ASSESSMENT OF ORGANIC AND NEUROGENIC SPEECH DISORDERS I

















 • 5. Sample production of same phoneme in multiple")
** • 8. Receptive and expressive lang skills • 9. Articulation—give test,")


**")

















 • Watch for expressive-receptive")


- Slides: 43
• ASSESSMENT OF ORGANIC AND NEUROGENIC SPEECH DISORDERS
I. CEREBRAL PALSY** • A. Introduction-definition (non-progressive motor disorder due to pre-, peri-, or post-natal damage) • Youtube—Charrise’s Story: My Life Journey with Cerebral Palsy (first few minutes)
Fogle, 2019—CP often results from: • Infantile hypoxia—partial or significantly diminished supply of oxygen to brain • Infantile anoxia—oxygen completely cut off
Types of CP: • Spastic: 50%; slow, jerky movements and increased muscle tone • Athetoid: 10%; slow, writhing, involuntary movements • Ataxic: 5 -10%; balance problems but normal reflexes and muscle tone • Rigid: 1%; simultaneous contraction of all muscle groups • Mixed: 30%; several types
B. Speech Problems and Their Assessment** • Oral motor—assess speech, nonspeech tasks • Feeding—sucking, chewing, swallowing • Slow DDK rates, discoordination of tongue • Resonance—nasal emission on consonants, hypernasality on vowels
• Prosody—monotone, monoloudness • Respiration—rapid breathing, waste of air, trailing off at the ends of sentences • Phonation—weak voice; strained if vocal folds are hyperadducted • Articulation—imprecise; weak pressure consonants
II. DYSARTHRIA** • A. Introduction • Neuromotor disorder affecting all systems: respiration, phonation, articulation, resonance, prosody • Due to: CP, degenerative diseases, stroke
B. Characteristics to Look for in Assessment** • Breathy respiration • Difficulty with appropriate syllable stress • Artic: imprecise, distorted consonants; weak pressure consonants
» Resonance: hypernasality • Phonation: monotone, monoloudness, often soft voice • PRAXIS tip: Festination means small, shuffling steps
III. CHILDHOOD APRAXIA OF SPEECH** • Youtube—childhood apraxia of speech 3 year old (Urban. Kowboy) • Youtube Severe Apraxia and Possible ASD (Julian)
2020 asha. org • CAS occurs in 1 -2 children per 1, 000 • Found in approximately 4% of ch referred for SSDs • Idiopathic CAS affects more boys than girls by a ratio of 2 or 3: 1
We know that: • Most ch with CAS have a family member with a speech or lang disorder • CAS has a genetic component
A. Introduction** • Inconsistent errors • Flat prosody • Difficulty sequencing sounds and syllables • Moderately to severely unintelligible
• CAS is not the result of neuromuscular weakness • Ch with CAS have impaired motor planning and programming capabilities • Unable to automatically learn motor plans necessary for rapid, accurate speech production • Better at word level than connected speech
True-False: • Childhood apraxia of speech is characterized primarily by weakness of the speech muscles and breathy speech.
B. Associated Problems • Family hx in some ch • Possible learning disability • Better receptive lang skills, ↓ expressive lang • Slow tx progress • Oral apraxia/difficulty with volitional nonspeech tasks • Slow DDKs • “Soft” neurological signs—gross & fine motor incoordination
C. Assessment—Evaluate: ** • 1. Pitch, loudness, prosody • 2. Overall intelligibility • 3. Resonance—e. g. , hypernasal? • 4. DDKs—alternating /pʌpʌ/ • and sequential motion /pʌtʌkʌ/
• CAS Assessment (continued) • 5. Sample production of same phoneme in multiple trials • 6. Ask them to produce words in both imitative and spontaneous modes • 7. Developmental hx— feeding, sucking problems? Slow lang devt. ?
CAS Assessment (continued)** • 8. Receptive and expressive lang skills • 9. Articulation—give test, administer items repeatedly to assess consistency of production • 10. Connected speech sample
One of my very favorites**: • 12. Production of polysyllabic words —have them say the words several times, check for consistency. E. g. : (words are not on test) • • • Expensive Refrigerator Buzz Lightyear’s Zurgotronic Ionblaster (ha ) Congratulations Cafeteria Computer
• Remember: inconsistency is a hallmark of CAS
IV. CLEFT PALATE (cleft is an opening in a normally closed structure)**
Youtube • LT 5 1/2 years old with cleft palate
A. Introduction-major categories** : • Isolated cleft lip
Cleft uvula alone**
Cleft of the hard palate**
Adult cleft of soft palate and part of hard palate**
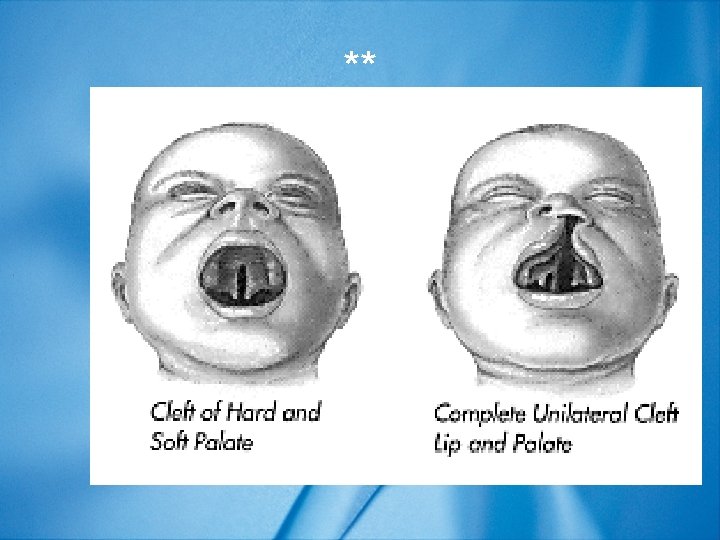
Cleft of soft and hard palate**
Combined Cleft Palate and Lip** • This can be unilateral or bilateral • Here is a unilateral cleft
Unilateral cleft of the lip and palate**
Unilateral cleft palate and lip**
Example of a bilateral combined cleft lip and palate: **
Bilateral combined**
Bilateral combined**
Fortunately, surgical repair is excellent in the 21 st century**
Surgical repair “after”**
Surgical repair “after”** • He had 5 -6 surgeries, the last of which was in 6 th grade • He is now a model and actor
B. Assessment of Patients with Cleft Palate** • Difficulty with pressure consonants (stops, fricatives, affricates) • Nasal emission, hypernasality • Compensatory errors like glottal stops hoarseness • Middle ear dysfunction (Eustachian tube), OME
Test question: • Nadia, a 7 -year old with a partially repaired cleft palate, has immigrated with her family from Jordan. She is somewhat unintelligible. Which of the following probably is/are TRUE? • A. She has difficulty with pressure consonants • B. Pressure consonants in error include stops, fricatives, and affricates • C. She probably has a severe bilateral sensorineural hearing loss • D. A, B • E. B, C
• Iowa Pressure Test (part of the Templin. Darley) • Watch for expressive-receptive lang gap • Listen for vocal pathology like hoarseness, soft voice due to strain on vocal folds or to VPI (velopharyngeal inadequacy)
C. Assessment Strategies** • 1. Work with team of professionals • 2. Help plan surgical interventions • 3. Assess intelligibility in connected speech • 4. Esp. assess production of pressure consonants in words and sentences • 5. Determine presence of hypernasality on vowels and nasal emission on consonants
Hold a mirror under the child’s nose…** • Have her prolong /i/ • Also assess pressure consonants, look for fog • Mirror should be clear if there is no hypernasality