ATRIAL FIBRILLATION CURRENT EVALUATION AND MANAGEMENT Prabhat Hebbar

ATRIAL FIBRILLATION CURRENT EVALUATION AND MANAGEMENT -Prabhat Hebbar MD.

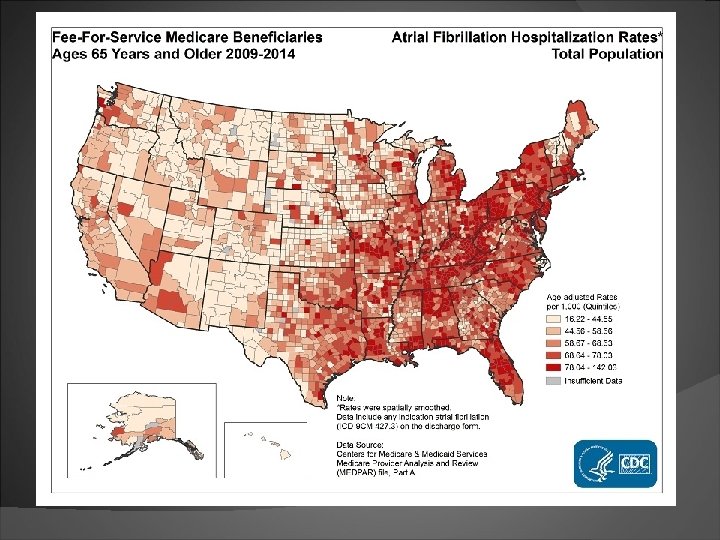
Epidemiology

CDC Fact Sheet 2017 2. 7– 6. 1 million people in the United States have AFib. 2% of people age < 65, 9% of people age > 65 years have AFib African Americans are less likely to have AFib. women generally live longer than men, more women than men experience AFib. Cost and Consequences 750, 000 hospitalizations/year. 130, 000 deaths/year. Cost: $6 billion/year. AFib causes 15%– 20% of ischemic strokes

Overall and sex-specific trends in incidence of AF between 1980 and 2000 -Miyasaka et al; Circulation 2006; 114: 119– 125

Stroke risk related to various cardiac conditions Framingham study - Wolf et al. Stroke 1991; 22: 983– 988.

Outcomes Mortality: doubled Stroke: increased 5 fold. More severe Hospitalization: more frequent Quality of life: wide variation, from no change to marked reduction. Congestive heart failure: wide variation from none to severe(tachymyopathy)

Mechanisms of AF

Electrophysiological mechanisms Triggers for onset + Substrate for maintenance Triggers mechanism: triggered activity and re-entry most common site: pulmonary veins - shorter refractory periods - abrupt changes in myocyte fiber orientation. paroxysmal AF: the junction between the PVs and the left atrium.

Triggers Haïssaguerre M et al. N Engl J Med 1998; 339: 659 -666.

Substrate Sustained atrial fibrillation triggers an inflammatory response leading to activation of myofibroblasts and release of cytokines - development of fibrosis - myocyte apoptosis - extracellular matrix generation and turnover - electrical and structural remodeling provides substrate for maintenance of to atrial fibrillation

Persistent Atrial Fibrillation

Natural History

Evaluation and Management

Detection An irregular pulse or irregular heart beat on auscultation should raise suspicion ECG is necessary to diagnose AF. Any arrhythmia that has the ECG characteristics of AF and lasts sufficiently long for a 12 -lead ECG to be recorded, or at least 30 s on a rhythm strip, should be considered as AF. Holter (24 -48 hrs) Event monitors (upto 1 month) Dual chamber pacemakers and defibrillators. Implantable loop recorder (upto 3 yrs)

Evaluation and Management Acute management: - relief of symptoms - assessment of AF-associated risk. Clinical Evaluation: Detailed history to assess - CHADs-2 Va. SC score/Stroke risk. - bleeding risk - time of onset (48 hrs) - conditions predisposing to AF - complications of AF

