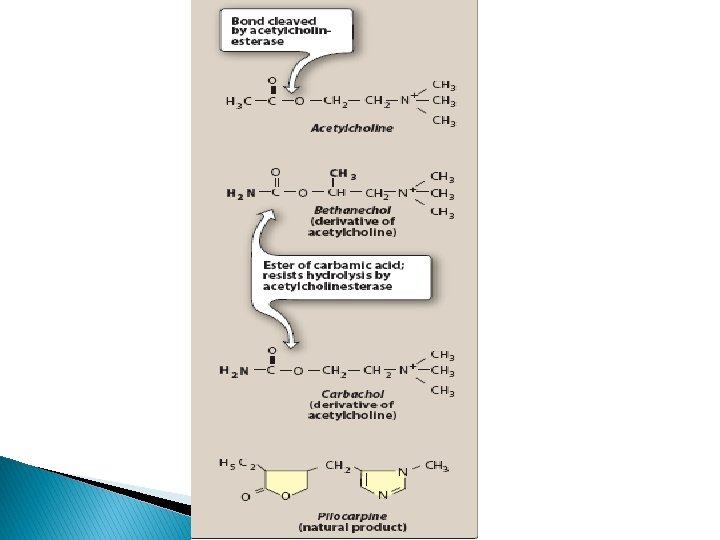
Direct acting cholinomimetics v. Activate directly cholinergic receptors: v. Choline esters: ØBethanechol, Carbachol, Methacholine. üResist degradation by cholinesterases. üHave longer duration of action than Ach. v. Natural alkaloid: ØPilocarpine. üActs directly on end organs like the eye. 12/5/2020 10
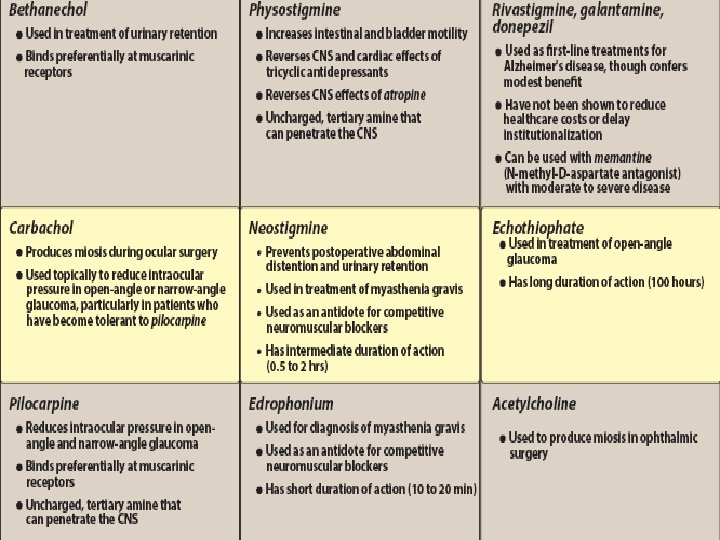
Bethanechol v. Derivative of Ach v. Has: ØLittle nicotinic effects ØGood muscarinic effects on bladder & GIT v. Leads to easy urination & defecation v. Used to treat post-operative or post-labour: ØUrinary retention or Øparalytic ileus: the weakness of intestine to push its content causing constipation because of weak peristaltic activity 12/5/2020 13
Carbachol v. Derivative of Ach v. Has muscarinic & nicotinic actions v. Limited use: ØBecause of nicotinic effects on ganglia & adrenal medulla v. Used mainly topically as miotic in glaucoma to decrease high intraocular pressure (IOP) 12/5/2020 14
Pilocarpine v. Natural plant alkaloid v. Resistant to CE enzyme v. It produces: ØMiosis (contraction of circular muscle of iris) ØContraction of ciliary muscle of the eye ØReduction of IOP v. Used topically in glaucoma 12/5/2020 15
Pilocarpine v. Lowers high IOP in close-angle & open angle chronic glaucoma v. Improves outflow of aqueous humour: ØOpens fluid pathway ØIncrease aqueous flow through canal of Schlemm ØSecondary to contraction of circular muscle of the iris & ciliary muscle v. Stimulates sweating, lacrimation, salivation 12/5/2020 16
12/5/2020 17
Indications of direct cholinomimetics v. Paralytic ileus (Bethanechol) v. Urinary retention (Bethanechol) v. Glaucoma (Pilocarpine & Carbachol topically v. Xerostomia (dry mouth) of Sjogren’s syndrome (oral pilocarpine) 12/5/2020 19
Adverse effects of direct cholinomimetics v. Excessive sweating, salivation v. Flushing, hypotension v. Abdominal colic & diarrhoea v. Bronchospasm v. Pilocarpine: ØImpaired accommodation to far vision & darkness 12/5/2020 21
Contraindications of cholinomimetics v Bronchial asthma v Peptic ulcer 12/5/2020 22
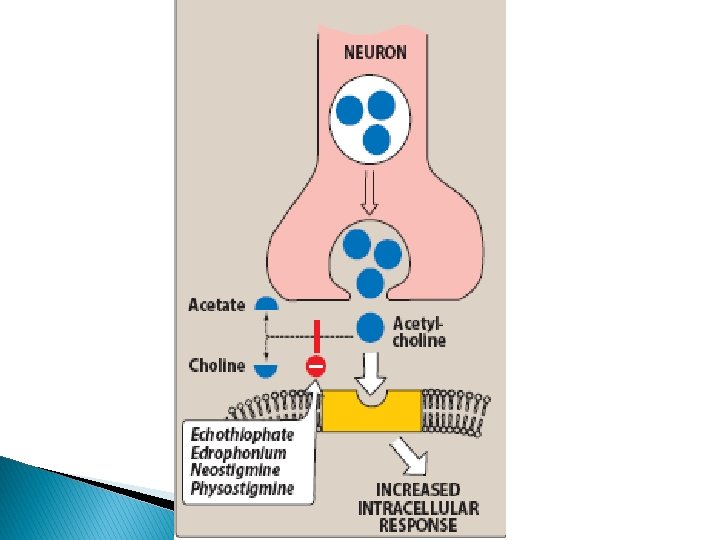
Cholinesterase enzymes v CE is a protein ØIn cholinergic synapses & RBC ØMetabolizes Ach into choline & acetate ØSpecific for Ach in cholinergic synapses v Pseudocholinesterase in plasma & liver ØNot specific to Ach ØMetabolizes other drugs (suxamethonium, procaine) 23
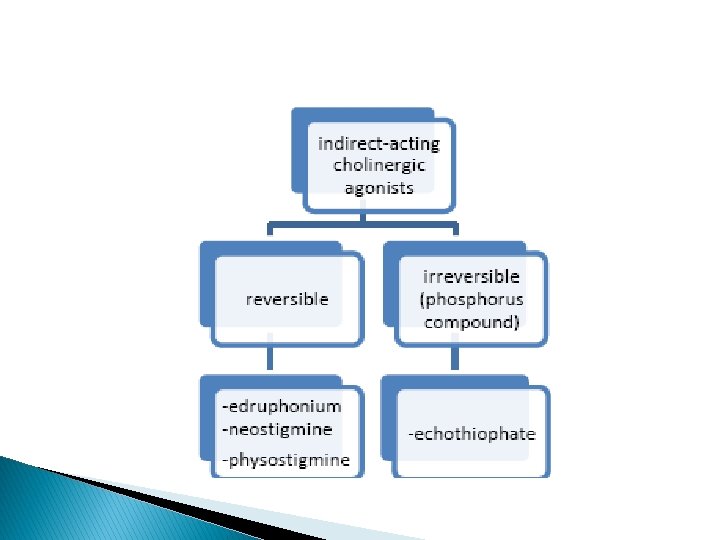
Classification of indirect-acting cholinomimetics Classified into: v Reversible cholinesterase inhibitors v Irreversible cholinesterase inhibitors 24
Uses of indirect-acting cholinomimetics v Diagnosis of MG (Edrophonium) v Treatment of MG (Pyridostigmine) v Reversible NMB intoxication (Neostigmine) v Alzheimer’s disease (Donepezil) v Irreversible CEI: insecticides 25
