Assertive Community Treatment Angela L Rollins September 14

Assertive Community Treatment Angela L. Rollins September 14, 2018 Nevada

Getting Started… Ø Introductions Ø Overview of Training Ø Other housekeeping Items?

Training Overview Ø Why ACT? Ø What is ACT? Ø ACT Team Structure and Roles Ø ACT Philosophy Ø ACT Team Processes Ø Rural ACT Fidelity item references throughout

Training Overview Ø Why ACT? Ø What is ACT? Ø ACT Team Structure and Roles Ø ACT Philosophy Ø ACT Team Processes Ø Rural ACT

Why ACT? Ø History of ACT Ø Who does ACT serve? Ø ACT Research
 Ø Developed during 1970 s Ø Revolving Door")
Initial Development (Stein & Test, 1980) Ø Developed during 1970 s Ø Revolving Door Ø “Hospital without Walls” Ø Experimentally demonstrated its effectiveness

Typical Admission Categories Ø Frequent psychiatric admissions Ø Homeless or unstable housing Ø Treatment nonadherence Ø Frequent use of emergency rooms Ø Dual diagnosis (SMI + substance abuse) Ø Legal problems Ø Discharge from long-term hospital Item O 1: mission-driven criteria

ACT Admission Process Item O 2: slow and thorough engagement Ø Initial referral screening Ø In-person assessment to confirm (TL/clinician) Ø First 90 days or so – comprehensive assessment and treatment planning Ø Engage, engage around what the consumer wants or is missing in life • housing and other transitions will take time and effort so intake rates urged to remain low

ACT Effectiveness Across 25+ Studies Ø Large impact on: Hospital use – 61% reduction in days • Housing • Retention in treatment Ø Moderate impact on: • Symptoms • Quality of life •

ACT Effectiveness ØWeaker impact on: • Employment • Substance use • Jail and legal problems • Social adjustment

Future Research & Practice of ACT Ø Integrating other EBPs on ACT Teams Ø Expanding recovery-focus Ø Examining effectiveness for special populations, adapt after full fidelity implementation l “Adapting” usually means adding rather than subtracting for special populations
 Ø Depends on Who Is Served ACT saves")
When Is ACT Cost-Effective? Latimer (1999) Ø Depends on Who Is Served ACT saves money when serving heavy users of psychiatric hospitals (>50 hospital days in prior year) Ø And How It’s Implemented l ACT saves money if program shows fidelity to model l
 Followed Model Closely Yes")
Fidelity Matters 3 -Year Follow-up (Mc. Hugo et al, 1999) Followed Model Closely Yes No Consumer dropped out of treatment 15% 30% Substance use remission 58% 13% Hospital admissions 2. 87 4. 69

Training Overview Ø Why ACT? Ø What is ACT? Ø ACT Team Structure and Roles Ø ACT Philosophy Ø ACT Team Processes Ø Rural ACT

ACT is a Way of Organizing Services… As a model, ACT is an effective way to deliver structured, intensive services (S 4, S 5) to meet the multiple, individualized needs (O 3) of consumers as they increase their involvement in the community in roles that they define as important and meaningful.

Some Basic Principles of ACT Ø Multidisciplinary team approach/shared caseload (H 2, H 7 -H 11, S 10) Ø Integration of all services (H 2, H 3, H 11, O 3, S 9) Ø Low client-staff ratios (H 1) Ø Intensive, yet flexible level of service (S 4, S 5 + H 3 meetings to flex + S 2 – goal is to retain + H 11) Ø Locus of contact in the community (S 1) Ø Assertive outreach (S 3, but also H 1, H 11, O 4, S 2, S 4, S 5, S 6) Ø Ready access in times of crisis (O 4, O 5, H 11) Ø No arbitrary time limits on services (O 7)

