Atrial Fibrillation Update in ED Management Susan P

Atrial Fibrillation: Update in ED Management Susan P Torrey, MD, FAAEM, FACEP Associate Professor of Emergency Medicine Tufts University School of Medicine

I have no financial disclosures but… www. Torrey. EKG. com @STorrey. MD

Atrial fibrillation • Epidemiology • Most common arrhythmia in ED • 0. 4% in general population (10 X > 60 years) • Substantial morbidity and mortality • • Cardiovascular and overall survival 5 -fold risk stroke Diminished quality of life Significant health care costs

Etiology of atrial fibrillation • Enlargement of atria • Ischemic cardiomyopathy • Hypertensive cardiomyopathy • Valvular disease (mitral stenosis) • Excess stimulation • Hyperthyroid • Cocaine • Embolism

Natural history of atrial fib • Cellular and electrophysiologic remodeling • Apoptosis, necrosis, and fibrosis • Occur as early as 1 month • “Atrial fib begets atrial fib” • Paroxysmal Persistent Permanent

What’s the hurry? Anter Circ 2009

Predicting progression from paroxysmal to persistent atrial fib • HATCH score • • • HTN Age > 75 CVA or TIA COPD CHF 1 1 2 de Vos JACC 2010

HATCH score

Natural history of atrial fib • Relapse rate – up to 25% in few weeks • Spontaneous conversion – 25 - 50% • Thromboembolic risk • 5%/year – 1. 5% (age 50 -59) to 23% (age >80) • As diverse as the variety of patients • Progressive over time

ED Management of A Fib • Unstable vs. stable presentation • Rhythm vs. rate control • Anticoagulation?

Algorithm for hypotensive A. Fib

Unstable? • Hypotensive, conscious pt with atrial fib • Amiodarone – for rate control • May cardiovert within 4 -6 hours • Heparin advisable • Digoxin • Slow in onset, but may help • Diltiazem • Small doses

Algorithm for hypotensive A. Fib Atzema CL. Managing Atrial Fibrillation. Ann Emerg Med, 2015

The stable patient with A fib • Rate or Rhythm Control • < 48 hours since onset – cardioversion? • ≥ 65 years old – no difference in outcome • Sinus rhythm is preferable to A fib • Rate control • β-blockers or Ca-channel blockers • ? worse exercise tolerance with β-blockers • β-blockers with hx CAD

The stable patient with A fib • Rhythm Control • Electrical cardioversion – 90% effective • Chemical cardioversion – 60% effective • procainamide, propafenone, flecainide, amiodarone • Questions to consider • Time from onset of arrhythmia • Risk of thromboembolic event

Association of the Ottawa Aggressive Protocol with rapid discharge of ED patients with recent-onset atrial fibrillation or flutter Stiell IG, et al. CJEM 12: 181, 2010. • Stable patients with clear onset < 48 hours • Without ischemia, hypotension or CHF • Pharmacologic cardioversion • Procainamide 1 gm over 60 min • Electrical cardioversion • 150 -200 J biphasic synchronized

Ottawa Aggressive Protocol • 660 patients • • • IV procainamide 58% converted 243 underwent EC 92% converted Adverse events – 7. 6% (minor) Median LOS – 4. 9 hours 7 -day relapse – 8. 6%

Is Discharge to Home after ED Cardioversion Safe For the Treatment of Recent-Onset Atrial Fibrillation? von Besser K. Ann Emerg Med 58: 517, 2011 • • • Michael 1999 Burton 2004 Jacoby 2005 Stiell 2010 Scheuermeyer 2010 #EC 80 388 30 243 141 882 success 89% 86 97 92 96 92% d/c 100% 91 97 96 96%

Cardioversion of atrial fibrillation in ED: a prospective randomized trial. Bellone A, et al. Emerg Med J 29: 188. 2012 • Prospective, randomized trial from Italy • 247 patients with AF < 48 hours • Excluded comorbid disease and CHADS 2 ≥ 2 • 108/121 EC (89%) vs 93/125 PC (74%) • ED LOS – 180 min EC vs 420 PC • Relapse 2 month – 26% EC vs 28% PC