Myasthenia gravis (MG) v. Autoimmune (autoantibodies to NM in NMJ) v. Reduction in receptor number v. Muscle weakness, fatigability, , difficult speaking & swallowing v. Treatment: ØReversible CEI ØThymectomy ØImmunosuppressant 27
Reversible Ch. E inhibitors v Inhibit reversibly CE enzyme v Accumulation of Ach v Electrostatic bonds v Stimulate nicotinic & muscarinic receptors v Useful in myasthenia gravis 28
Neostigmine v. Synthetic CEI, does not cross BBB v. Duration of action (4 hrs) v. Mainly in MG & also in: ØAntidote to competitive NM blocker tubocurarine poisoning ØParalytic ileus, urinary retention v. Given orally, SC 29
Pyridostigmine v Similar to neostigmine v Has longer duration of action (6 hrs) v Useful orally in myasthenia gravis 30
Cholinergic Crisis: �Over-stimulating of nicotinic receptors can cause muscle weakness and paralysis by the excessive intake of Anticholinesterases which are (indirect drugs) �Over-stimulation of nicotinic receptors will lead to its blockage instead of further activation. �Cholinergic crisis can happen to myasthenia gravis patients who are overdosing on anticholinesterases drugs.
Edrophonium v. Similar to neostigmine v. IV, short duration of action (10 -20 min) v. Useful in diagnosis of MG v. To differentiate between weakness due to myasthenic crisis or cholinergic crisis: ØMyasthenic crisis ØCholinergic crisis 32 improvement aggravated
Adverse effects of CEI v. Excessive salivation v. Flushing and hypotension v. Abdominal colic and diarrhoea v. Bronchospasm 33
CEI useful in Alzheimer’s disease v Tacrine q. Reversible CEI used in treatment of Alzheimer’s disease; qhepatotoxic v Donepezil ØNew selective CEI ØOnce daily ØLacks hepatoxicity of tacrine ØUseful in Alzheimer’s disease 34
Irreversible CE Inhibitors v. Organophosphorous (OP) compounds. v. Irreversibly inhibit CE. v. Covalent bond in Enzyme-inhibitor complex. v. Used as insecticides: ØParathion, malathion v. As nerve gases in chemical warfare: ØTabun, Sarin, Soman 35
Isoflurophate (DFP) v OP compound. v Irreversibly inhibits CE. v Insecticide. v Toxicity: excessive cholinergic stimulation. v May be used topically in glaucoma. v Duration of action about a week. 36
Echothiophate v. New agent. v. Similar to isoflurophate. v. Long duration of action (week). 37
Differences between direct & indirect-acting cholinomimrtics v. Actions on receptors: ØDirect ØIndirect v. Pharmacodynamic effects: ØSimilar v. Central effects with indirect: ØCross BBB 38
Organophosphorous Insecticide Poisoning v Agricultural or industrial accidents v Excessive cholinergic manifestations v GIT (diarrhoea, colic) v Respiratory (dyspnoea, bronchospam) v CV (bradycardia, hypotension) v Micturition, excessive sweating, M. paralysis v Miosis (pin-point pupil), convulsions & death 39
Treatment of OPI Poisoning v General measures. v High doses atropine IV or IM. v Mechanical ventilation. v Diazepam for convulsions. v Enzyme reactivation by pralidoxime IM. 40