Autoimmune bullous dermatosis Prof Dr Wafaa Abdallah These

Autoimmune bullous dermatosis Prof. Dr. Wafaa Abdallah

� These diseases are characterized by pathogenic auto antibodies directed at target antigens. The target antigens are components of desmosomes or basement membrane zone.
.")
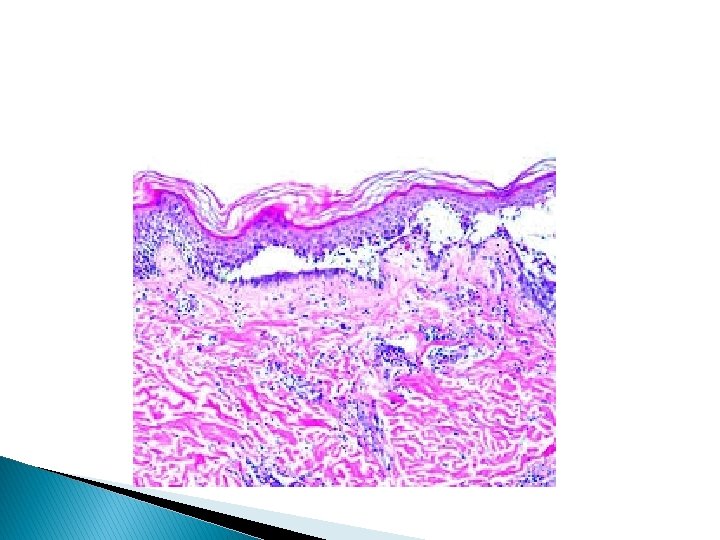
I- PEMPHIGUS family � This name is derived from the Greek word pemphix (blister). � The auto antibodies in this disease react with intercellular adhesion molecules. The immunoreactants are deposited between keratinocytes. The intercellular bridges disappear and keratinocytes separate. This is acantholysis.

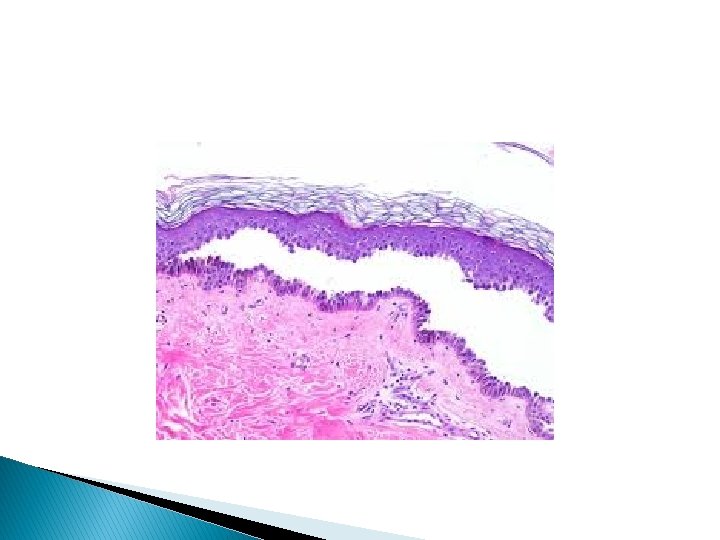
Pemphigus vulgaris � This is the commonest of the pemphigus family. Pathology � The earliest lesion is suprabasal acantholysis. This is followed by spongiosis.

Immunofluorescence � Direct immunofluorescence shows immunoglobulin deposited on surface of keratinocytes. � Indirect immunofluorescence over 80% of patients have circulating PV auto antibodies.