ED cardioversion of atrial fib • ED cardioversion is effective and safe • With identification of appropriate patient, and • With attention to thromboembolic risk • Saves time, money and resources • Patient satisfaction • Spare admission and unnecessary meds

CHADS 2 • • • CHF Hypertension Age ≥ 75 Diabetes Stroke/TIA 1 1 2

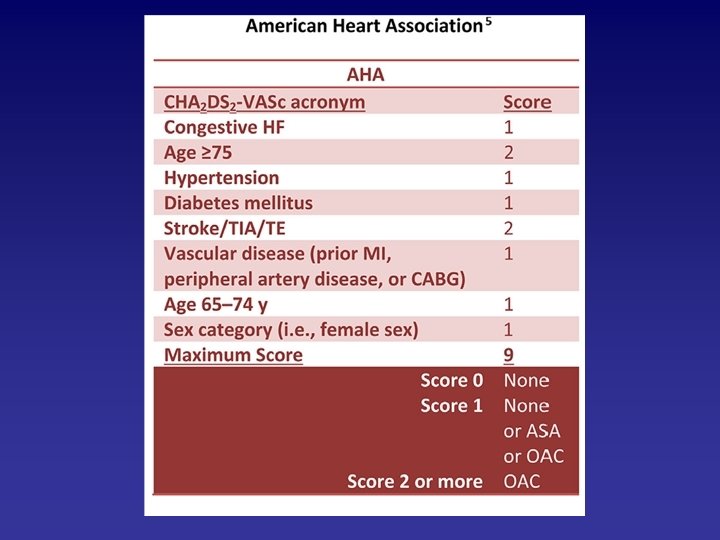
CHA 2 DS 2 -VASc • • • CHF Hypertension Age ≥ 75 Diabetes Stroke/TIA Vascular dz 1 1 2 1 • (MI, CABG, PVD) • Age 65 -74 y • Sex (female) 1 1
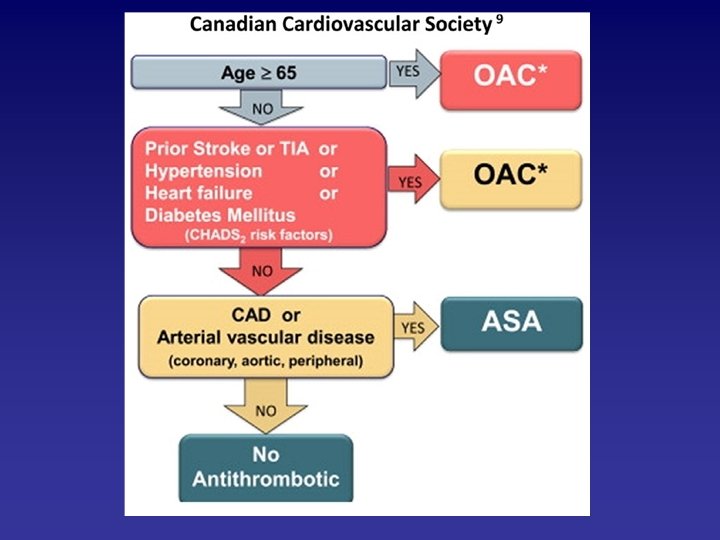
 • 2014 Canadian Cardiovasc Society")
To anticoagulate or not • 2012 European Society (ESC) • 2014 Canadian Cardiovasc Society (CCS) • 2014 American Coll Card (ACC/AHA) • All groups recommend anticoagulation for: • Age > 65 years • Mechanical heart valves • Rheumatic valvular disease
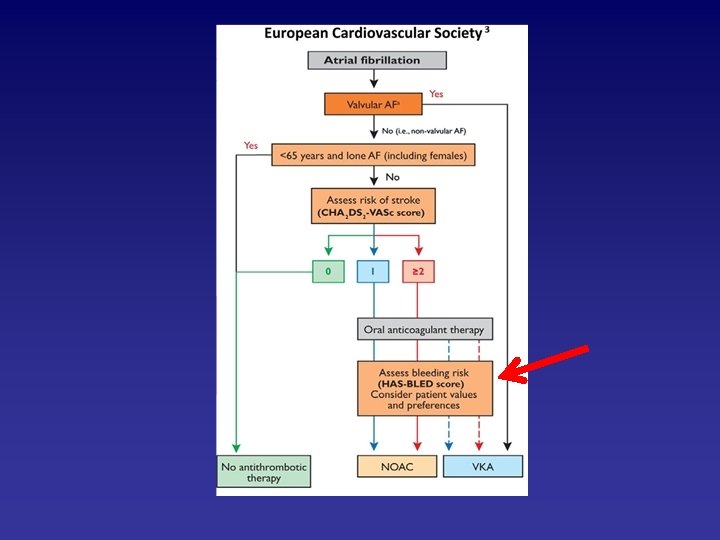

