Assisted births lowering instrumental birth rates Women who

• Assisted births • lowering instrumental birth rates. • Women who use epidural as a form of pain relief are at increased risk of having an instrumental assisted birth

• Birth by ventouse • -used more commonly than forceps. • - The vacuum extractor is an instrument that applies traction. • - an alternative to forceps. • -The cup cleaves to the baby's scalp by suction with maternal effort.

• • • The use of the ventouse a delay in labour and the head is engaged no cephalopelvic disproportion CPD. useful in the case of a second twin, when the head relatively high. • vacuum extractor is less likely to achieve a successful vaginal delivery than forceps.

• • • the ventouse is associated with cephalohaematoma facial and cranial injuries are common with forceps. The cup is positioned over the sagittal suture. Soft and rigid vacuum extractor cups -The metal cups , or the Malstrom type , have a central traction chain and a vacuum conduit. • - silicone rubber cup( malleable silicone cup) is shaped to the contour of the baby's head • -Soft cups have a poorer success rate than metal cups, but are less likely to be associated with scalp trauma.

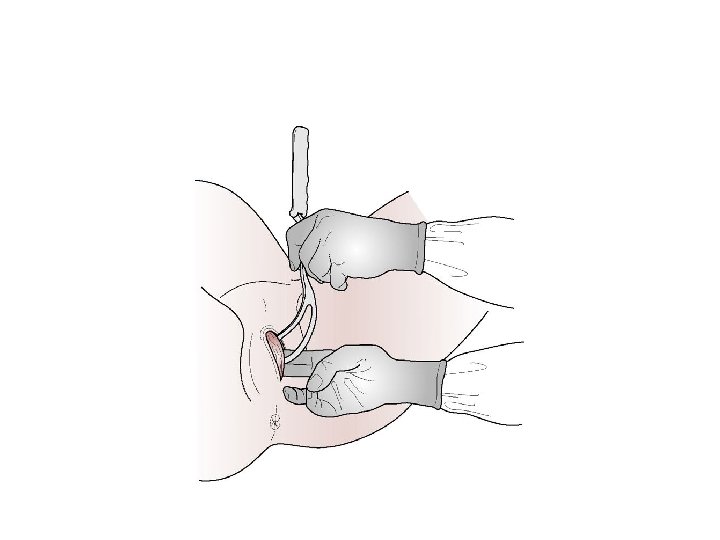
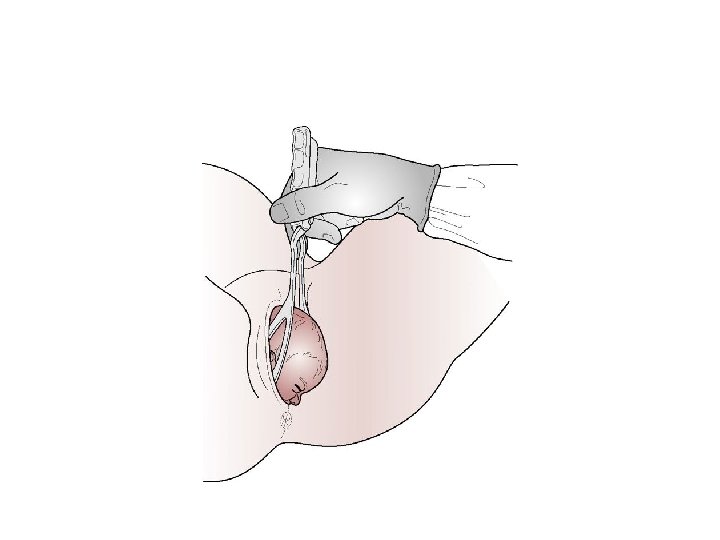
• • • Procedure - lithotomy position - Local anaesthesia , or inhalational analgesia. - Pudendal nerve block or epidural - Episiotomy is not routinely carried out. -The procedure is explained and consent obtained - the bladder is emptied. -The fetal heart rate is recorded regularly. - The cup of the ventouse is placed on the flexing point of the fetal head.


