Assessing Clients with Bowel Elimination Disorders Chapter 26

Assessing Clients with Bowel Elimination Disorders Chapter 26

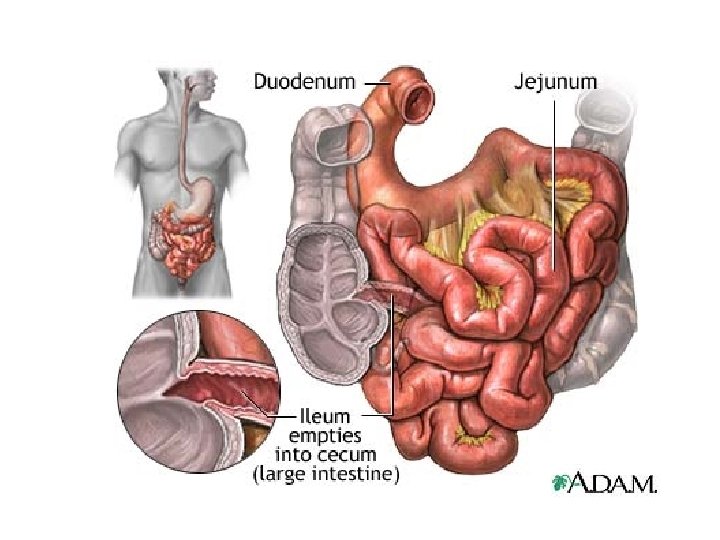
Review of Anatomy and Physiology l Small intestine – – pyloric sphincter to ileocecal junction three regions l l l – duodenum jejunum ileum Function - chemical digestion and absorption l microvilli, villi and circular folds increase surface area

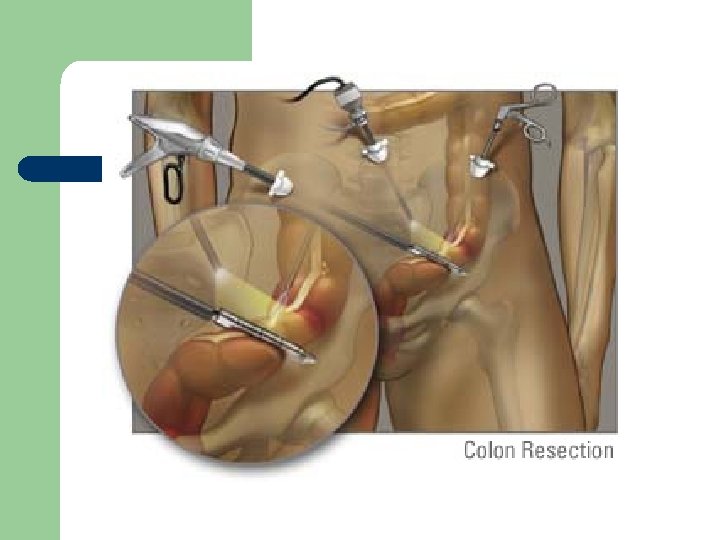
Small bowel surgery

Small intestine

Review of Anatomy and Physiology l Large intestine - colon – – – ileocecal valve to anus Cecum - first part of intestine - appendix Colon divided into 3 parts l l l – ascending transverse descending Function - eliminate undigestible food, absorb water, salt and vitamins
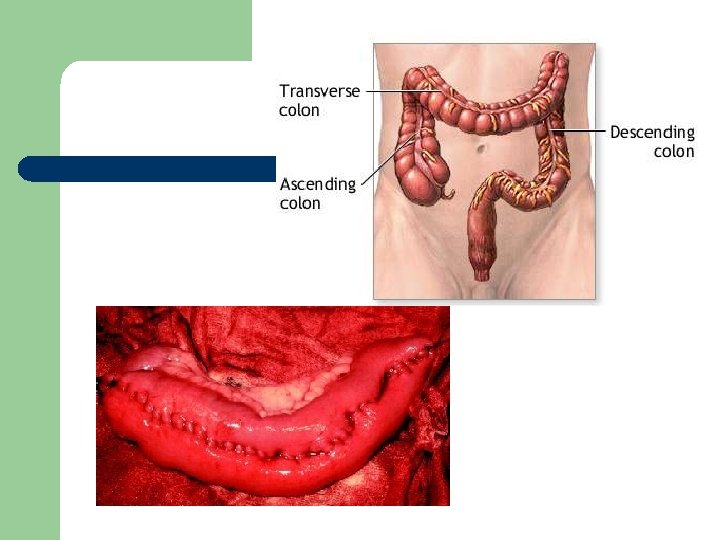

Large Intestine

Assessment of Bowel Function l Subjective – – – – onset characteristics course severity precipitating factor relieving factors associated symptoms

Sample Interview Questions l l l Can you describe the type of cramping and abdominal pain you are having? Have you every had bleeding from your rectum? Have you noticed any changes in your bowel habits?

