ASTHMA ZAID ALGHANANEEM OBSTRUCTIVE LUNG DISEASES Characterized by

ASTHMA ZAID ALGHANANEEM

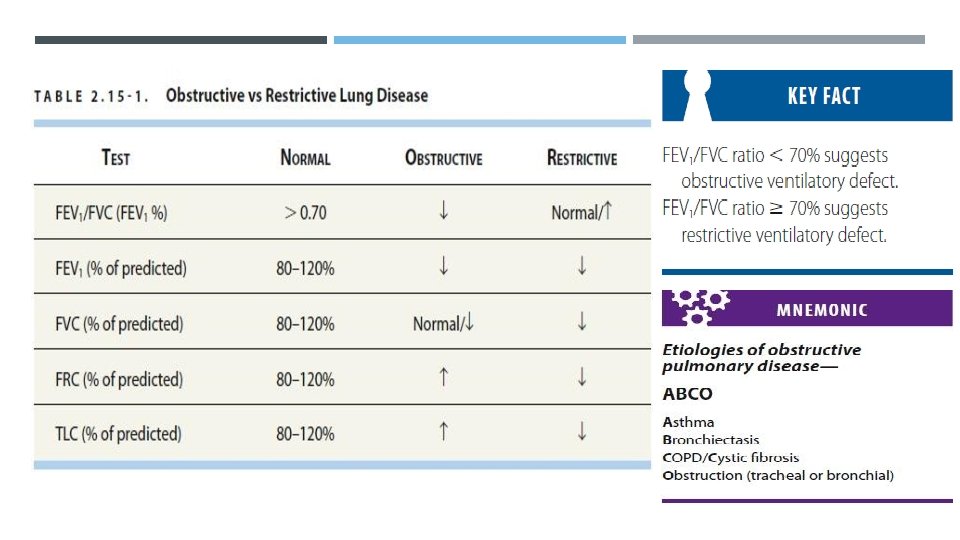
OBSTRUCTIVE LUNG DISEASES Characterized by airway narrowing or collapse that causes impaired expiration; results in air trapping. ASTHMA : Reversible airway obstruction 2° to bronchial hyperreactivity, airway inflammation, mucous plugging, and smooth muscle hypertrophy. Most often diagnosed in childhood or early adulthood but can present later. Asthma is associated with T helper cell type-2 (Th 2) immune responses, which are typical of other atopic conditions. Elevated levels of Th 2 cells in the airways release specific cytokines that promote eosinophilic inflammation and immunoglobulin E (Ig. E) production.

In asthma, all cells of the airways are involved and become activated. Included are eosinophils, neutrophils, T cells, mast cells, alveolar macrophages and dendritic cells, epithelial cells, fibroblasts, and bronchial smooth muscle cells. These cells also regulate airway inflammation and initiate the process of remodeling by the release of cytokines and growth factors. Asthma is Type I hypersensitivity reaction. The relationship between atopy (the propensity to produce Ig. E) and asthma is well established and in many individuals there is a clear relationship between sensitization and allergen exposure, as demonstrated by skin-prick reactivity or elevated serum-specific Ig. E. Asthma triggers include allergens, URIs, cold air, exercise, drugs (Aspirin, Beta blockers), GERD, smoking, obesity and stress.

CLINICAL PRESENTATION Asthma is a disease of exacerbation and remission, so the patient may not have any signs or symptoms at the time of examination. Usually presents with dry cough, episodic wheezing, dyspnea, and/or chest tightness, often worsening at night or in early morning. PE: Wheezing, prolonged expiration (↓ I/E ratio), increased accessory muscle use, tachypnea, tachycardia, hyperresonance, and possible pulsus paradoxus (severe). Late signs: ↓ Breath sounds, cyanosis, and ↓ O 2 saturation, hypercapnia (↑ Paco 2). Best initial test: Spirometry/PFTs; obstructive pattern that is reversible with short-acting β- agonists (SABA). FEV 1/FVC < 70%, ↓ FEV 1, normal/↓ FVC, ↑ RV and TLC. Normal/ ↑ DLCO (diffusing capacity of the lung for carbon monoxide), also known as transfer factor for carbon monoxide or TLCO Increase in FEV 1 ≥ 12% with SABA (albuterol). PFTs are often normal between exacerbations.