Testing EKG, Holter and event monitors Labs: CBC, BMP, TSH, +/- LFTs Echo: valvular, ventricular, atrial and congenital heart diseases, LA dimensions. Stress test: reasonable if signs/risk factors for CAD

Management Goals Reduce symptoms - rate vs rhythm control - cardioversion Preventing severe complications - anticoagulation - control of ventricular rate - adequate therapy of concomitant cardiac diseases

Management Cascade

Anticoagulation

Anticoagulation AF increases the risk of stroke by five-fold Stroke in atrial fibrillation more disabling. Anticoagulation reduces stroke risk by twothirds Anticoagulation only treatment shown to reduce mortality in AF Antiplatelet therapy reduces stroke risk by one-fifth

CHADS 2 Score Evolved from the AF investigators and SPAF investigators criteria. Initial rapid and easy to use means of assessing stroke risk. CHADS 2 score of 0, an adjusted rate of 1. 9 per 100 pt yrs Stroke rate increased by a factor of 1. 5 for each 1 -point Recommendations low risk (score 0): No anticoagulation moderate risk (score 1) Aspirin or oral anticoagulation high risk (score >/= 2) Oral anticoagulation - Gage et al, JAMA. 2001; 285: 2864 2870

CHADS 2 Score limitations Too many patients classified as moderate risk Even pt at mod risk (CHADs 2 =1) benefit from anticoagulation over aspirin Did not include many stroke risk factors

CHA 2 DS 2 -VASc Score Lip et al, Chest 2010; 137: 263– 272

“And there’s an app for that too”

Recommendations CHA 2 DS 2 -VASc score of 0, reasonable to omit antithrombotic therapy. CHA 2 DS 2 -VASc score of 1, no antithrombotic therapy or treatment with an oral anticoagulant or aspirin may be considered. CHA 2 DS 2 -VASc score of 2 or greater, oral anticoagulants are recommended CHA 2 DS 2 -VASc score of 2 or greater and who have end-stage CKD (Cr. Cl <15 m. L/min) or are on hemodialysis, it is reasonable to prescribe warfarin (INR 2. 0 to 3. 0) for oral anticoagulation.

Hart et al, Ann Intern Med. 2007; 146: 857 -867

Adjusted dose warfarin vs placebo/control 64% - Hart et al, Ann Intern Med. 2007; 146: 857 -867
 absolute risk")
Hart et al Stroke reduction Warfarin: 64% (95% CI, 49% to 74%) absolute risk reduction: 2. 7% per year Aspirin: Nonsignificant 19% (CI, -1% to 35%) absolute risk reduction: 0. 8% per year Warfarin vs antiplatelet therapy: 37% (CI, 23% to 48%) Major Bleeding warfarin vs aspirin: risk for intracranial hemorrhage doubled absolute risk increase small (0. 2% per year) Mortality warfarin versus control: all-cause mortality substantially reduced (26% [CI, 3% to 43%])

No. ACs vs Warfarin Limited reversal agents

Dabigatran Direct Thrombin Inhibitor Alternative to warfarin for CHADS 2 Va. Sc of 2 or greater in those with nonvalvular afib RE-LY Trial: 150 mg dose superior to warfarin in preventing ischemic stoke with no difference in bleeding Praxbind ® (idarucizumab) is a specific reversal agent for Pradaxa

RELY

Rivaroxaban Oral factor Xa inhibitor Rocket AF: noninferior to warfarin for stroke prevention no significant difference in risk of major bleeding intracranial and fatal bleeding occurred less frequently Antidote: FDA approves Andex. Xa

Rocket AF

Apixaban Oral factor Xa inhibitor Aristotle : superior to warfarin in preventing stroke caused less bleeding resulted in lower mortality Antidote: FDA approves Andex. Xa Dose Adjustment: Cr >1. 5, Age > 80, Wt < 60 kgs