What ACT is NOT A sub team of a larger team with mixed caseloads of ACT and non-ACT clients (O 1) Ø Individual caseloads (H 2) Ø Responsibilities for treatment are outside ACT (H 7 -H 10; Ø O 3 -O 6 Traditional psychiatry role (i. e. , med checks, occasional interactions with team members) (H 3, H 7) Ø Brokered services (O 3) Ø Day treatment (O 3) Ø Case management for persons in group homes (O 3) Ø Traditional MH team (i. e. , weekly meetings, limited backup, informal information sharing) (Lots but H 3, H 11) Ø
 l Take a look")
Fidelity Scale Ø Dartmouth Assertive Community Treatment Scale (DACTS) l Take a look

Training Overview Ø Why ACT? Ø What is ACT? Ø ACT Team Structure and Roles Ø ACT Philosophy Ø ACT Team Processes Ø Rural ACT

Surveying the audience…

Typical ACT Team Staff Members Ø Team Leader Ø Psychiatrist Ø Addiction Specialist Ø Employment Specialist Ø Peer Recovery Specialist Ø Nurse Ø Mental Health Professionals/CMs Ø Therapist/Social Worker/Psychologist Ø Administrative Help

Teamwork looks like… ACT brings specialists together in a cohesive team approach Ø No silos operating in tandem (more than H 2) Ø Sharing information daily (H 3) Ø Joint treatment planning – Individual treatment teams (ITTs) for tx planning on large teams Ø How to work together to address barriers/goals of the client Ø See client with a holistic perspective – each team member might offer a unique voice Ø 80% rule of thumb for role performance; less for rural teams Ø

Team Leader Ø Direct the day-to-day clinical operations of the team l l Ø provides regular group and individual clinical supervision scheduling staff work hours to assure appropriate coverage lead daily team meetings & treatment planning meetings continuously evaluate status of all consumers & do appropriate coordination of treatment to meet their changing needs Direct & coordinate the consumer admission & assessment processes l l l schedule admission interview assign the individual treatment team (ITT) Supervise, direct, and coordinate completion of the comprehensive assessment/reassessment of each consumer Participate in staff recruitment, interviewing, hiring, orientation, performance plans Ø Supervise the medical record documentation to ensure quality and accuracy Ø
 can mean…")
Team leader as player-coach Ø 50% time in direct services (H 4) can mean… l l l Shadow staff in vivo for supervision Serve as the second staff member in double team visit for aggressive consumers (assessment and safety) Initial assessment contacts Provide counseling (esp on small teams) – IMR, some SUD counseling, CBT “ 50%” means half of the typical direct services another team member is expected to provide

Psychiatrist for all consumers on the ACT team Ø Ø Ø Along with team leader, is the clinical leader for the team Conduct psychiatric assessments, including MSE, psyc. history, establishing DSM IV diagnoses Regularly assess consumers & prescribe psychotropic medications (see each consumer at least monthly) via office AND home visits Educate consumers & their families regarding medications/symptoms/illness/side effects Collaborate with team RN(s) in assessing physical health & coordinating medical and psychiatric treatment Provide on-site crisis assessment & management & collaborate with acute & long-term inpatient providers

Substance Abuse Specialist Ø Assessment of consumers’ substance use status l l Comprehensive and ongoing assessments Assess stage of substance abuse treatment recovery Harm reduction and stagewise philosophy over traditional abstinence-only philosophy with lots of confrontation (S 9) Ø Provide stage-wise individual (S 7) and group (S 8) interventions (both in office and in community) to develop trusting relationships to enhance successful substance abuse outcomes Ø l For engagement groups (and individual tx) • some savvy SA specialists use IMR to focus on consumer wants/goals/needs rather than reducing use • “Life group”, “Goals group”, “Coping group” l MI: goals are the fodder for engaging consumers around risky substance use • what are the goals and what gets in the way?