HAS-BLED • • H A S B L E D Hypertension Abnl renal or liver fx Stroke Bleeding hx Labile INRs Elderly Drugs or alcohol 1 1 or 2 1 1 1 or 2 ≥ 3 = high risk of bleeding

Atrial fibrillation in Sub-Saharan Africa Stambler BS. Internat J Gen Med 8: 231, 2015

Atrial fibrillation in Sub-Saharan Africa Stambler BS. Internat J Gen Med 8: 231, 2015

Thomboembolic Complications after Cardioversion of Acute Atrial Fibrillation Airaksinen KE, et. Al. J Am Coll Card 62; 1187, 2013 • 5, 116 cardioversions in 2, 481 patients • No peri-procedural anticoagulation • Embolic events within 30 days • 38 embolic events (31 strokes) – 0. 7% • Occurred median 2 days / mean 4. 6 days Fin. VC (Finnish Cardio. Version) Study

Thomboembolic Complications after Cardioversion of Acute Atrial Fibrillation Airaksinen KE, et. Al. J Am Coll Card 62; 1187, 2013 • Independent predictors • • Age > 60 years Heart failure Female sex Diabetes • Highest risk (CHF and DM) • Lowest risk (no CHF, < 60) 9. 8% 0. 2%

Time to Cardioversion for Acute Atrial Fibrillation and Thromboembolic Complications. Nuotio I, et. al. JAMA 312: 647, 2014 Time to cardioversion • < 12 hours • > 12 hours Incidence emboli • 0. 3% • 1. 1% Risk of stroke with anticoag – 0. 3 -0. 8% Risk without anticoag < 48 hrs – 0. 7%
 Receive Oral Anticoagulation? Chao")
Should Atrial Fib Patients with 1 Risk Factor (Beyond Sex) Receive Oral Anticoagulation? Chao TF, et al. J Am Coll Card 65: 635, 2015 • 12, 935 males (score 1) – 2. 75%/yr stroke rate • 1. 96% with vascular disease • 3. 50% those 65 -74 years old • 7, 900 females (score 2) – 2. 55%/yr • 1. 91% with HTN • 3. 34% those 65 -74 years old
 Receive Oral Anticoagulation? Chao")
Should Atrial Fib Patients with 1 Risk Factor (Beyond Sex) Receive Oral Anticoagulation? Chao TF, et al. J Am Coll Card 65: 635, 2015 • CHA 2 DS 2 -VASC risk factors are not equal • Age 65 – 74 associated with highest risk • Anticoagulation for 1 additional risk factor