Aristotle

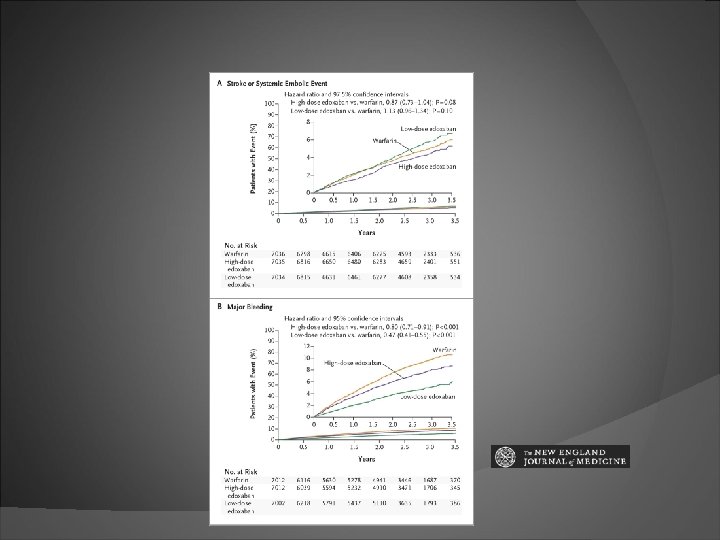
Edoxaban: ENGAGE AF study Oral factor Xa inhibitor edoxaban 30 mg and 60 mg vs Warfarin noninferior to warfarin with respect to the prevention of stroke or systemic embolism significantly lower rates of bleeding and death from cardiovascular causes

RATE VS RHYTHM CONTROL

Rate vs Rhythm control trials • Rhythm-control strategy offers no survival advantage over rate-control. • Lower risk of adverse drug effects, with the rate-control strategy. • Anticoagulation should be continued in this group of high-risk patients.

Outcomes Mortality and hospitalization: - No benefit of rhythm control - Post-hoc analysis: maintenance of sinus rhythm improves survival Quality of Life: - No differences in quality if life. - Post-hoc analyses: maintenance of sinus rhythm may improve quality of life. Ideal patient for rate control: Elderly patient with asymptomatic atrial fibrillation.
. Warfarin use")
Sinus Rhythm associated with decreased risk of death (HR 0. 53). Warfarin use associated with decreased risk of death (HR 0. 50) AADs associated with increased mortality only after adjustment for the presence of SR(HR 1. 49). AADs are not associated with improved survival, which suggests that any beneficial antiarrhythmic effects of AADs are offset by their adverse effects. If an effective method for maintaining SR with fewer adverse effects were available, it might be beneficial.

RACE II Trial • 614 pts with permanent AF • Lenient rate control: resting heart rate <110 bpm in AF • Strict rate control: resting heart rate of <80 bpm and an adequate increase in heart rate upon moderate exertion • Lenient rate control is as effective as strict rate control and is easier to achieve • Symptoms, adverse events, and quality of life similar in both groups. • Patients assigned to lenient rate control had fewer hospital visits.

Optimal rate control

Rhythm Control
 therapy Treatment is to reduce AF-related symptoms. Efficacy to maintain")
Principles of antiarrhythmic drug(AAD) therapy Treatment is to reduce AF-related symptoms. Efficacy to maintain sinus rhythm is modest. If one AAD ‘fails’, a clinically acceptable response may be achieved with another agent. Proarrhythmia or extra-cardiac side effects are frequent. Safety rather than efficacy considerations should guide the choice of AAD. Young patients should be considered for rhythm control Make sure patient has had adequate anticoagulation prior to initiation.

New algorithm for sinus rhythm maintenance in AF

Flecainide Drug of choice in pts with structurally normal hearts Start with 50 mg BID and then increase to 100 mg BID Start AV nodal blocking agent concomitantly Treadmill stress test 1 week after initiation Avoid if Cr Cl < 35 Adverse effects: - proarrhythmias - conduction abnormalities - acute rise in pacing threshold - heart failure exacerbation

Propafenone similar to Flecainide only difference: liver metabolism, so safe to use in renal failure patients 150 mg TID, upto 300 mg TID

Dofetilide Pure Class III agent Dose 125 – 500 mg BID based on Cr Cl cannot use with Verapamil or HCTZ Proarrhythmia risk 3. 3% highest in first 72 hrs Initiate in hospital can be used in CAD and CHF patients

