Audit of Sepsis Management and Outcomes of ED




 Gender, No(%)")
 60% 57% 46% 44% 40% 33%")


 no empiric antibiotics given by ED staff • 2 cardiopulmonary")
")
 in 2015 Single (n=40) Mixed by")
 in 2014 Single (n=29) Mixed by 2 (n=1) Gram +ve")


 7/45 (15. 6%) Discharge")






- Slides: 23
Audit of Sepsis Management and Outcomes of ED in a Tertiary Hospital G Chan 1, E Kidney 2, L Morrisey 2, A Ronayne 1, M Kelleher 1, U Kennedy 2, B Boyle 1 Department of Clinical Microbiology 1 and Emergency Department 2 03/10/2015
Methods • Retrospective audit of patients who attended ED of SJH with significant positive blood culture(SPBC) • 1 st Jan-30 May 2014 and 2015 • SJH ethical approval • Review of ED patient records, Microbiology Telepath System, EPR system • Data collection and analysis with Microsoft Excel: – SIRS criteria, Sepsis 6, time for medical review, antimicrobial choice, microbiology advice, adherence to antimicrobial guidelines, susceptibility data, 30 -day mortality and length of stay
Aims AIMS • To audit the compliance of sepsis management in ED of those with significant blood stream infection over a 5 -month period of consecutive 2 years • To audit the compliance of empirical antimicrobial guidelines and the antimicrobial choice in those presenting to ED with significant positive bloodstream infection (SPBC) • To review the bed day cost for SPBC infections presenting to ED
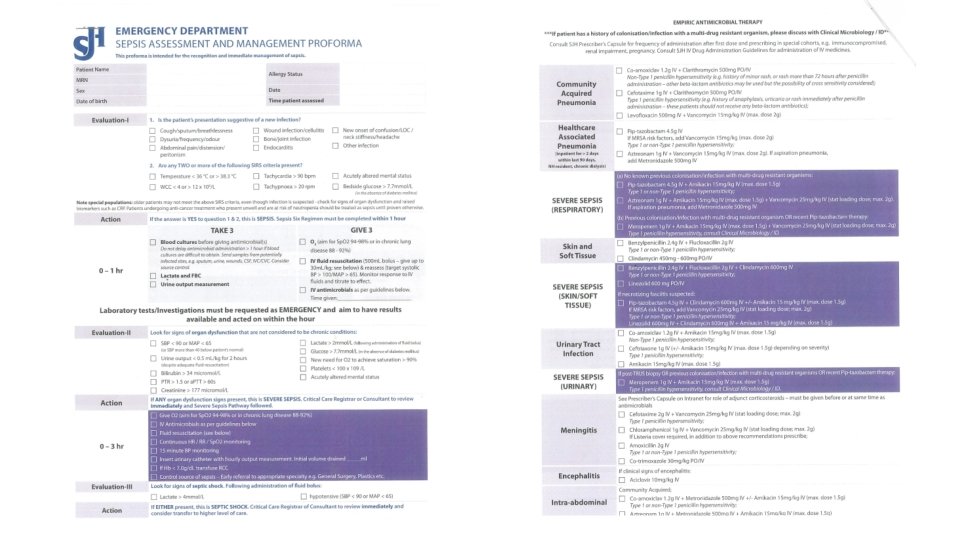
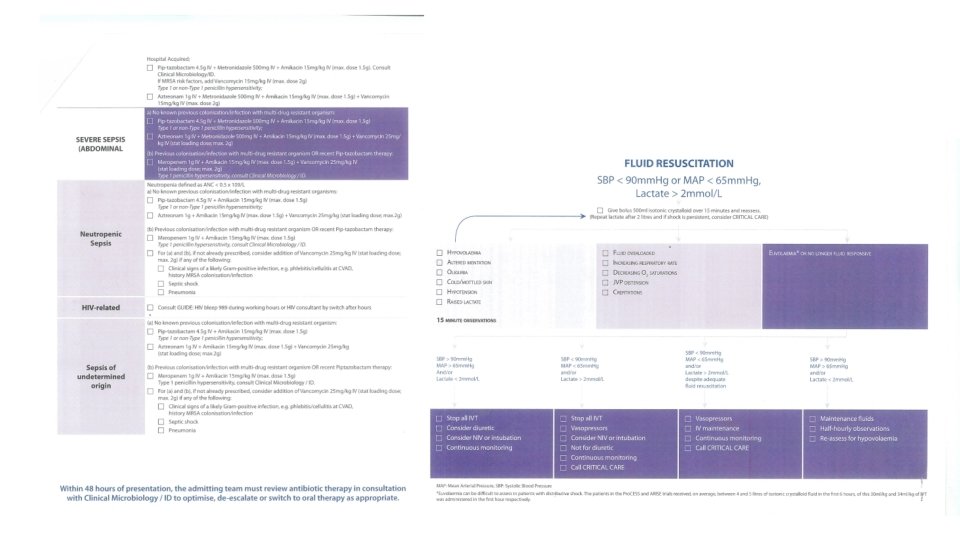
Audit standards • Surviving Sepsis Guidelines • Sepsis 6 bundle to be performed within 1 hour once diagnosis of sepsis is made • Hospital antimicrobial guidelines Sepsis Management National Clinical Guideline No. 6
Results Year 2014, n=30 No of significant positive 30 blood culture (SPBC) Gender, No(%) of male 20 (66. 7%) Age, mean(range), years 64 (31 -94) 48% ICU admission, No(%) 3 (10%) Year 2015, n=45 45 26 (57. 8%) 63 (24 -96) 64% 9 (20%)
Sepsis 6 Components Performed Within 1 hour (SPBC) 60% 57% 46% 44% 40% 33% 30% 26% 20% 30% 28% 15% 10% 13% 7% 7% 4% 4% 0% FBC Blood culture Lactate Urine output measured 2014 2015 O 2 prescription IV fluids IV antibiotics
2014 Mean time to medical review, hours 2: 36 SIRS≥ 2 Severe sepsis Mean time to antibiotics, hours 5: 00 SIRS≥ 2 Severe sepsis Mean time to micro advice, hours 2015 1: 20 1: 12 1: 10 3: 05 3: 09 2: 34 23: 28