Assessing the Abdomen l l l Inspection, auscultation, percussion and palpation as described Rectal exam - polyps Stool for occult blood – + requires further testing for colon CA or GI bleeding 2 nd to peptic ulcers, ulcerative colitis or diverticulosis

Blood and Stool l l Melena - black tarry stool Blood on Stool - bleeding sigmoid colon, rectum Blood in Stool - colon, ulcerative colitis, – diverticulitis, tumor, ulcer Stool black, hard = oral iron Strong odor = blood of high fat content – steatorrhea

Nursing Care of Clients with Bowel Disorders Chapter 26

Disorders of Intestinal Motility l Diarrhea – – l serious in the young and elderly increase in the frequency, volume and fluid content of the stool Causes – bacteria, or parasitic infections, malaborption, medications, diseases, allergies or pyschological

Diarrhea l Clinical Manifestations – – vary widely from several large watery stool to very frequent small stools result in severe electrolyte imbalances l l – hypokalemia - Low K+ hypomagnesemia - low Mg+ hypovolemia - fluid volume deficit - hypovolemic shock with vascular collapse

Diarrhea l Collaborative Care – – treat underlying cause Labs l l – stool specimen - for WBC’s, parasitic infections culture electrolytes - imbalance Diagnostic tests l sigmoidoscopy - direct exam of bowel

Diarrhea l Client prep – l Dietary management – – l consent, npo, enemas fluid replacement - gatorade, pedialyte bowel rest for 24 hours - add milk last Pharmacology – absorbents, anticholinergics, antibiotics

The Client with Constipation l The infrequent or difficult passage of stool – – l two or less BM’s per week affects elders - impaired health, medications, decrease physical activity Diagnostics – Barium enema l – - tumors, diverticular disease colonoscopy l - tumor, obstruction, take bx

Constipation l Dietary Management – – l high fiber - vegetable fiber adequate fluids Pharmacology – – – laxatives for short term use bulk form agents for long term use enemas - acute short term or as prep

Irritable Bowel Syndrome l l Disorder characterized by alternating periods of constipation and diarrhea Cause - no organic cause found – – related to food ingestion, meds. , stress, hormones looking at motor activity of the G. I. tract

IBS l Clinical Manifestations – – Colic-like abdominal pain Altered bowel elimination l – l Bloating, tenderness Labs and Diagnostics – l mucous in stool, change in frequency, straining, urgency, incomplete emptying stool specimen, colonoscopy, UGI with SBFT Dietary management – add fiber - adds bulk and water content

Bloating and Cramping

The Client with Fecal Incontinence l l Loss of voluntary control of defecation Causes – interfere with sensory or motor control of rectum and anal sphincters l l l neuro -spinal cord injury, head injury local trauma - OB tears, anal-rectal injury, surgery Other - radiation, impaction, tumors, confusion

Fecal Incontinence l Collaborative Care – – – dx made by history digital exam - poor sphincter tone treatment l bowel training program - establish regular pattern dietary changes – stimulant - coffee, suppository, digital stimulation – l surgery - colostomy
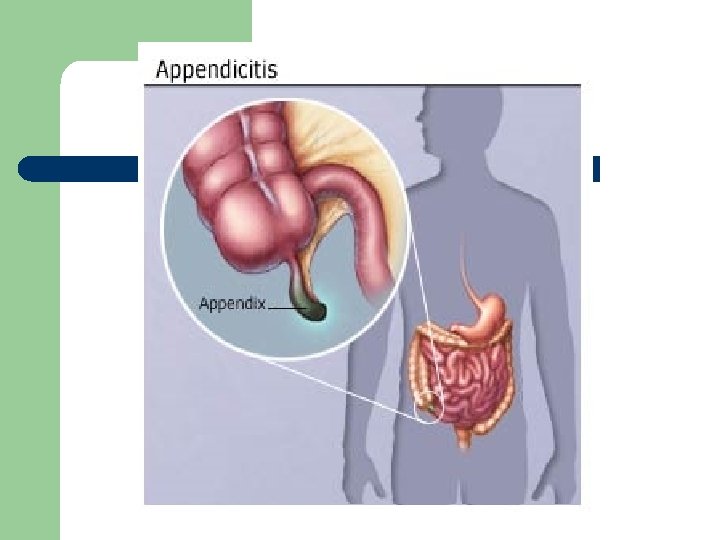