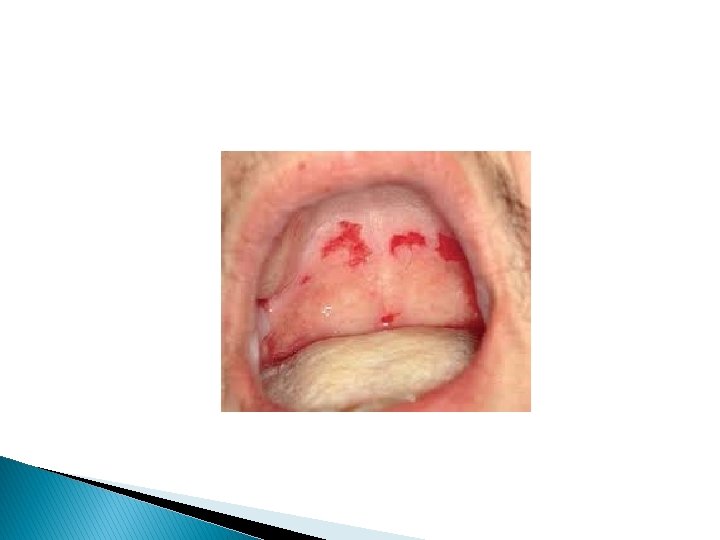
Clinical picture � There may be some constitutional symptoms, as fever, malaise, latitude and arthralgia along the course of disease. � Almost all patients have mucosal lesions. They may be the presenting symptoms specially in mouth or may be the only manifestation. � In the mouth intact bullae are rare but there are erosions (buccal or palatal) which are slow to heal. � Other mucosal surfaces may be involved as conjunctive, nasal, pharynx, larynx, oesophagus, urethra, vulva and cervix.

Cutaneous lesions � Most patients develop localized or generalized cutaneous lesions in the form of flaccid bullae between which there is apparently normal skin. Firm sliding pressure with a finger will lead to an erosion due to separation of normal looking epidermis from demis. (+ve Nikolysky's sign). � The bullae will rupture leading to erosions which will heal slowly with no scarring. Pigmentary changes may occur. morbidity and mortality are related to disease activity.



Differential diagnosis � From other bullous dermatosis.

Other pemphigus types Pemphigus vegetans � There are vegetating granulations in flexures. Pemphugis foliaceus � There are crusted lesions surrounded by erythema. Pemphigus erythematosus � It has a resemblance to lupus erythematosis. Others

Treatment of pemphigus � Prednisolone with an adjuvant is the preferred treatment for P. V. Dose � 1. 0 – 1. 5 mg/kg/day can usually control disease. � The dose should be titrated to chemical response.

Adjuvant therapies � Include: azathioprine, cyclophosphamide, methotrexate and dapsone. � In other mentioned types of pemphigus treatment is more or less the same as PV except when localized where patients may not need systemic therapy. � Patients treated by systemic steroids are liable to all complications of steroids as hypertension, glucose intolerance and others. � They should be carefully monitored.

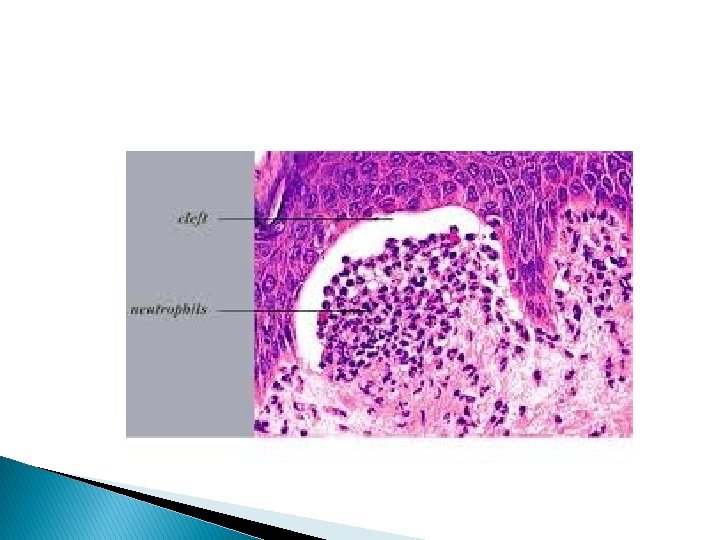
Dermatitis herpetiformis � This is a rare intensily pruritic chronic symmetrical recurrent polymorphic eruption consisting of papules, wheals, vesicles and bullae and excortiatons. � Gluten (protein found in cereal) provokes flares of the disease. � Histopathology bullae are subepidermal, neutrophils and eosinophils accumulate within dermal papillae forming microabcesses