Source of Infection 50% 43% 45% 40% 35% 30% 27% 25% 20% 15% 18% 17% 18% 15% 11% 10% 7% 5% 4% 3% 2% 3% 0% Respiratory Urinary IA Cr. BSI 2014 SSTI 2015 Endovascular ENT Unknown
SPBC 2015 5/45 (11%) no empiric antibiotics given by ED staff • 2 cardiopulmonary arrest: 1 resp sepsis, 1 SBP • SIRS≥ 2: 1 IE 1 SSTI 1 unknown source 8/45 (17. 8%) had source control • 2 Surgical drainage of abscess • 1 Nephrostomy • 3 ERCP and biliary stenting • 1 Cholecystectomy • 1 Drainage of empyema
2015 • • • Suitable for IV to PO switch in 21/45 ( 47%) 16/21 (76%) had PO switch 22 HCA (49%), NHCA 23/45 (51%) 3 vaccine preventable 1 alcohol associated (SBP) 11/45 (24%) IVDU 4 IE, 1 septic emboli, 1 dental abscess, 1 empyema, 2 SSTI, 1 respsepsis/cardiac arrest, 1 unknown
Pantoea agglomerans; 1 Number of Isolates ( n=50) in 2015 Single (n=40) Mixed by 2 (n=5) Gram +ve (n=29) 58% Gram –ve ( n= 21) 42% Pseudomonas aeruginosa; 1 Morganella morganni; 2 fully sensitive Clostridum perfringens; 1 Enteroccocus faecium; 1 Vanc s Enteroccocus faecalis; 2 1 ESBL, given piptaz as empiric 3 Cipro r 3 Coamox r, 2 given coamox 4 Coamox i 1 Piptaz r , given piptaz 1 Gent i Escherichia Coli; 15 Amox s Streptococcus pneumoniae; 3 1 Pen i (mic 0. 5) 2 Pen s Streptococcus mitis/oralis; 1 Streptococus infantarius; 1 Klebsiella oxytoca; 1 Streptococcus anginosus; 2 Amox resistant Klebsiella pneumoniae; 1 Granulicatella adiacens; 1 1 MRSA Streptococcus dysgalactiae; 2 Staphylococcus aureus; 13 Streptoccucus salivarius; 1 Abiotrophia defectiva; 1 Pen r
No of Isolates (n=31) in 2014 Single (n=29) Mixed by 2 (n=1) Gram +ve (n=6) 19% Gram –ve (n=25) 81% Klebsiella oxytoca; 1 Staphyloccocus aureus; 6 No MRSA Proteus mirabilis; 1 Enterobacter aerogenes; 2 Piptaz I , given Enterobacter cloacae; 1 Gent s Escherichia Coli; 18 Serratia marcescens; 1 Gent s, given piptaz Pseudomonas aeruginosa; 1
The Empirical and Adjusted Antimicrobial choice in Audit Period of 2015 Piperacillin-tazobactam Meropenem Aztreonam Daptomycin Vancomycin Clarithromycin Metronidazole Gentamicin Flucloxacillin Fluoroquinolone Penicillin Coamoxiclav Amoxicillin Cephalosporin 4 6 0 1 1 1 2 3 0 5 3 1 4 0 4 1 0 3 3 5 5 5 4 9 2 2 0 25 Targeted tx 4 5 10 Empiric tx 15 20 25