• - traction is applied with a contraction, with maternal effort, • -This traction is done in a downwards and backwards direction, then in a forwards and upwards manner, thus following the curve of Carus. • -The vacuum is released and the cup then removed at the crowning of the fetal head. • Precautions in use • • ensure that no vaginal skin is trapped in the edges of the cup • • Prolonged or excessive traction should not be used. • • Ask for help, Address the client, Adequate anaesthesia • • Bladder empty • • Cervix must be completely dilated • •

• Determine the position of the fetus • • Equipment and extractor ready • • Fontanelle, apply the cup over the sagittal suture • • Gentle traction at right angles • • Halt traction and reduce the pressure, repeat the cycle with the next contraction • • Incision, of episiotomy, if necessary • • Jaw is reachable, so, remove the vacuum cup

• Complications • - prolonged traction will increase the likelihood of scalp abrasions, cephalohaematoma or subaponeurotic bleeding • -Failure of the ventouse , This is more likely in the presence of excessive caput, less experienced practitioners.

• The midwife ventouse practitioner • Midwife ventouse practitioners must be well educated and trained before carrying out this procedure. • Birth by forceps • delivery of the fetal head or to protect the fetus or the mother • used to assist the delivery of the after-coming head of the breech • to draw the head of the baby up and out of the pelvis at caesarean section birth.

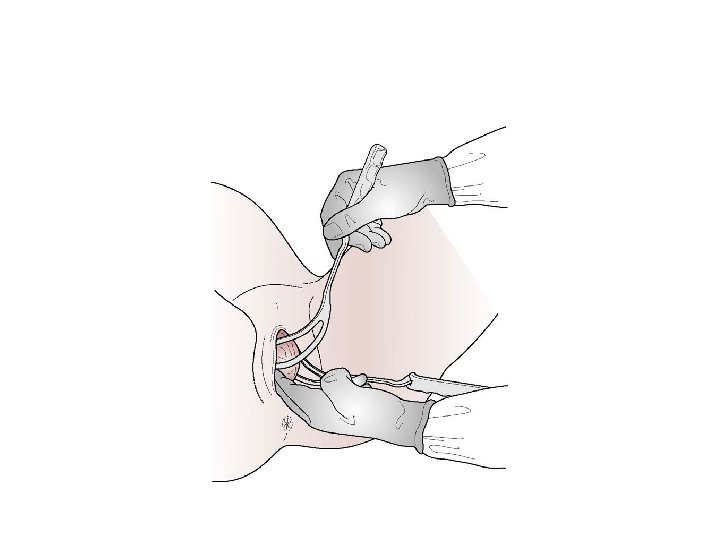
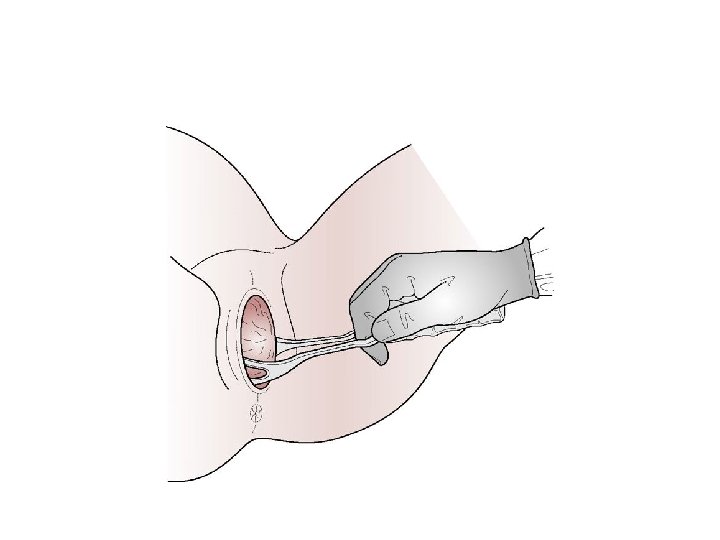
• • Characteristics of obstetric forceps - composed of two separate blades - a right and a left. -The forceps are inserted separately on each side of the head -The forceps are locked together by either an English or a Smellie lock. -Rotational forceps have a sliding lock. -The blades are spoon shaped (cephalic curve) - the blade is attached to the handle at an angle that corresponds to the pelvic curve

• Classification of obstetric forceps • -low and mid-cavity. • - Low-cavity forceps are used when the head has reached the pelvic floor and is visible at the vulva. • -Mid-cavity forceps are used when the head is engaged and the leading part is below the level of the ischial spines. • -High-cavity forceps are considered unsafe and a caesarean section will be carried out.