Acute Inflammatory and Infectious Disorders l Appendicitis – – inflammation of the appendix common cause of acute abd pain most common reason for emergency abd surgery most common in adolescents and young adults

Appendicitis l Simple – l Gangrenous – l appendix is inflamed but intact tissue necrosis and microscopic perforations Perforated – gross perforation and contamination of peritoneal cavity

Appendicitis l Clinical Manifestations – – continuous mild generalized upper abd pain then intensifies and localizes to RLQ l l l – – rebound tenderness - tenderness on release of pressure at Mc. Burney’s point + Rt heel tap pain What about pain medications? nausea, anorexia, vomiting, low-grade fever perforation - increased pain, temp, abscess

Appendicitis Pathophysiology l l l The appendix can become obstructed by fecalith (hard masses of feces) a stone, inflammation or parasites. As a result of the obstruction the appendix becomes distended with fluid. This increases pressure within the appendix and impairs its blood supply. The lack of blood supply leads to inflammation, edema, ulceration, and infection of the tissue. Can become necrotic and perforate if treatment is not indicated.

Appendicitis l Interdisciplinary Care – – Labs - CBC, UA, pregnancy test Diagnostic studies - abd X-ray, pelvic exam, ABD ultrasound Pharmacology - IV’s , antibiotics - third generation cephalosporin - rocephin Surgery - Appendectomy exploratory vs laproscopy
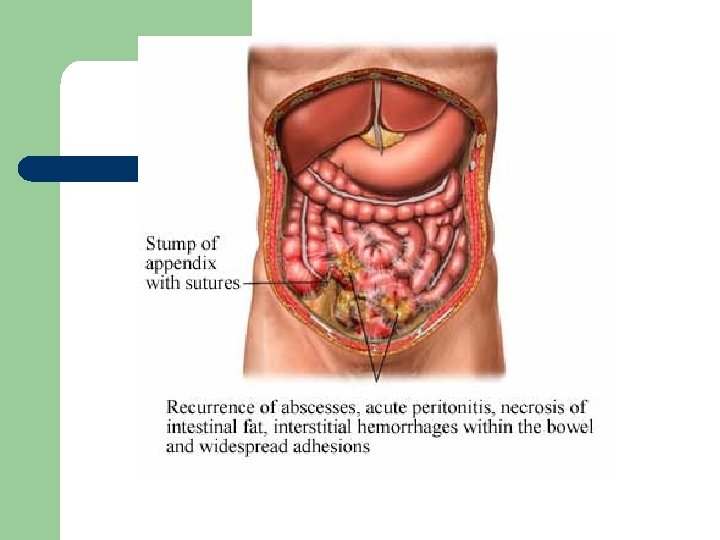

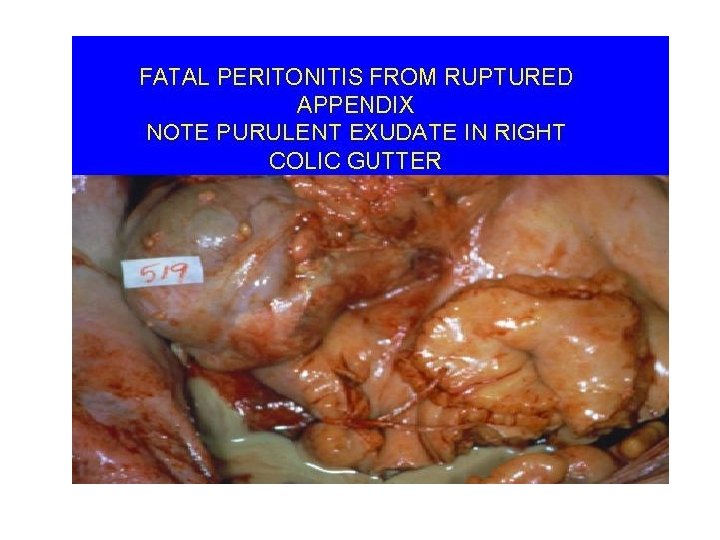
The Client with Peritonitis l Inflammation of the peritoneum - is the most significant complication of acute abdominal disorders – – perforation of appendix, diverticulum, peptic ulcer, pancreatitis or GSW bacterial infection - E coli or klebsiella