SA specialist cont’d Ø Cross-train other ACT staff in talking about substances of abuse Ø Provide supportive case management & ADL services to build relationships and meet basic consumer needs Ø Participate in daily team mtgs. , treatment planning mtgs. , and ITTs for those working with SUDs

Employment Specialist Ø Ø Provide individual vocational-supportive counseling to enable clients to identify vocational strengths and problems, establish vocational/career goals & plans to reach them, & recognize & target symptoms of mental illness that interfere with work Engage consumers around the ACT team’s ability to help them go back to work! Provide benefits counseling-planning for how benefits and income may change (Soc. Security, Medicaid…) Job development based on client’s needs, abilities, and interests l Teach job-seeking skills (resumes, interviews…) if specific to a particular job! (no job skills groups, pretty please) Perform job coaching, problem-solving, and support on and off the job site Ø Coordinate with state vocational rehab. & other employment services Ø Participate in daily team mtgs. , treatment planning mtgs. , and ITTs Ø Graduating consumers too quickly (O 7) might omit the many benefits of the ES on ACT teams. Ø

Peer Recovery Specialist Team CEO - Chief Engagement Officer Ø Help consumers aspire to roles which emphasize their strengths via Ø l l Ø sharing their first hand experiences with their own recovery, mental health treatment offering hope and reassurance, especially for skeptical consumers Provide services and interventions to consumers which focus on recovery from their illness (IMR curriculum is perfect for peers to deliver!) l l l education about mental illness, symptoms teaching coping skills to manage symptoms, stress building social supports using medications effectively reducing relapses

Peer specialist cont’d Ø Full-fledged team member means l l Paid Able to document like other team members Daily team meeting Treatment planning meetings and ITTs Ø NOT…. l l l Van driver Volunteer Hanging out periodically or running a group only

Psychiatric Nurse Ø Ø Ø Assess overall physical health of consumers l As part of comprehensive assessment & on an ongoing basis Direct, coordinate, & provide appropriate physical health treatment l Build relationships with medical providers in the community l Provide education & information to other team members l Accompany consumers to medical appointments, facilitate medical follow up Provide education to consumers, families, and staff about mental illness, physical health, medications Take lead role in coordinating and providing the team’s medication administration services Participate in daily team meetings, treatment planning meetings, & ITTs Provide on-call crisis interventions and back up according to team’s policy

Case Manager/ Mental Health Professional Ø Ø Ø Provide in vivo case management for team consumers including coordinating and monitoring services l Act as liaison/build relationships with community agencies and families l Advocate on consumers’ behalf for resources, access to services Provide in vivo ongoing assessment of and assistance with consumers’ Activities of Daily Living (ADLs) Conduct comprehensive assessments/reassessments Assume primary responsibility for developing, writing, implementing, & revising consumer treatment plans, in conjunction with ITTs Participate in daily team mtgs. , treatment planning mtgs. , and ITTs Perform shift management & on-call crisis intervention

Therapist/ Social Worker/ Psychologist The therapist takes the lead in providing structured 1: 1 and group therapy interventions which are focused on everyday problem solving strategies, often cognitive behavioral in nature. Ø Counseling services can be provided in the community or consumers’ homes, as well as the office setting Ø Cross train other staff members on the use of CBT & other counseling skills Ø

Administrative Professional There is no DACTS fidelity item but there should be! Ø Large teams – absolutely essential Ø l TL can delegate some team coordination items and spend more time as player-coach Track and schedule treatment planning Ø Billing and fidelity process item tracking Ø Follow-up on documentation for Medicaid, SS, housing, and other resources Ø Answer the phones (if no shift manager) Ø

Training Overview Ø Why ACT? Ø What is ACT? Ø ACT Team Structure and Roles Ø ACT Philosophy Ø ACT Team Processes Ø Rural ACT