Sotalol Class III + non specific beta blocker provides good rate control if Afib recurs renal excretion- dose adjustment in CRI 80 -160 mg BID preferred in pts with ICD preferred in pts with CAD Do not use in patients with CHF and EF<25% Proarrhythmia risk 2 -3% initiate in hospital

Dronedarone Amiodarone without the iodine moiety Class III agent, multichannel blocker + antiadrenergic activity. ATHENA: Reduction in hospitalization compared to placebo. reduction in cardiovascular deaths ANDROMEDA: stopped prematurely increased mortality in pts with advanced heart failure. PALLAS: increased rates of heart failure, stroke, and death from cardiovascular causes in permanent afib pts who were at risk for major vascular events Dosage: 400 mg BID

Amiodarone Most effective of the AADs but also most toxic Multi channel blocker Loading: 400 mg PO BID/TID Maintenance: 200 mg daily EKG 1 week after initiation Adverse effects: Bradycardia, liver toxicity, QT prolongation (<0. 5%), Hypothyroidism(20%), Hyperthyroidism (3%), Lung toxicity, Skin pigmentation Drug interaction: reduces hepatic metabolism of digoxin and warfarin. Monitoring: LFTs, TFTs, CXR, PFTs( yearly)

CATHETER ABLATION FOR AF

Guidelines Indicated in patients with Symptomatic paroxysmal AF refractory or intolerant to at least 1 antiarrhythmic medication when a rhythm-control strategy is desired (1 A) Symptomatic persistent AF refractory or intolerant to at least 1 antiarrhythmic medication. (2 A) Recurrent symptomatic paroxysmal AF, catheter ablation is a reasonable initial rhythm-control strategy. (2 A)

Catheter ablation of AF Radiofrequency Cryoablation

• • • Primary endpoint ( Death + CVA + Bleeding + Cardiac arrest) Ablation therapy not superior to drugs for CV outcomes at 5 years Significant reductions in death and CV hospitalizations with ablation On treatment analysis ablation demonstrated superior efficacy As this was a single blinded trial there was a high crossover rate. Time to first AF recurrence was greater

Restoration of sinus rhythm by catheter ablation in pts with CHF led to significant improvements in - LVEF (21%) - Symptoms - Exercise capacity - Quality of life.

Catheter ablation as compared to amiodarone in pts with CHF - More successful in maintaining sinus rhythm - Reduction in hospitalizations - Reduction in mortality.

AV node ablation

AV node ablation Guidelines AV nodal ablation with permanent ventricular pacing is reasonable to control heart rate when pharmacological therapy is inadequate and rhythm control is not achievable. (IIA)

AV node ablation provides highly effective control of ventricular rate patients in whom pharmacological rate control has failed and rhythm control with drugs and/or LA ablation has failed. improves quality of life reduces mortality patients with reduced LV function may require biventricular pacing after atrioventricular node ablation.

Left atrial appendage occlusion Watchman device only FDA approved percutaneous LAA closure device semi-spherical nitinol frame with a polyethylene terephthalate membrane coating deployed transseptally using a dedicated 14 Fr sheath usually under transesophageal echocardiography and fluoroscopic guidance.

707 pts with NV Afib randomized to Watchman vs continued warfarin. Primary efficacy endpoint stroke, systemic embolism and CV death 3. 0% vs 4. 3% WATCHMAN vs Warfarin (noninferior) Primary safety events 5. 5% vs 3. 6% (more safety events in the Watchman arm)

Recommendations FDA approved for patients at increased risk of stroke and systemic embolism based upon CHADS 2 or CHA 2 DS 2 -VASc scores deemed by their physicians to be suitable for warfarin therapy have an appropriate rationale to seek a nonpharmacological alternative to warfarin

Conclusions Epidemic of atrial fibrillation. Assess stroke risk and anticoagulate appropriate patients. Rate vs rhythm control strategy. Ablation is effective and safe in selected patients. AV node ablation and pacemaker. NOACs are effective and safe. Consider Watchman in patients not suitable for long term anticoagulation.

Thank you
- Slides: 67