Peritonitis l Clinical Manifestations – Abdominal Effects l l – Diffuse or localized pain - rebound Boardlike rigidity diminished or absent bs distention, anorexia, nausea, vomiting Systemic effects l l fever, malaise, tachycardia, restlessness shock

Peritonitis l Labs and Diagnostics – – CBC - WBC’s with shift to the left, immature wbc out to help fight infection Blood culture - bacterial invasion into blood stream Paracentesis - obtain peritoneal fluid Abd x-ray - free air under diaphragm indicative of gastrointestinal perforation

Peritonitis - Interdisciplinary Care l Pharmacology – – l broad-spectrum antibiotics until culture report obtained narcotic analgesic, antipyretics Surgery - laparotomy – peritoneal lavage l l washing out cavity with copious amounts of isotonic soln drains - JP or pen rose, may be left open

Nursing Care - Peritonitis l NGT – l intestinal decompression Pain - abd distention and inflammation – – – assess - location, severity and type - analgesics fowler’s - minimize stress on abd structures alternative pain management - visualization, medication, relaxation

Nursing Care - Peritonitis l Fluid volume deficit – l Altered protection – l I & O, vs, wt. , assess for dehydration monitor for sign of infection, handwashing, aseptic technique for drsg changes Anxiety – potential threat to life

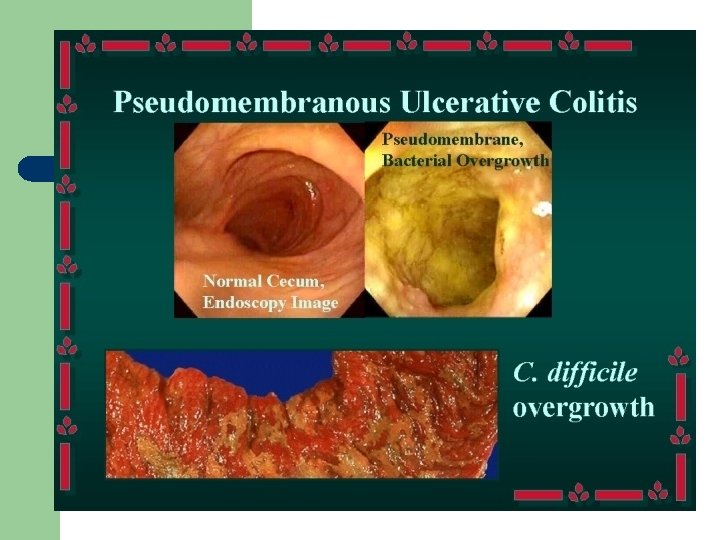
The Client with Viral or Bacterial Infection l Gastroenteritis – – – describes general GI inflammation syndrome - diarrhea, vomiting, anorexia, nausea and pain organisms - Staphlococcal, Salmonella, Shigella, Botulism - life threatening, Cholera - third world countries dx - stool culture, tx - antibiotics, rehydration

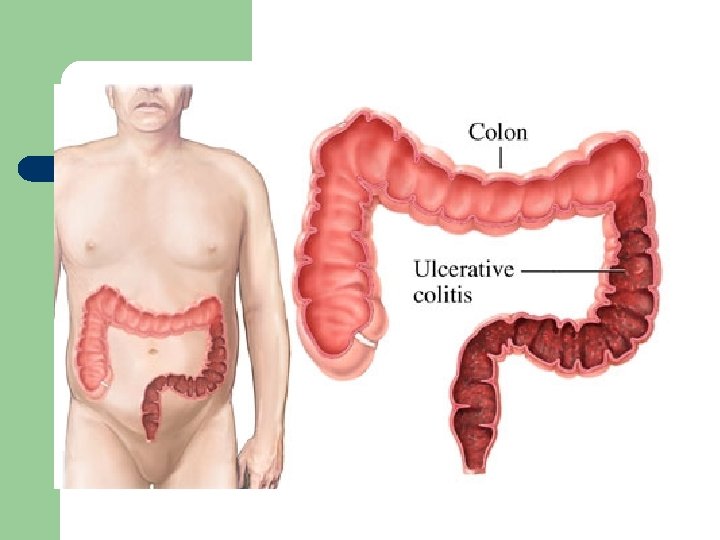
l Ulcerative Colitis – – – chronic inflammatory bowel disorder of the mucosa and sub mucosa. Affects young 15 -40 yrs old Cause l – unknown, genetic component, autoimmune, dietary factors - fiber poor foods, smoking Affects the large bowel