Methacholine challenge: Tests for bronchial hyperresponsiveness; useful when PFTs are normal but asthma is still suspected. Considered positive with ≥ 20% decrease in FEV 1. Arterial blood gas (ABG): Early exacerbation: Respiratory alkalosis caused by hyperventilation (↓ Paco 2, ↑ p. H, mild hypoxemia). Late/severe exacerbation (impending respiratory failure): Respiratory muscle fatigue results in respiratory acidosis caused by inability to ventilate (normalizing Paco 2, normalizing p. H, ↓ Pao 2). Chest x-ray (CXR): Normal appearance to hyperinflation with flattening of the diaphragm, lobar collapse may be seen if mucus occludes a large bronchus. Symptomatic patients should be instructed to record peak flow readings after rising in the morning and before retiring in the evening. A diurnal variation in PEF of more than 20% (the lowest values typically being recorded in the morning) is considered diagnostic

Cough may be the dominant symptom in some patients, and the lack of wheeze or breathlessness may lead to a delay in reaching the diagnosis of so-called ‘coughvariant asthma’. The diagnosis may be supported by the presence of atopy demonstrated by skin- prick tests or measurement of total and allergen-specific Ig. E Aspirin-exacerbated respiratory disease: Samter’s triad of asthma and chronic rhinosinusitis with nasal polyps that is exacerbated with aspirin or NSAID use. Pseudoallergic reaction (not Ig. E mediated).
")
ACUTE SEVERE ASTHMA An episode can progress over several days or hours (usual scenario) or progresses rapidly over 1 to 2 hours. The patient is anxious in acute distress and complains of severe dyspnea, shortness of breath, chest tightness. The patient is only able to say a few words with each breath. Signs include expiratory and inspiratory wheezing on auscultation (breath sounds may be diminished with very severe obstruction), dry hacking cough, tachypnea, tachycardia, pale or cyanotic skin, hyper-inflated chest with intercostal and supraclavicular retractions, and hypoxic seizures if very severe. Peak expiratory flow and/or FEV 1 less than 40% of normal predicted values. Decreased arterial O 2 (Pa. O 2), and O 2 saturations by pulse oximetry (Sa. O 2 less than 90% [0. 90] on room air is severe).

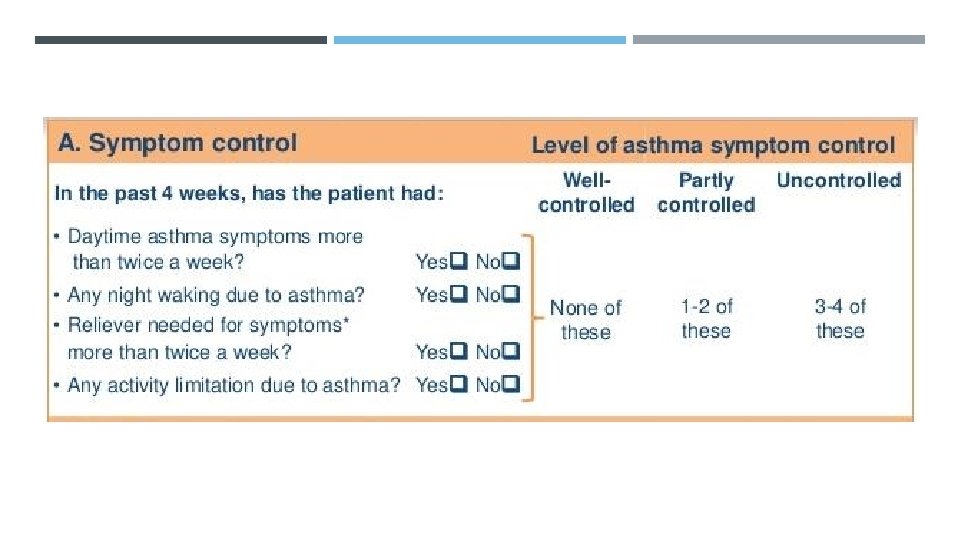
GOALS OF ASTHMA TREATMENT Symptoms control: Few asthma symptoms No sleep disturbance No exercise limitation Risk reduction: Maintain normal lung function Prevent flare-ups (exacerbations) Prevent asthma deaths Avoid medication side-effects