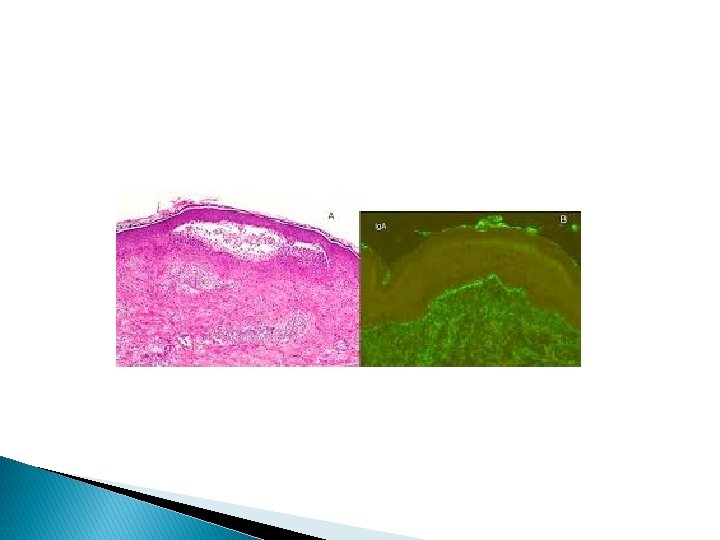

Direct IF � Positive showing granular deposits of Ig. A in dermal papillae. Indirect IF � Is –ve for basement membrane zone BMZ or dermal auto antibodies. D. D. � Scabies, papular urticaria, other pruritic disease.

Treatment � Dapsone in a dose of 100 – 200 mg/day. � Alternatives include sulfapyridine. � Gluten free diet may help in discontinuation of drug.
 � This disease seems to have an immunologic pathogenesis.")
III- Miscellaneous Erythema multiforme (EM) � This disease seems to have an immunologic pathogenesis. � clinically EM involves. ◦ ◦ ◦ Macular Popular Or urticarial lesions. As well as classic iris or target lesions. Lesions may involve the palms or trunk as well as oral and genital lesions.

EM simplex � Macules and papules or urticarial wheals and target lesions. � Having an acral distribution. � Target lesions: Have 3 zones, a central dusky erythema, middle paler zone of oedema and outer zone of erythema with a well defined edge. � Occasionally bullae or erosions may be on mucous membranes.

Treatment � in minor forms symptomatic treatment � In major forms systemic steroids 30 – 60 mg/kg decreasing over 1 – 4 weeks. � Good nursing in dermatologic intensive care unit and ophthalmologic help.

Steven Johnson syndrome and toxic epidermal necrolysis � They seem to have an immunologic pathogenesis.
 � This is a severe illness")
clinical features of Steven Johnson syndrome (SJ syndrome) � This is a severe illness with marked constitutional symptoms. (high fever, myalgia, arthralgia and extensive EM of trunk) � Significant involvement of mucous membrane with extensive bullae and crustations. Occasional blisters and lesions cover less than 10% of surface area. � Eye changes � Include conjunctivitis, corneal ulceration, anterior uveitis and panophthalmitis.
 � This should be differentiated from SI syndrome. There are")
Toxic epidermal necrolysis (TEN) � This should be differentiated from SI syndrome. There are typical sheet like lesions involve more than 30% of body surface with wide spread, pruritic macules and atypical target lesion. There is severe involvement of mucous membranes. � SJS may evolve into TEN � Complications are similar to those of extensive burns.


DD � SSSS, and other bullous dermatosis. Treatment � It is a life threatening disease. � Suspected drug should by stopped. � Care as extensive burn. � Use of high dose systemic steroid is controversial.
- Slides: 31