Asymptomatic abnormal LFTs again ignore reassure investigate or

Asymptomatic abnormal LFTs…. . again! ignore, reassure, investigate or refer? Alastair Mac. Gilchrist Laboratory/Primary care Meeting 7 November 2013
")
Why bother? (1)
 ► Liver disease is usually asymptomatic until irreversible…. . the classic")
Why bother? (2) ► Liver disease is usually asymptomatic until irreversible…. . the classic “silent killer” ► Most liver disease is due to alcohol, NAFLD or viral hepatitis…. . all preventable or reversible in early stages
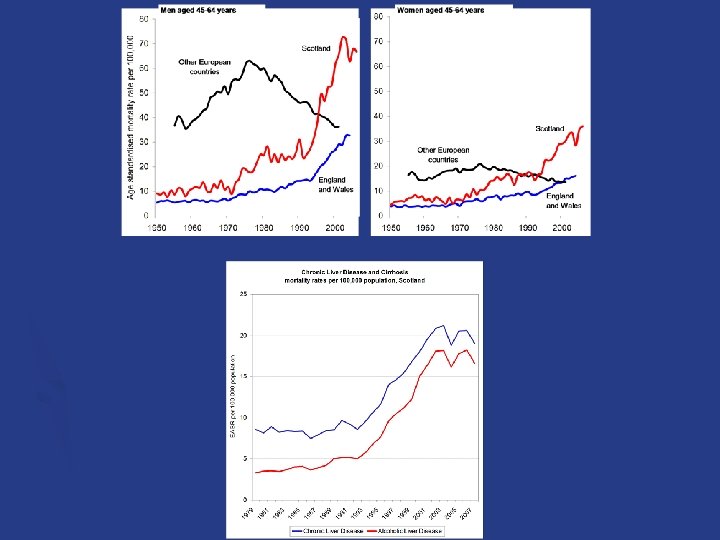

► Alcohol kills a Scot every 3 hours § § ► 1 in 20 of all deaths in Scotland Twice that of England Doubled in last 15 years 1 in 10 of deaths in Scots aged 35 -54 is due to alcoholic liver disease. Enough alcohol is sold in Scotland to enable every adult to exceed safe drinking guidelines § almost double that of England § Britain’s consumption has doubled since 1960 ► Alcohol is 70% more affordable than in 1980 Price Consumption Harm
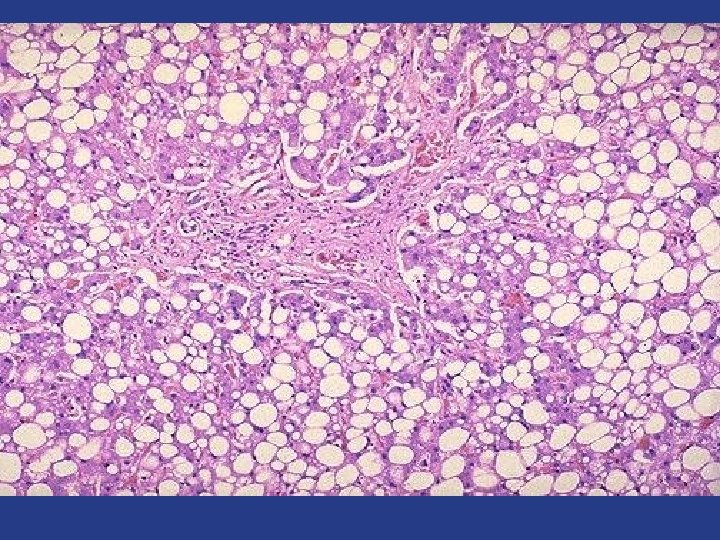

NAFLD is a big problem Very common ► Up to 30% of population ► Up to 75% if obese 2. 2 -5% will develop cirrhosis over 20 years 3. Difficulty distinguishing progressive disease (i. e. fibrosis) 1.

The future of hepatitis C therapy e. g. sofosbuvir, daclatasvir, ledipasvir interferon-free oral once-daily dosingle combi-pill short course minimal side effects

hepatitis C therapy is changing pre 2011 genotype 2 or 3 genotype 1 drugs peg-interferon + ribavirin duration 24 weeks 48 weeks cure up to 80% up to 40% now genotype 2 or 3 drugs peg-interferon + ribavirin + bocepravir or telapravir duration 24 weeks up to 48 weeks cure up to 80% up to 70% 2015 ? genotype 2 or 3 genotype 1 drugs DAAs duration 12 weeks ? cure 100% ? genotype 1

What are abnormal liver function tests? ► bilirubin ► ALT ► alkaline phosphatase ► GGT ► albumin ► AST ► prothrombin ► FBC ► creatinine time

GGT v AST ► GGT § § isolated GGT with raised MCV – consider alcohol in female NAFLD, GGT predicts cirrhosis GGT indicates liver source for ALP ignore GGT alone <100 ► AST § in ALD, AST often > 2 x ALT § in NAFLD, suspect significant fibrosis if ► AST > ALT (AST/ALT > 0. 8) ► APRI score (AST: platelet ratio) >1. 5 routine LFTs in primary care: remove GGT and add AST?

The patient with asymptomatic abnormal LFTs ► ► ► NAFLD is not the only diagnosis Pattern and duration are important Consider: § § § ► Measure: § § § § ► Alcohol history Hepatitis risk factors Drugs metabolic syndrome clues Autoimmune disease clues Family history Viral hepatitis serology HBs. Ag, anti-HCV Ab Autoimmune markers ASMA, ANA, AMA Glucose Lipids Ferritin Caeruloplasmin (if <55 y) Alpha-1 -antitrypsin phenotype Ultrasound HBV, HCV AIH, PBC NAFLD haemochromatosis Wilson’s disease α-1 -Antitrypsin deficiency

Have they got fibrosis/cirrhosis? 1. Primary care ► Clinical exam ►Hepatosplenomegaly ►Spider naevi, etc. ► LFTs ►GGT ►AST/ALT ►Albumin ►Platelets ► Ultrasound

Have they got fibrosis/cirrhosis? 2. Secondary care ► APRI score ► Hyaluronic acid ► Marker panels § ELF § Fibrotest ► Elastography § Fibroscan § ARFI ► Liver biopsy

“liver screen” ► Who? ↑ALT/GGT/AP ► What? USS Aetiology ► Action? > 2 x ULN 2 occasions > 4 weeks apart HCV Ab, HBs. Ag ASMA, ANA, AMA ferritin caeruloplasmin (<55 y) glucose, lipids (TTG, TFTs) Staging AST platelets albumin Refer if +ve aetiology screen fibrosis/cirrhosis ↓platelets AST/ALT>0. 8 splenomegaly unexplained ↓alcohol ↓weight ALD NAFLD

Sub-groups ► ↑bilirubin ► ↑GGT ► AP alone: ► ↑AP + GGT: usually Gilbert’s (exclude haemolysis) (check unconjugated) think alcohol (think NAFLD) probably not liver consider isoenzymes usually biliary USS for biliary obstruction Check AMA for PBC

So…for the next patient with asymptomatic abnormal LFTs…. investigate? if persistent according to clinical picture don’t miss treatable disease refer? if require treatment, suspect advanced disease or diagnosis unclear reassure? if negative screen and no suspicion of advanced disease ignore? never!

and…. . a very big thanks to Simon, Sara, Emily and Thulani Your Text Here
- Slides: 18