ACT Philosophy Ø Recovery Ø Expectations Ø Stress Vulnerability Model

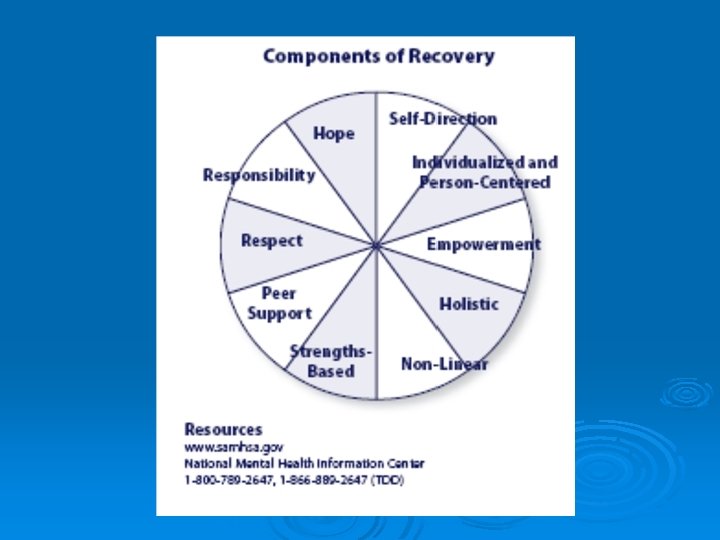
Recovery: SAMHSA* Consensus Statement “Mental health recovery is a journey of healing and transformation enabling a person with a mental health problem to live a meaningful life in a community of his or her choice while striving to achieve his or her full potential. ” *SAMHSA: Substance Abuse and Mental Health Services Administration www. samhsa. gov/

QUESTION: Where do you feel a tension between ACT and recoveryoriented care?

Recovery orientation on a continuum High Low Mixed 40

Critical Ingredients of Recovery. Oriented ACT Ø Four ingredients identified from a research project (“Recovery Oriented Profiles” from interviews and observations) 1. Team culture 2. Team structure 3. Environment 4. Process of working with consumers Ø Differentiated high from low recovery oriented teams 41

Critical Ingredient: Team Culture Ø Trusts Consumers l l Assume consumers can handle responsibilities (e. g. , money, medications) Staff view their role “not as parents” Ø Positive Expectations for Consumers l Staff believe consumers can achieve their goals and graduate Ø Strength-based/Respect Consumers l Celebrate consumer success, lack of judgment/labels Ø Team Cohesion & Respect for Each Other 42

Critical Ingredient: Environment Ø Visual cues endorsing recovery principles Posters about recovery, including team mission Vs. l Separate bathrooms, signs with rules for consumers, locked door with window for medication delivery l 43

Critical Ingredient: Team Structure Peer specialist on team Team leader endorsed recovery concepts Clinical skills (motivational interviewing, educational techniques) Other evidence-based practices integrated (IMR, SE, IDDT) High Recovery Oriented Team Low Recovery Oriented Team Yes No Yes Some (SE & IDDT) 44

Critical Ingredient: Process of Working with Consumers Ø Who makes the decisions about treatment? l Consumers (consumer goals drive treatment) vs. Staff Ø When does the team step in? l l When consumer is at risk and/or after other attempts have been made vs. Right away How is risk defined Ø How does the team step in? l Process of discussions with consumer and team vs. With external controls 45

Testing our hope/optimism How many of the consumers I work with: Will be able to achieve personal goals? Will be able to work in a competitive job (in the community, for real wages)? • Will be able to pursue spiritual/religious activities? • Will be able to have satisfying intimate relationships? • Will be able to live in their own apartment or home? • •

Evaluating our Beliefs About Consumers’ Ability to Recover What are our fears about change? Ø Combating what we’ve already been taught/learned. Ø Moving beyond “compliance”, “stability” and/or “maintenance” Ø What personality characteristics do we bring to the consumer/staff relationship that may have an impact? Ø Looking at and navigating through agency and team practices, climate, expectations, and dynamics. Ø

ACT Philosophy Ø Recovery Ø Expectations l Video l Discussion Ø Stress Vulnerability Model

