ATGs how many ATG Fresenius rabbit serum containing

ATGs: how many? ? ATG Fresenius: rabbit serum containing polyclonal antibodies against the ALL-T leukemia line Jurkat. TMG Genzyme: rabbit serum containing polyclonal antibodies against human thymocytes.

Antibodies specificities ATG/ALG CD m. Ab inhibitions Source Fl-labeled CD m. Ab-50% inhibition point in μg/ml of ATG/ALG ATG AM CD 2 CD 3 CD 4 CD 5 CD 7 CD 8 130 550 280 1100 150 190 (ATG horse Upjohn) Merieux rabbit 40 230 400 20 70 30 Merieux horse 60 600 400 70 125 130 Fresenius 180 4400 >5000 240 1700 MALG 460 1000 1400 500 220 300 (horse ATG Minnesota) Bourdage et al. , Transplantation 1995; 59: 1194 -1200

ATG-F / TMG-G: Different spectrum of specifities against co-stimulation molecules activity Activities anti CTLA - 4 ATG - F ++++ TMG - S ++ anti CD 86 ATG - F +++ anti CD 28 TMG - S +++ anti CD 80 ATG - F ++++ TMG - S Pistillo et al. , Transplantation 2000
 Total dose 15 mg/kg 3 mg/kg Cs. A - MTX")
ATG–F administration schedule (BO) Total dose 15 mg/kg 3 mg/kg Cs. A - MTX -6 -5 -4 -3 -2 -1 0 Total dose 30 mg/kg 10 mg/kg Cs. A - MTX -6 -5 -4 -3 -2 -1 0
 prior allogeneic")
Prophylaxis of chronic Gv. HD with or without anti T-lymphocyte globulin (ATG-F) prior allogeneic peripheral stem cell transplantation from HLAidentical sibling after myeloablative conditioning in patients with acute leukemia: A randomised phase III study Primary endpoint: reduction of c. GVHD from 60% to 35% Sample size: 60/arm Study medication: ATG-Fresenius 10 mg/kg on days -3 -2 -1
 Sponsor: University Hospital Hamburg Protocol Coordinator Germany: Nicolaus")
EUDRACT-Number 2005 -005719 -83 (ATGfamily study) Sponsor: University Hospital Hamburg Protocol Coordinator Germany: Nicolaus Kröger Hamburg Protocol Coordinator Italy: Bologna Scientific Committee: Francesca Bonifazi Nicolaus Kröger, Axel R. Zander, Frank Schulz-Kindermann Ernst Holler, Hermann Einsele, Jürgen Finke, Rainer Schwerdtfeger, Michael Schleuning Gerhard Ehninger, Martin Bornhäuser, Hans-Jochem Kolb Francesca Bonifazi, Giuseppe Bandini,
 and blood lymphocytes")
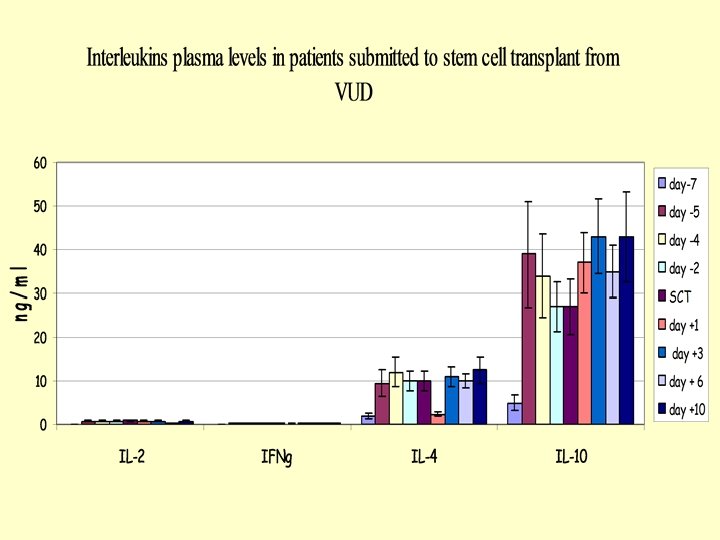
Levels of plasma ATG (active) and blood lymphocytes

mean channel value of fluorescence arbitrary units ‘

Half time of Jurkat-reactive antibodies 8 patients after 30 mg/kg ATG-Fresenius days -3, -2, -1.

Preparative regimen Tot. dose 7. 5 mg 800 Gy ATG – G 800 c. Gy Cs. A/MMF From Lowsky et al. , 2005

ATG-G levels From Lowsky et al. , 2005

Intracellular interleukin-4 Comparison of Intracellular Cytokine Production. From Lowsky et al. , 2005

Effect of ATG prior to allogeneic stem cell transplantation Before Tx After Tx To facilitate engraftment To reduce risk of Gv. HD

Skin NMA GVHD after NMA Vs MA Allo. SCT: MA Morbidities involving the skin, liver, and gut after nonmyeloablative conditioning compared with myeloablative conditioning. Liver Gut Figura 2 Overall Acute Chronic Mielcarek et al. Blood 2003

From Sala-Torra et al. , 2008
 Nr. pazienti")
Linfomi. Ric GVHD ACUTA E CRONICA: ATG VS NON ATG (BO) Nr. pazienti

I and II treatment plans I ATG-G 10 mg/KG -4 200 Gy FK / MTX 3/16 graft failure -1 0 II ATG-G 10 mg/KG -10 -7 450 Gy -1 0 G-csf FK / MTX no graft failure more infections more relapse From Toor et al. , 2008

Hematopoietic Stem Cell Transplantation in a canine model c. ATG-G 2 -5 mg/kg - 12 100 Gy -7 Csa /MMF 0 From Diaconescu et al. , 2005
 Maximum Donor MNC Chimerism (%) Graft Engraftm Rejection ent Duration (wk)")
Marrow Cells (million/kg) Maximum Donor MNC Chimerism (%) Graft Engraftm Rejection ent Duration (wk) Dog. N°. c. ATG-g (mg/kg) TNC CD 34 CD 3 G 200 3. 5 263 4. 2 17. 8 5 Yes 8 G 198 4 345 4. 1 25 Yes 18 G 166 5 206 7. 5 6. 9 25 Yes 11 G 208 4 453 11. 3 38. 5 40 No ≥ 36 G 252 4 175 6. 6 13. 2 5 Yes 8 From Diaconescu et al. , 2005

Preparative regimen Tot. dose 7. 5 mg 800 Gy ATG – G 800 c. Gy Cs. A/MMF From Lowsky et al. , 2005

Lymphoid and myeloid engraftment From Lowsky et al. , 2005

T-cell engraftment From Lowsky et al. , 2005

Conclusioni 1. Utilizzo ATG non sarebbe indicato, in quanto riduce la GVHD, soprattutto cronica, diminuendo la Gv. L. 2. Utilizzo ATG indicato in quanto necessario per favorire l‘attecchimento, il chimerismo completo, elementi di primaria importanza ai fini del successo (eradicazione della malattia) del trapianto. La tossicità è minima. Gli ATG concorrono a realizzare dei condizionamenti “ridotti” evitando l’impiego di farmaci citotossici/immunosoppressivi. 3. Poiché il punto 2 è molto più importante del punto 1, gli ATG devono essere usati nei regimi “a intensità ridotta”.
- Slides: 31