Antimicrobial Choice in 2014/2015 Empirical Tx 2015 2014 Antimicrobial guidelines compliance • Partial compliance • Full compliance Appropriate antibiotic use according to susceptibility data * 28/45 62% 11 (24%) 17 (38%) 93% • Mortality group (n=7)** 6/7 (71%) Targeted Tx 2015 Targeted Tx 2014 52% 73% 100% 2/3 (66%) 100% • *Excluding 2 without sensitivity profile and 2 not given empiric antibiotics prior to blood culture results • ** 1 out of hospital cardiac arrest not given empiric antibiotics. Ecoli BSI and SBP which is piptaz sensitive
Outcome 2015 2014 P value 30 -day mortality, No (%) 7/45 (15. 6%) Discharge by 30 day(%) 35/45 (78%) Mean length of stay, days 23 (1 -132) 3/30 (10%) 22/30 (73%) 21 (1 -72) NS NS NS Total length of stay ICU admission, No(%) ICU mortality, No (%) 628 3/30 (10%) 1/3 (33%) NS NS 1054 9/45 (20%) 2/9( 22%) • In 2015, discharge summary done in 30/45 (67%), of these, 27/30 (90%) had sepsis/infection as diagnosis • 15/45 (33%) with no discharge summary : 1 current inpatient, 2 AMA, 7 RIP, 5/15 (33%) discharged without letter
Review of Bed Day Cost of SPBC Two 5 - Month Period 2014/2015 Mean LOS 2014 Bed day Cost 20 days € 402, 240 Mean LOS 2015 Total ICU stay Non-ICU stay Total Days 23 days 62 days 992 days 1054 days ICU cost (per day € 3500) AMAU cost (per day € 356) Total 2015 Total for 10 month Estimate for 12 months € 217, 000 € 353, 152 € 570152 € 972, 392 1 - 1. 3 million euro in bed days costs alone
Summary • Improvement of time to medical review and time to antibiotics • Suboptimal Sepsis 6 Bundle adherence • Suboptimal compliance of empirical antimicrobial guidelines (62%) and de-escalation therapy • Suboptimal sepsis coding on discharge
“ I would challenge you to a battle of wits but I see you are unarmed” Challenges Future considerations : • Sepsis ED proforma • Sepsis call • National audit programme • Sepsis online elearning • IVDU cohort interventions Change Resources Integration Beyond Life without struggle is a life without success!
Aims Conclusion • Early recognition of sepsis and prompt intervention is prudent as sepsis is a time-dependent emergency • Importance of appropriate antimicrobial use for infections according to local prescribing guidelines
Acknowledgements • Microbiology Department, SJH • Emergency Department, SJH
Sepsis 6 Components Performed Within 1 hour 70% 60% 57% 59% 53% 50% 46% 38% 40% 28% 30% 31% 38% 33% 30% 19% 20% 13% 10% 7% 3% 0% FBC Blood culture Lactate Urine output measured 2015 O 2 prescription 2015 Severe Sepsis IV fluids IV antibiotics