ACT Philosophy Ø Recovery Ø Expectations Ø Stress Vulnerability Model

Stress-Vulnerability Model Biological Factors Vulnerability Psychiatric Symptoms Stress Impairment
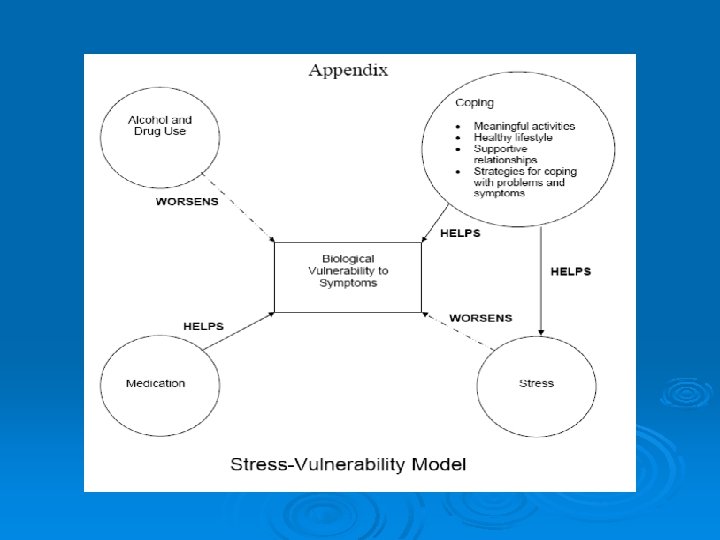

Implications for Assessment & Intervention Ø Address multiple entry points Ø Provide practical assistance so impairment will not contribute to stress Ø Reduce exposure to stress Ø Reduce sensitivity to stress Ø Increase factors that make it easier to cope with stress (innate and developed strengths) Ø Reduce psychiatric symptoms

Training Overview Ø Why ACT? Ø What is ACT? Ø ACT Team Structure and Ø ACT Philosophy Ø ACT Team Processes Ø Rural ACT Roles

Team Processes Ø Admissions Ø Engagement Ø Comprehensive Assessment Ø Person-centered treatment planning Ø Implementation of the plan Ø Addressing Ethics

ACT Admission in Nevada? Ø Medicaid eligibility documentation? Ø Focus on those who are most likely to benefit from ACT and are of most interest to state planners? Ø Baseline data collection to track progress over time?

Where do you get referrals? Ø Internal Recruiting l Ex: Build in regular meetings with inpatient unit or outpatient program Ø External Recruiting l l Outreach with consumers Outreach with other stakeholders • Busy urban teams may sit back and wait for referrals • Other teams may do some case finding, depending on what contracts and requirements are in your state

Elements of Admission Process Ø Receive referral Ø First client interview Ø [Team discussion – last 5 -10 mins of a daily team meeting] Ø Further information gathering Ø Team decision (could be 30 day assessment if feasible in your system– operating on a preliminary approval)

Engagement: Getting Started Ø Get to know the person l Understanding his or her experience with mental illness and mental health services Identify and address most pressing needs Ø Build TRUST Ø l l l With TEAM, not just with individuals Peer or another specialist who matches up well with what the consumer wants can lead it though – make the “pitch” Be prepared to hear disgruntled accounts of past service experience and compare/contrast with ACT Be creative and individualize Ø Patient and persistent Ø Engagement is both an initial and ongoing process Ø

Challenges to Engagement Ø Symptoms Ø Past negative experiences with the mental health system Ø Locating the consumer Ø Beliefs about mental illness

Assertive Engagement and Recovery Ø Balance is key Ø External controls examples: l l l Team as rep payee Outpatient commitments Daily medication administration • Thoughtful, judicious use is best Ø Creative engagement examples: l l l Getting physical healthcare needs met Getting a place to live Getting a job or an income

Ongoing Comprehensive Assessment Ø Ø Ø Contributes to the team’s understanding of the consumer and his or her environment Completed during the 30 days covered by the initial plan Primary responsibility for completion lies within the Individual treatment team (ITT) assigned Assessment takes place in community settings where contact with the consumer occurs Information gathered while also working with the consumer to meet initial needs Includes psychiatric/social functioning history timeline