Anticoagulation, CHA 2 DS 2 VASC score, and thromboembolic risk of cardioversion of acute A fib. Gronberg T, et al. Am J Cardiol 117: 1294 -98, 2016 • CHA 2 DS 2 VASC was significant predictor of thromboembolic complications in cardioversion of acute atrial fib • Periprocedural anticoagulation reduced risk 82% • High CHA 2 DS 2 VASC score had high rate of failed cardioversion or early recurrence of A fib ? rationality of rhythm control
 – inhibits thrombin • Rivaroxaban (Xarelto®) –")
NOACs Novel Oral Anticoagulants • Dabigatran (Pradaxa®) – inhibits thrombin • Rivaroxaban (Xarelto®) – blocks factor Xa • Apixaban (Eliquis®) • compared to warfarin, NOACs cause significant reduction in strokes, intracranial hemorrhage, major bleeding events and mortality Ruff CT, et al. Comparison efficacy and safety NOACs with warfarin in atrial fib – meta-analysis. Lancet 2014

Comparison of Efficacy and Safety of new Oral Anticoagulants with Warfarin in Atrial Fib Ruff CT, et al. Lancet 383; 955, 2014

NOACs Novel Oral Anticoagulants • • Fewer interactions with medications Fewer restrictions of foods No lab monitoring Rapid onset action – peak 3 hours • Contraindicated: • Mechanical heart valves • Mitral stenosis

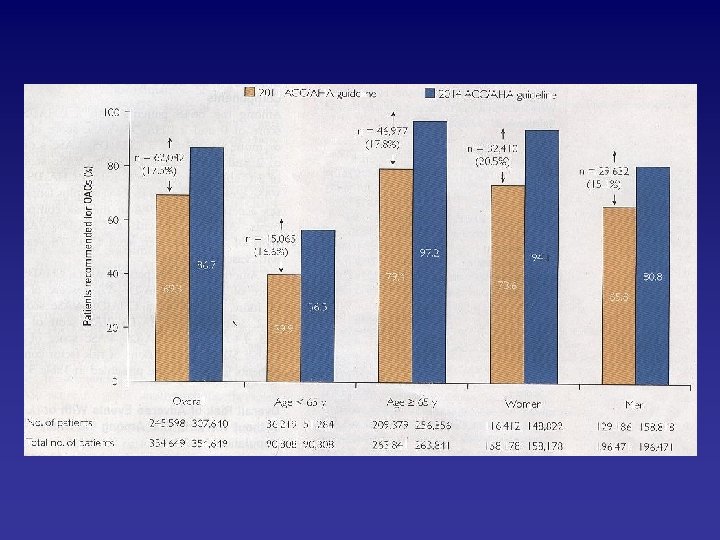
Impact on outcomes of changing treatment guideline recommendations for stroke prevention Chao TF, et al. Mayo Clin Proc 91: 567 -574, 2016. • Patients with atrial fib recommended OAC • 2011 guidelines • 2014 guidelines - 69% - 86% • Most woman with a fib (94%) • Most patients > 65 years (97%) • New guidelines = risk adverse outcomes • Hazard ratio – 0. 89

In conclusion… • Respect atrial fibrillation • Not exactly a benign arrhythmia • For ED management consider… • Rhythm control • Rate control • Anticoagulation

30 -day Death after ED Visit for A. Fib – The AFTER Study Atzema CL, et al. Ann Emerg Med 66: 658, 2015 1. Troponin positive 2. Other acute ED dx 3. COPD 4. Bleeding risk 5. Age ≥ 75 Age 65 – 74 6. CHF

30 -day Death after ED Visit for Atrial Fibrillation - the AFTER Study Atzema CL, et al. Ann Emerg Med 66: 658, 2015

Ca. Cl before IV diltiazem in management of atrial fibrillation. Kolkebeck T, et al. JEM 26: 395 -400, 2004. • Prospective, double-blind, placebo-control • 75 pts with a fib > 120/min • ½ received Ca. Cl / ½ placebo • Rate control same between groups • No significant side-effects noted • No benefit to maintaining BP
- Slides: 44