Ulcerative Colitis l Clinical Manifestations – – insidious onset - attack last 1 to 3 months diarrhea - 30 to 40 stools per day with blood and mucus fatigue, anorexia, generalized weakness toxic megacolon - transverse colon is paralyzed may rupture, massive hemorrhage - need colostomy
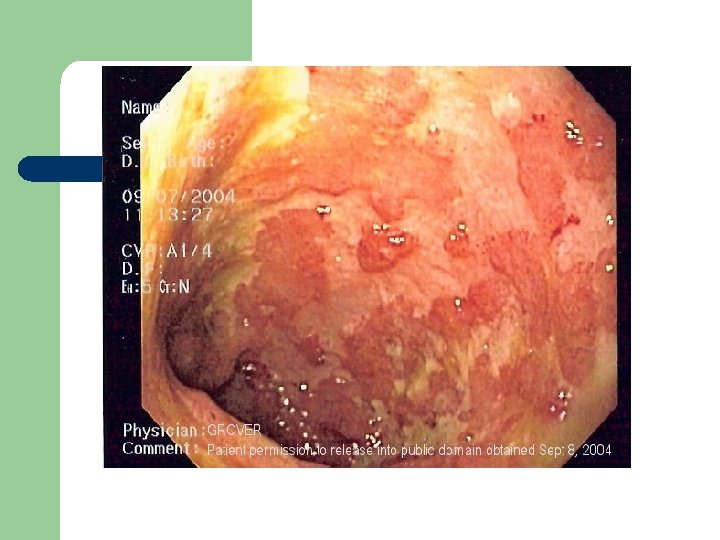

Ulcerative Colitis l Interdisciplinary Care – – – supportive treatment Dx - by sigmoidoscopy, edema, inflammation, mucus and pus Pharmacology l – Azulfidine - sulfonamide antibiotic, acts topically on colonic mucosa to inhibit inflammatory process Dietary - npo with TPN, then low residue

Ulcerative Colitis l Surgery – – l not initial treatment ileostomy Nursing Care – – relieving abd cramping emotional support teaching about illness and special needs Nsg dx. - diarrhea and body image disturbance

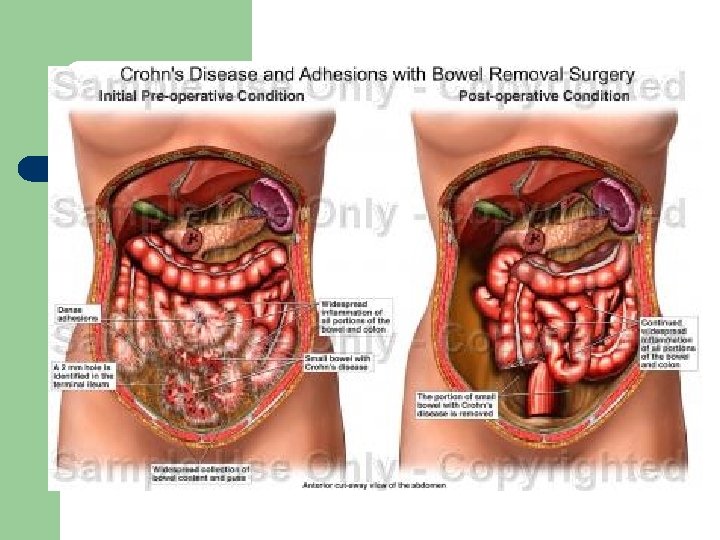
The Client with Crohn’s Disease l l l Slowly progressive, relapsing inflammatory disorder of GI tract diarrhea less severe, no blood or mucus RLQ pain, fever, malaise, fatigue affect young people 10 -30 can occur anywhere in the GI tract, patchy lesions