Areas of Comprehensive Assessment Ø Psychiatric hx, mental status, diagnosis, and narrative Ø Physical health Ø Drug and alcohol use Ø Social development and functioning Ø Activities of daily living Ø Education and employment Ø Family relationships Ø Psychiatric/social functioning

Sources of Information Ø Consumer Ø Treatment provider records Ø Criminal justice system records Ø Family Ø Employment records Ø School records Ø Observation and clinical experience

Challenges Ø Wrong agenda – i. e. , filling out forms Ø Collecting the information Ø Time (at first) Ø Resistance to doing something different Ø Thinking you already know the consumer Ø Thinking assessment is a static process

Consumer-Focused Treatment Planning Ø Identify what is important to the consumer, in terms of goals and objectives. l Ø Build on consumers’ strengths Responsibility of ITT to write plan with consumer l l Incorporate findings from comprehensive assessment Schedule specific team interventions to support the plan--who will do what, when, how often

Identify what is important to the consumer Have you ever heard consumers say they want to: Ø verbalize understanding of their illness? Ø interact appropriately with peers? Ø attend a sheltered workshop? Ø comply with treatment? Ø take their psychiatric medications as prescribed?

Or is it more likely a consumer may want to: • Live in an apartment • Get a car • Meet some men/women • Live in a house • Get a job • Save money • Get a driver’s license • Visit family • Take a vacation • Go to a restaurant

Consumers’ Goals “in their own words” Ø “Find a doctor to get rid of germs that the Sheriff’s Department infected me with” Ø “Get some money so that I do not have to eat out of trash cans and sell drugs for food” Ø “Eat three meals a day” Ø “Stay out of jail and the hospital because people are out to get me” Ø “Have a good place to live for a while” Ø “Earn money in order to get things that I want”

Foci of Treatment Plan Ø Consumer Goals Ø “Entry Points” of stress-vulnerability model l Factors related to stress l Psychiatric symptoms l Impairment due to symptoms l Problems due to impairment Ø Stage of Change

Components of a Quality Treatment Plan Evidence of Consumer Involvement Ø Content of Plan Itself: Ø l l Developed on basis of comprehensive assessment Problem/needs statements focus on how consumers’ functioning is impacted Goals & objectives are measurable, achievable, time-limited, & individualized Specific, detailed staff interventions: who will do what, when, and how often (adapted from “Checklist for Quality Treatment Plan Development & Reviews”, ACT Center of Indiana, 2004)

Treatment Plan Example: Tonya—Problem & Goal #1 Problem/Need: Tonya is currently living in a shelter. She has been there for 15 days and is aware that she can live there for a maximum of 90 days. She has had her own apartment 4 different times, but reports she has been evicted for not paying her rent, as well as problems with visitors she has let into her apartment. Goal: “I want to find a safe place to live & not get kicked out again. Objective: (1) Tonya will be able to identify 5 housing resources that are available to her within 2 weeks. Interventions: (1) Team staff will review with Tonya housing assistance programs in the community, as well as help her access housing listings, newspaper ads, etc. Objective: (2) Tonya will find an apartment and move in within 60 days. Interventions: (1) Team staff will assist Tonya with talking with landlords, visiting potential apartments, and filling out applications. (2) Team staff will assist Tonya in accessing needed household items and furniture as she prepares to move into her apartment. Continued on next slide…
 Tonya will demonstrate her budgeting skills")
Tonya: Problem & Goal #1 cont. Objective: (3) Tonya will demonstrate her budgeting skills as evidenced by paying rent and related utilities on time for 3 months. Interventions: (1) Team staff will work with Tonya weekly to assist her in creating a monthly & weekly budget. (2) Team staff will assist Tonya in opening and learning to maintain/balance a checking account. Objective: (4) Over the next 3 months Tonya will identify the dangers of letting others into her apt. , as evidenced by verbalizing the possible dangers and actions she can take to avoid them. Interventions: (1) Weekly 1: 1 with team staff for social skills training, with focus on assertiveness, keeping herself safe, & getting back to doing activities and things she enjoys outside her home.