NON-PHARMACOLOGICAL STRATEGIES AND INTERVENTIONS Smoking cessation advice: is particularly important, as smoking not only encourages sensitisation but also induces a relative glucocorticoid resistance in the airway. Occupational asthma: identify and remove occupational sensitizers as soon as possible. Avoiding triggers: This is particularly important in the management of occupational asthma but may also be relevant in atopic patients
")
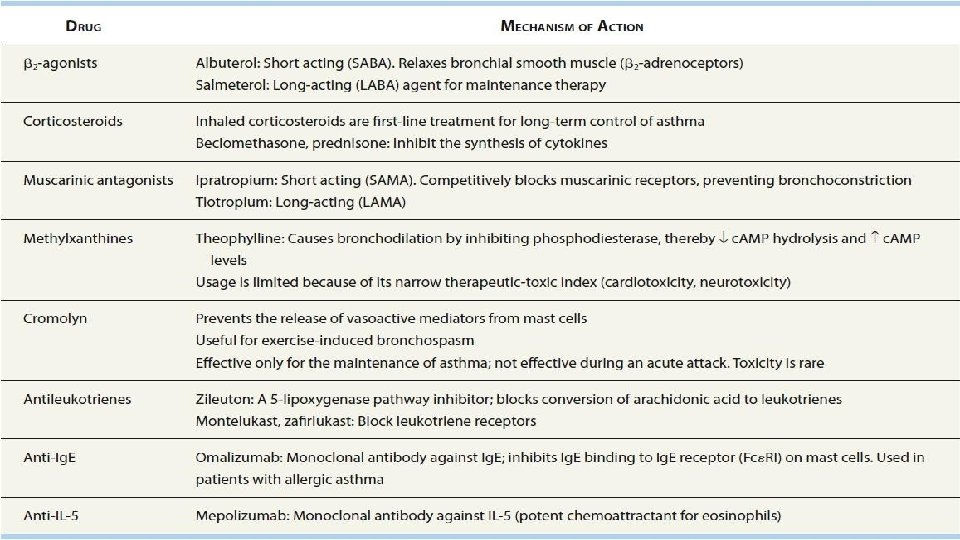
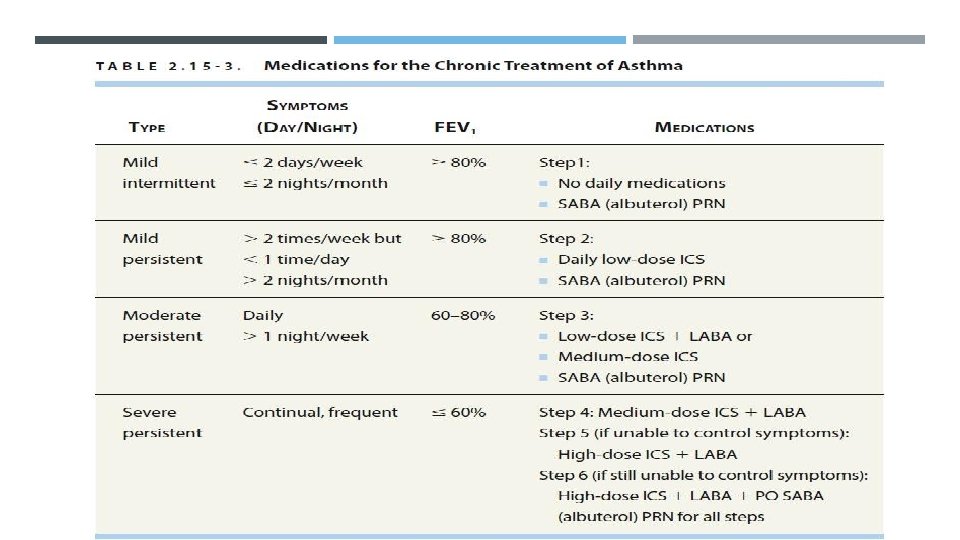
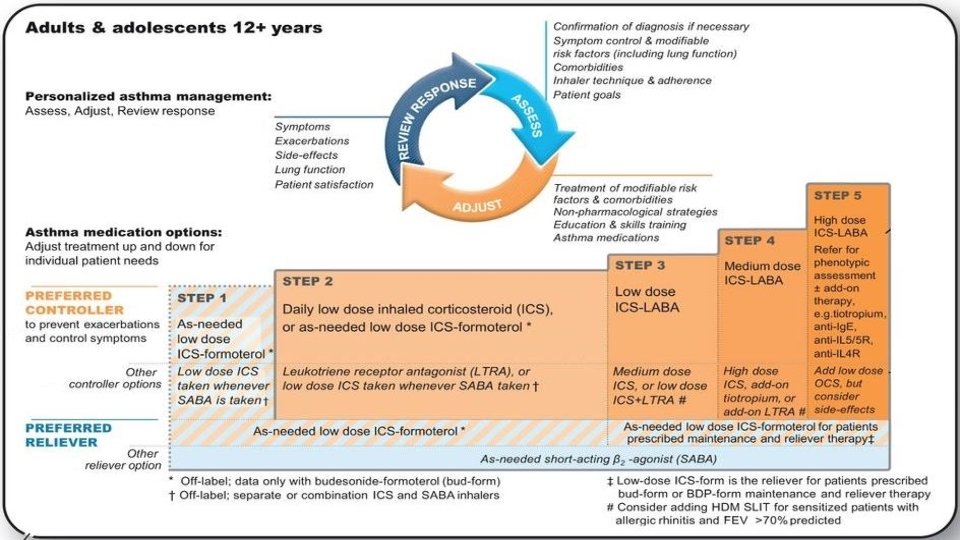
MAINTENANCE THERAPY Determined by the classification of asthma severity Step 1: Inhaled SABA (albuterol) as needed for symptom control is first-line. Step 2: Add daily medication for long-term control. Low-dose inhaled corticosteroids (ICS) are preferred. Alternatives include cromolyn, leukotriene receptor antagonist (LTRA), or theophylline. Continue albuterol PRN. Step 3: Add long-acting β-agonist (LABA) such as salmeterol to low-dose ICS or ↑ dose of ICS to medium-dose. Continue albuterol PRN. Step 4: Medium-dose ICS + LABA. Continue albuterol PRN. Step 5: High-dose ICS + LABA. Consider omalizumab (anti-Ig. E) or mepolizumab (anti-IL-5) for patients with allergies (↑ Ig. E). Continue albuterol PRN. Step 6: High-dose ICS + LABA + oral corticosteroid. Continue albuterol PRN.