Crohn’s Disease l Interdisciplinary Care – l therapy is directed toward managing the symptoms and controlling the disease process Labs and Diagnostics – – – Stool specimen X-ray - UGI with SBFT - shows ulcerations, strictures and fistulas colonosocpy - bx

Crohn’s - Interdisciplinary Care l Pharmacology – – l Dietary – l same as ulcerative colitis - anti inflammatory antidiarrheal - no risk of mega colon NPO - TPN, eliminate milk Surgery – 2 nd to complications, bowel obstruction - bowel resection

Malabsorption Syndromes l A condition in which nutrients, carbohydrates, protein, fats, water, electrolytes, minerals, and vitamins are ineffectively absorbed by the intestional mucosa – – mostly disease of small intestine surgery of small intestine

Malabsorption Syndrome l Clinical manifestations – anorexia, abd bloating, diarrhea, weight loss, weakness, malaise, muscle cramps, anemia l l signs of malnutrition Celiac Disease – – hypersensitivity to gluten, protein found in cereal Tx - gluten free diet

Malabsorption Syndrome l Lactose Intolerance – – – deficiency of lactase the enzymes needed for digestion and absorbtion of lactose the primary carbohydrate in milk affects 90% of Asians, 75% of African Americans, high incidence among Jewish and Hispanic populations usually hereditary, symptoms occur in adolescence or early adulthood

Malabsorption Syndrome l Short Bowel Syndrome – from resection of significant portions of the small intestine l – CA, mesenteric thrombosis with bowel infarction, Crohn’s disease or trauma Treatment l l frequent small, high caloric and high protein meals multivitamin and mineral supplements

Neoplastic Disorders l Polyps – – is a mass of tissue that arises from the bowel wall and protrudes into the lumen occur most often in the sigmoid colon and rectum 30% of people over age 50 have polyps most are benign, some have potential to become malignant - are removed

Polyps l Interdisciplinary Care – – – Diagnosis made by barium enema and sigmoidoscopy or colonoscopy Follow-up recommended because polyps tend to recur Consider a “silent” disease - few or no symptoms with significant risk of CA

The Client with Colorectal Cancer l l l Malignant tumor arising from the epithelial tissues of the colon or rectum 2 nd leading cause of cancer death in Western countries long term survival rate is only 35% occurs more in males than females occurs after age 50

Colorectal Cancer l Risk Factors – – – – over age 50 polyps in colon or rectum cancer elsewhere in the body family history ulcerative colitis or crohn’s disease radiation, immunodeficiency disease dietary - high fat, high caloric, low Ca+ and fiber

Colorectal Cancer l Clinical Manifestations – – – no symptoms until it becomes advanced slow growth pattern - 5 -10 yrs. for symptoms to develop bleeding change in bowel habit - diarrhea or constipation pain, anorexia, weight loss - advance disease

Colon Cancer

Colorectal Cancer l Interdisciplinary Care – establish dx - colonoscopy – surgical intervention – adjuncts of chemotherapy and radiation

Colorectal Cancer l l Surgical resection of tumor, adjacent colon and regional lymph nodes Dukes Staging – – Stage A - confined to bowel wall Stage B - penetration of bowel wall Stage C - lymph node involvement Stage D - distant metastases

Permanent for tumors of rectum or sigmoid colon l Hartmann pouch – temporary – the distal portion of the colon is left in place and sewn shut

Double Barrel colostomy

Nursing Care of the Client Having Bowel Surgery l Pre-operative – – – consent assess level of understanding bowel prep l l oral and parental antibiotics cathartics and enema to reduce risk of bowel contamination

Nursing Care of the Client Having Bowel Surgery l Post-operative Nursing Care – Routine post-op care l l l – – – vital signs, turn, cough, deep breath q 2 hrs I & O - NGT drainage, surgical drains assess for post-op hemorrhage Assess for bowel sounds and distention Provide pain relief Assess resp. status - teach to splint