Tonya-Problem & Goal #2 Problem/Need: Tonya has an extensive history of substance use. She is unsure if this use has any connection to her feeling unsafe and worried about others being out to get her. She states that she does have more problems with her thoughts and sleep when she is using drugs. Tonya has a history of trading sex for money to purchase drugs. She reports that she currently uses alcohol and crack cocaine, and that these two help “drown out the voices so I won’t hurt myself and I feel better”. In the past she has used LSD, PCP, marijuana, amphetamines, and tranquilizers. Goal: “To check out if using drugs is making things worse for me. ” Objectives: (1) Within the next month Tonya will identify 5 ways that using substances may have affected her life. Interventions: (1) 1: 1 with SA specialist (motivational interviewing, or MI) 2 x per week. Other team staff to use MI during other contacts to assist with the change process. (2) attend “achieving my goals” group [persuasion] 2 x per week with SA specialist Continued on next slide…
 Within the next month Tonya will")
Tonya: Problem & Goal #2 continued Objective: (2) Within the next month Tonya will identify one or more things she views as being potential benefits from reducing or eliminating the use of substances. Interventions: (1) 1: 1 with SA specialist (motivational interviewing, or MI) 2 x per week. Other team staff to use MI during other contacts to assist with identifying potential benefits. (2) attend “achieving my goals” group [persuasion] 2 x per week with SA specialist Objective: (3) Within 3 months Tonya will develop a list of alternative options, activities, coping skills she can choose from to help her feel better about herself instead of using substances. Interventions: (1) 1: 1 with SA specialist (using MI) 2 x per week. Other team staff to use MI during other contacts to assist with identifying potential benefits. (2) attend “achieving my goals” group [persuasion] 2 x per week with SA specialist (3) 1: 1 social skills training with team staff to identify healthy activities and coping, as well as modeling and role playing how to use them.

Implementing the Treatment Plan Ø Schedule specific interventions to support the plan (Client weekly schedule) Ø Check daily that the plan is being implemented Ø Daily Report & Log Ø If the plan is not working, change it

Schedule Specific Interventions to Support the Plan Ø From treatment plan l l Ø Which staff person? What will he or she do? On what day? At what time? Record on Consumer Weekly Schedule Card

Check Daily that the Plan is Being Implemented Every consumer’s plan (via the weekly client schedule card) is checked each day in preparation or/during the daily team meeting. Each appointment from the weekly client schedule card is entered on the daily team schedule in the appropriate time slot, and a team member is assigned to each appointment.

Daily Report & Log Each consumer is reviewed daily during the daily team meeting Yes, you can get through 100 consumers in one hour l During the meeting, identify team members who had contact with the person during the past 24 hours or since the last meeting • “no contact” will be expected for many l Describe what happened in behavioral terms • brief, factual, focused on most imperative clinical symptoms or issues l The team leader or designee records a brief summary for each consumer (separate report “logs” for each consumer)

Daily Report & Log Ø continued…. If a problem needs to be addressed and it can be handled quickly, it is addressed during the meeting l some use last 15 mins for short 3 -5 min discussions for a few consumers Other team members might ask questions and/or offer suggestions Ø If the problem needs more extensive discussion, another meeting is scheduled for later that day with several team members Ø
 Process Ø Team Leader assigns members after assessment completed l")
Individual Treatment Team (ITT) Process Ø Team Leader assigns members after assessment completed l 3 -5 Staff Based on individual concerns, needs, & goals l Exs: l • • • Nurse for lots of physical health issues SA specialist for comorbid SUD ES for someone who wants to work Peer for someone receiving IMR from peer mix of team members for remaining positions to rotate responsibilities

Scheduling ITT’s Ø Meets minimum of 2 times per year during treatment planning meeting l l Recommend scheduling 6 -12 months in advance Team of 50: 2 hours per week Team of 100: 4 hours per week Staff meets 1: 1 with consumer to prep for ITT meeting

What happens at ITT Meeting? Ø From consumer’s perspective, review last six months history and treatment plan progress. l Ø Discussion and dialogue. Elicit from consumer new treatment goals. Take notes and quotes for tx plan. l Expect consumer to have difficulty when first starting the process

If a plan isn’t working, change it! Ø If the plan is not working, answer the following: l l Is the problem that the plan is addressing the team’s goal versus the consumer’s goal? Was the consumer’s goal misunderstood? Did the consumer’s goal change? Is the goal right and the plan wrong?