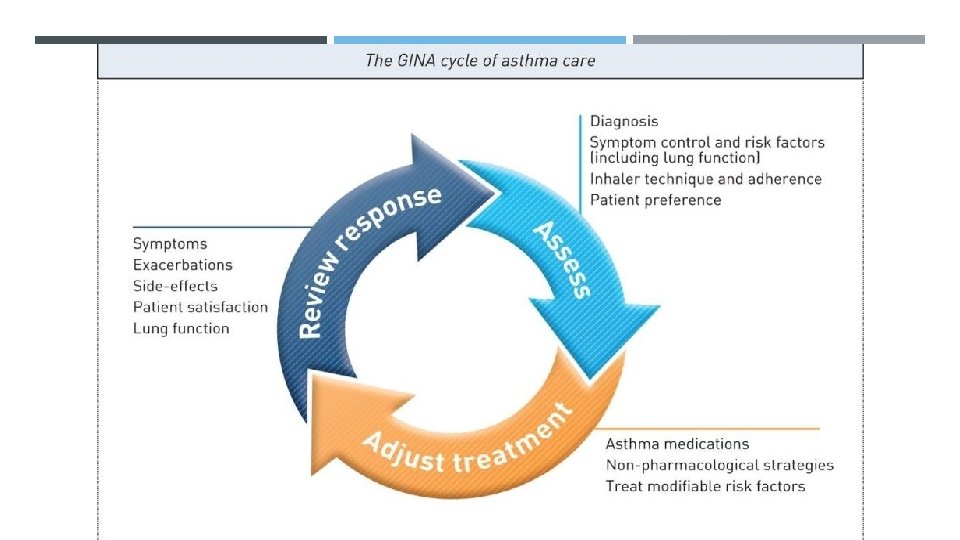
Every patient should be trained in essential skills and guided asthma self- management, including: 1. Asthma information 2. Inhaler skills 3. Adherence 4. Written asthma action plan 5. Self-monitoring of symptoms and/or peak flow 6. Regular medical review Assess symptom control, exacerbations, side effects, lung function and patient satisfaction