• • • • Types of obstetric forceps non-rotational or rotational -Adequate analgesia is required prior to their application to the fetal head. Wrigley's forceps -use when the head is on the perineum. - a short and light type of forceps, with both pelvic and cephalic curves and an English lock. - used after-coming head of a breech delivery, or at caesarean section. Neville-Barnes or Simpson's forceps used for a low or mid cavity forceps delivery when the sagittal suture is in the anteroposterior diameter of the cavity/outlet of the pelvis. They have cephalic and pelvic curves - the handles are longer and heavier than those of the Wrigley's. Anderson's and Haig-Ferguson's forceps are also similar in shape and size

• Kielland's forceps • designed to deliver the fetal head at or above the pelvic brim. • used for the rotation and extraction of the head that is arrested in the deep transverse or in the occipitoposterior position. • The blades have little pelvic curve. • The shallow curve allows safe rotation of the forceps in the vagina. • Downward traction encourages rotation of the head.


• Indications for the use of obstetric forceps • delay in the second stage of labour • fetal compromise • and maternal distress.

• Delay in the second stage of labour may be due to: • • insufficient contractions (but this is better corrected by oxytocin infusion) • • epidural analgesia • • mal-rotation of the head • • maternal fatigue. • Fetal compromise may be due to: • • prematurity • • hypoxia • • intrauterine growth restriction • • a maternal obstetric or medical condition (e. g. pre-eclampsia). • Maternal distress may be caused by: • • hypertension • • cardiac condition • • maternal exhaustion or long labour.

• Prerequisites forceps delivery • • Care of the bladder. To prevent harm or injury • • Analgesia. by epidural or pudendal block plus perineal infiltration of local anaesthetic • • Information giving and consent. The couple must be kept informed • • Paediatrician. The paediatrician or advanced neonatal practitioner may not be required at birth • • Neonatal resuscitation equipment. This must be checked and prepared in case it becomes necessary.
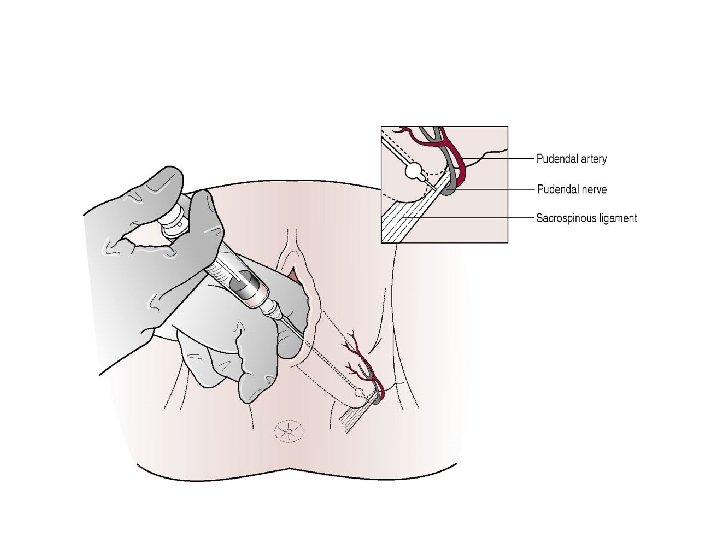

• Pudendal block • the infiltration of the area around the pudendal nerve by local anaesthetic. • The transvaginal route is used to locate the ischial spine, as the pudendal nerve emerges from vertebrae S 2 –S 4 and crosses this. • Use a pudendal block needle. • About 10 m. L of local anaesthetic, usually 1% lidocaine (lignocaine), is injected into the region just below the ischial spine -Both motor and sensory nerves are affected as both lie in this region.

• The pudendal nerve supplies the levator ani muscles, also the deep and superficial perineal muscles • It may be used to provide analgesia for the lower vagina and perineum, and is therefore used forceps and ventouse deliveries. • this technique does not harm the baby.

• • • Perineal infiltration -A local anaesthetic is used to infiltrate the perineum prior to episiotomy or suturing Technique - the presentation and position are identified - The membranes ruptured - full dilatation of the cervix - head engaged -no CPD. - Episiotomy is not routinely carried out

• • Complications OF forceps: Maternal complications include: • trauma or soft tissue damage occur to the perineum, vagina, or cervix • hemorrhage from the above • dysuria or urinary retention, which may result from bruising or oedema to the urethra • painful perineum • postnatal morbidity intervention

• • Neonatal complications • marks on the baby's face, which can be caused by the pressure of the forceps, but resolve quite rapidly • excessive bruising from the forceps • facial palsy, which may result from pressure from a blade compressing a facial nerve, and is usually temporary.

Thank you
- Slides: 30