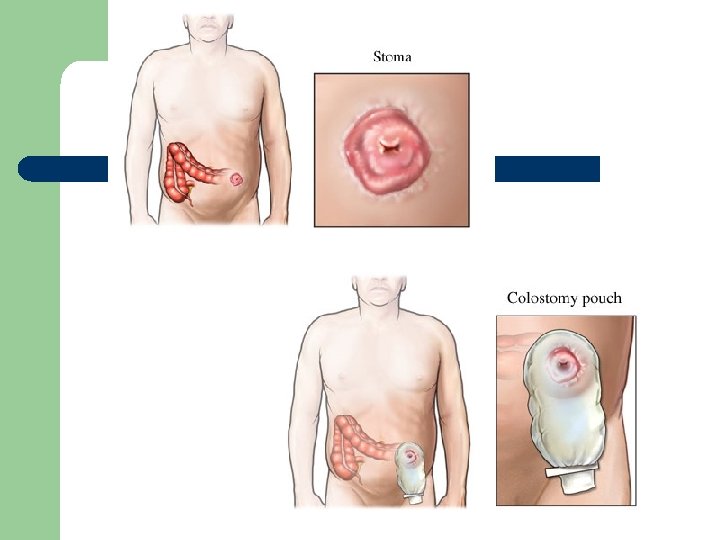
Nursing Care of the Client Having Bowel Surgery l Post-operative care – – – Assess position and patency of NGT Assess stoma - color, size, check pallor Assess stoma out-put - usually bright red initially then changing to clear greenish yellow by day 2 -3 Encourage ambulation, this stimulates peristalsis teach colostomy care

Nursing Care of Clients Having Bowel Surgery l Effects of ostomy on Body Image – – – adjust to loss of body organ and dx of cancer show acceptance of client and ostomy concerned over the affect of cancer develop a trusting relationship listen actively ostomy, cancer support groups, social services

Colostomy Surgery

Case Study - Colorectal Cancer l W. C. , 65 yr old male, retired railroad employee, husband father of 3 grown children. Has 3 month history of small amount of blood and mucus in stool. Has a sensation of rectal pressure and has notice his stool has changed in diameter, now is pencil thin.

l l l Physician palpates a tumor in the rectum. Colonoscopy and bx confirm adenocarcinoma W. C. is scheduled for a abdonminalperitoneal resection and sigmoid colostomy

l His wife has many questions and asks, why does the colostomy have to be permanent? l Why does he need erythromycin and neomycin tablets? l She then asks, is he going to be ok?

Physician Orders l Explain the rationale behind these orders – – – Insert NGT and connect to low intermintent suction Insert foley catheter Routine post-op v. s. , OOB tonight See PCA order sheet (M. S. 1 mg q 10 min, up to 10 mg every 4 hours) NPO

Nursing Interventions l Explain the rationale behind these interventions – – – establishing a therapeutic relationship assessing patency and position of the NGT assessing respiratory status assessing b. s. assess stoma and stoma output teaching to splinting the incision

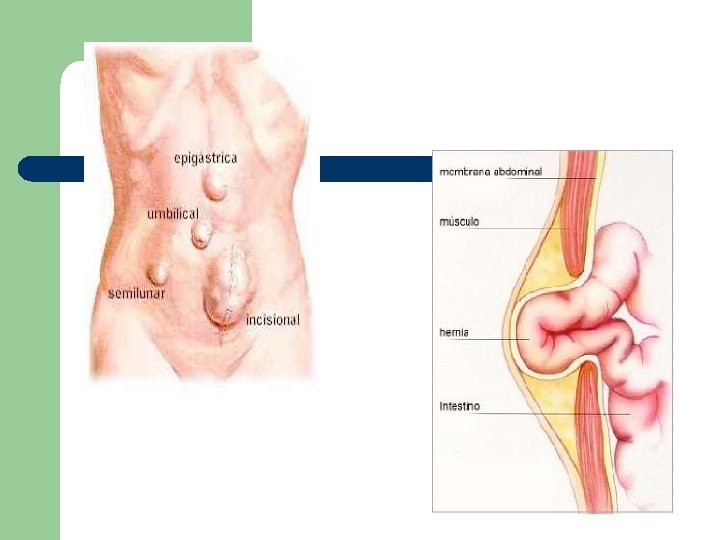
Structural and Obstructive Disorders l Hernia – – protrusion of an organ or structure through a defect in the muscular wall Inguinal hernias l l l 75% of all hernias cause by improper closure of the tract that develops as the testes descend into the scrotum before birth bulge at inguinal cannal reducible - contents of the sac return to abd cavity strangulated hernia - blood supply is compromised

Structural and Obstructive Disorders l Umbilical hernias – – l occur more frequently in women obesity, mult. pregnancies, prolonged labor tend to enlarge steadily strangulation is common Incisional or Ventral hernias – occur at previous surgical incision