If a plan isn’t working, change it! Ø Are adjustments needed? l Because the consumer’s needs changed over time? l As a result of interventions provided? l As a result of changes in consumer’s environment or stressors (good or bad)? If so, schedule a treatment planning meeting with the ITT and the consumer

Ongoing Assessment & Treatment Planning GOALS ASSESSMENT DETAILED PLAN SCHEDULE OF INTERVENTIONS

Areas of Ethical Vulnerability for ACT Teams Ø Home visits Ø Controlling consumers’ money Ø Medication monitoring Ø Engagement process Ø Assertive outreach Ø Appropriate intensity of services

Consumer’s Right to Refuse Treatment Ø Involuntary Outpatient Commitment Ø Payee of Benefits Ø Consumer wishing to use services outside the ACT team

Possible Solutions to Ethical Dilemmas Ø Advance directives Ø Consumer involvement in treatment planning in a meaningful way Ø Direct more attention to what consumer values Ø Use involuntary commitment as last resort Ø Advisory board for ACT team Ø Consumer as provider on the ACT team Ø Regular review of team practices

Typical Skill Sets Common Across all ACT Team members Stagewise mindset Ø Motivational enhancement Ø Empathic reflection and listening Ø Clinical know-how to report critical symptom presentations back to team Ø More flexibility than rigidity Ø l l plans will change different consumer profiles may dictate different ratios Able to work on a team, trust the team Ø Healthy balance of hard work and self-care Ø

Skills Ø ACT as a platform for other EBP’s and other best practices • Cognitive Behavioral Techniques • IDDT interventions – substance abuse assessment and counseling • Supported employment interventions • Family Interventions • Illness Management & Recovery Interventions
 Ø Generalist vs specialist emphasis")
Rural ACT Ø Generally smaller teams (consumers and staff) Ø Generalist vs specialist emphasis Ø Intensive (ie, longer visits, multiple purposes) vs frequent, short visits l Not uncommon for short visits to be an issue in urban areas too (e. g. , parking in Chicago) Ø Community as part of the team (e. g. , extenders) Ø Routes take on even more importance

Rural ACT Ø Daily team meeting adaptations with technology Ø Nurse practitioner/Physician’s assistant vs MD l l Not many of ANY prescriber group in rural areas Telehealth may be a better option

Example: VA RANGE vs MHICM Ø VA Rural Access Networks for Growth Enhancement (RANGE rural ACT) vs. VA Mental health intensive CM (MHICM/ACT) l Similar patient profiles except: • less schizophrenia • more suicidality (VA)less long-term hospitalization, more comorbid SUD l l l Teams did not differ on intensity Slightly poorer QOL Better satisfaction with care

Acknowledgements These materials were adapted from presentations developed by: Gary Bond, Indiana University-Purdue University Indianapolis Barbara J. Burns, Duke University Medical Center Judy Cox, New York State Office of Mental Health Richard De. Liberty, IN Division of Mental Health and Addiction (formerly) Natalie De. Luca, ACT Center of Indiana Elizabeth Edgar, National Alliance for the Mentally Ill Lia Hicks, ACT Center of Indiana, Adult & Child Center Hea-Won Kim, Indiana University-Purdue University Indianapolis Mike Mc. Kasson, ACT Center of Indiana, Adult & Child Center New York ACT Institute National Implementing Evidence-Based Practices Project, Dartmouth
- Slides: 94