Stepping up: Periodic adjustment of controller treatment by clinician and/or patient may be needed. - Sustained step up (for at least 2 -3 months): if symptoms and/or exacerbation persist despite 2 -3 month of controller treatment. - Short-term step-up (for 1 -2 weeks): during viral infection or allergen exposure. Stepping down: Consider stepping down treatment once good control has been achieved and maintained for 3 months, to find the lowest treatment that control both symptoms and exacerbations, and minimizes side-effects.

Metered-dose inhaler is an inhaler device with specified doses that provides a certain dose of the active agent in each puff.

ACUTE ASTHMA EXACERBATION MANAGEMENT Assess exacerbation severity while starting SABA and oxygen. Assess dyspnea (e. g. is the patient able to speak sentences or only words), respiratory rate, pulse rate, oxygen saturation and lung function. Check for anaphylaxis. Consider alternative causes of acute breathlessness (e. g. heart failure, upper airway dysfunction, inhaled foreign body or pulmonary embolism). Arrange immediate transfer to: 1. Acute care facility if there are signs of severe exacerbation. 2. Intensive care if the patient is drowsy, confused, or has a silent chest. For these patients, immediately give Inhaled SABA (repeated doses), Inhaled ipratropium bromide, Oxygen, Systemic corticosteroids
, systemic glucocorticoids. SABA/ ipratropium and magnesium can")
O 2, SABA (albuterol is first-line), systemic glucocorticoids. SABA/ ipratropium and magnesium can be used in severe exacerbations. Never use ipratropium alone in asthma treatment. Consider intubation in severe cases (cyanosis, inability to maintain respiratory effort, altered mental status) or acutely in patients with a Paco 2 > 50 mm. Hg or a Pao 2 < 50 mm. Hg.
 should be administered to maintain the oxygen")
Oxygen: High concentrations (humidified if possible) should be administered to maintain the oxygen saturation above 92% in adults. High doses of inhaled bronchodilators: Short-acting β 2 -agonists are the agent of choice. Ipratropium bromide provides further bronchodilator therapy and should be added to salbutamol in acute severe or lifethreatening attacks. Systemic glucocorticoids: These reduce the inflammatory response and hasten the resolution of an exacerbation. They should be administered to all patients with an acute severe attack. They can usually be administered orally as prednisolone but intravenous hydrocortisone may be used in patients who are vomiting or unable to swallow. There is no evidence base for the use of intravenous fluids but many patients are dehydrated due to high insensible water loss and will probably benefit. Potassium supplements may be necessary, as repeated doses of salbutamol can lower serum potassium. Intravenous magnesium may provide additional bronchodilatation in patients whose presenting PEF is below 30% predicted.

FOLLOW-UP AFTER EXACERBATION Exacerbation often represent failures in chronic asthma care, and they provide opportunities to review the patient’s asthma management. All patients must followed up regularly by health care provider until symptoms and lung function return to normal. The acute attack should prompt a look for and avoidance of any trigger factors, the delivery of asthma education and the provision of a written selfmanagement plan.
- Slides: 23