The Client with an Intestinal Obstruction l l Occurs when intestinal contents fail to be propelled through the lumen of the bowel Small intestine obstruction – – ileum of small intestine most common site Mechanical Obstruction l – physical barrier, tumor or scar tissue Functional Obstruction - paralytic ileus l peristalsis fails

Bowel Obstruction

The Client with an Intestinal Obstruction l Clinical Manifestations – – – cramping, colicky abdominal pain, can be intermittent or increase in intensity vomiting high-pitched tinkling bowel sounds - reflects the bowels attempt to propel contents past the obstruction later stages - absent bowel sounds electrolyte imbalance - hypovolemia - shock

The Client with an Intestinal Obstruction l Large Bowel Obstruction – – – usually occurs in sigmoid colon cancer most common cause Clinical Manifestations l l l abdominal pain and constipation abdomen is distended and tender to palpation Treatment for Bowel Obstructions – NGT - functional surgery - mechanical

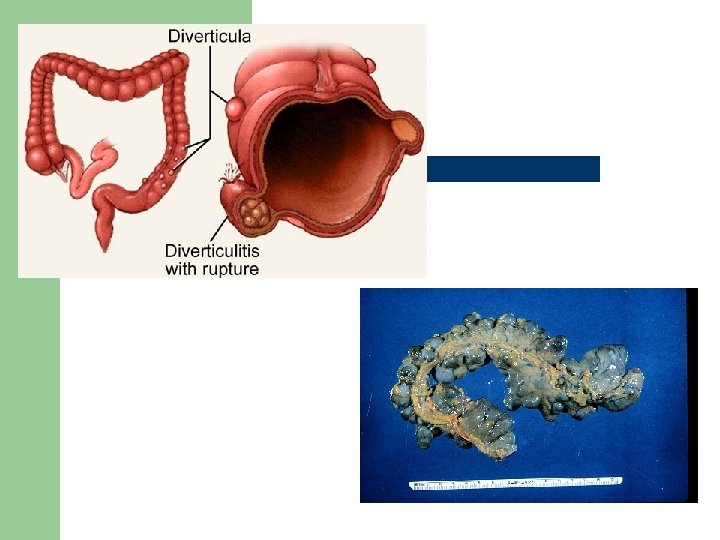
Diverticulitis

The Client with Diverticular Disease l Diverticula – – acquired saclike projections of mucosa through the muscular layer of the colon 90 -95% occur in the sigmoid colon increased incidence in US, Australia, United Kingdom and France related to cultural factors - diet high in refined foods and low in fiber

The Client with Diverticular Disease l Diverticulosis – – l the presence of diverticula 80% are asymptomatic Clinical Manifestations – – left-sided abd pain, constipation and diarrhea narrow stools, occult bleeding

The Client with Diverticular Disease l Diverticulitis – – l inflammation and microscopic perforation of diverticular mucosa undigested food becomes trapped, blood flow is impaired - leads to abscess or peritonitis Interdisciplinary Care – – Chronic diverticular disease - dietary changes Acute diverticulosis - bowel rest, antibiotics, eventually surgery

Anorectal Disorders l The Client with Hemorrhoids – – hemorrhoidial veins become weak, distended, develop varices - cause is straining, pregnancy also increases intra-abdominal pressure internal or external l l bleeding, bright red, unmixed with stool pain associated with thrombosed or ulcerated

The Client with Hemorrhoids l Interdisciplinary Care – – conservative therapy - diet, increase fiber, fluids, bulk forming laxative, Preparation H surgery l l l sclerotherapy - inject chemical irritant to induce inflammation - fibrosis - scarring rubber band ligation - rubber band placed snugly around - necrosis - slough cryosurgery - necrosed by freezing with probe

The Client with Hemorrhoids l Nursing Care - post-op – – – inspect rectal dressing for bleeding pain management - position of comfort - side lying ice pack over rectal drsg sitz bath tid and prn bowel movement meds - analgesics, stool softeners

The Client with Anorectal Lesions l Anal Fissure – l Anorectal Abscess – l bacteria invades pararectal space - I & D Anorectal Fistula – l ulcers of the epithelium of the internal sphincter tunnel or tubelike tract - leaks stool Pilonidal Disease - chronic draining sinus
- Slides: 92