ASD Eligibility Outline n Review n ASD Rule

+ ASD Eligibility

+ Outline n. Review n. ASD Rule or CI/ ADHD/ EI n. Medical vs. Educational n. Coordinated n. Placement/ Evaluation Process Exit/ Transition
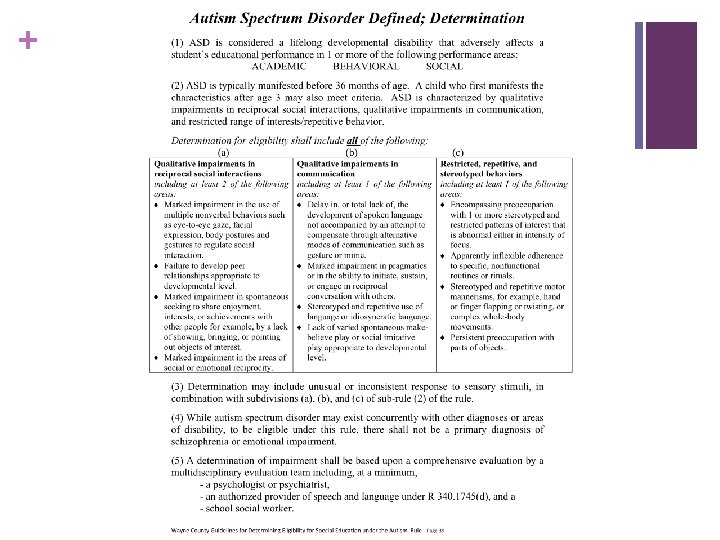

+ MI Rule 340. 1715 Section One Autism Spectrum Disorder is considered a lifelong developmental disability that adversely affects a student’s educational performance in 1 or more of the following performance areas: ACADEMIC BEHAVIORAL SOCIAL

+ Academic n Skill Development n n Academic n Work Output n Hand Writing n Reading n Literal>Inferential n Writing n Rote>Context n Math n Knowledge>Problem Solving n Word calling>Reading Comp. Learning Process n Attending n Transition

+ Behavior n External n n Acting Out n Internal n Avoidance n Aggression n Withdraw n Temper tantrum n Shut down n Noises n Hiding n Non-compliance Self-regulatory n Rocking n Self-talk n Break n Self-regulatory n Thoughts n Fantasy

+ Social n Information Sharing n Interest n Lack of give and take n Interacting at the appropriate time n Difficulty participating in groups n Inability to tolerate physical proximity. n Impaired social initiation

+ MI Rule 340. 1515 Section Two ASD is typically manifested before 36 months of age. A child who first manifests the characteristics after age 3 may also meet criteria. ASD is characterized by qualitative impairments in reciprocal social interactions, qualitative impairments in communication, and restricted range of interests/repetitive behavior.

+ ASD Rule Review Wayne County Guidelines for Educational Eligibility Attachment D & G

Determination for eligibility shall include All of the following Qualitative impairments in reciprocal social interactions including at least 2 of the following areas: Qualitative impairments in communication including at least 1 of the following areas: Restricted, repetitive, and stereotyped behaviors including at least 1 of the following areas: Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures and gestures to regulate social interaction. Failure to develop peer relationships appropriate to developmental level. Marked impairment in spontaneous seeking to share enjoyment, interests, or achievements with other people for example, by a lack of showing, bringing, or Delay in, or total lack of, the development of spoken language not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime. Marked impairment in pragmatics or in the ability to initiate, sustain, or engage in reciprocal conversation with others. Stereotyped and repetitive use of language or idiosyncratic language. Encompassing preoccupation with 1 or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus. Apparently inflexible adherence to specific, nonfunctional routines or rituals. Stereotyped and repetitive motor mannerisms, for example, hand or finger flapping or twisting, or complex whole-body movements. Persistent preoccupation

+ Attachment G

+ Qualitative impairments in reciprocal social interactions including at least 2 of the following areas: Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures and gestures to regulate social interaction. Failure to develop peer relationships appropriate to developmental level. Marked impairment in spontaneous seeking to share enjoyment, interests, or achievements with other people for example, by a lack of showing, bringing, or pointing out objects of interest. Marked impairment in the areas of social or emotional

Social Mild May avoid looking others in the eye, or become fussy if interaction is required. May be quite social or excessively shy. May not be as responsive to the adult as a typical peer. Moderate Shows aloofness (seems unaware of adult or peer) at times. Appears consistently aloof or unaware of what others are doing. Persistent or directed attempts are necessary to get the child’s attention at times. He or she almost never responds to or initiates contact with others. Minimal contact is initiated by the child. May cling to parents Cries or laughs somewhat more than most inappropriately. children of the same age. CARS May demonstrate a combination of high Severe Often the children will parallel play. Only the most persistent attempts to get the child’s attention have any effect.

+ Qualitative impairments in social interaction. n Qualitative impairments = Very Different n Much more than shyness or immaturity n Occurs across all settings n Occurs with all persons, not just strangers

+ Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures and gestures to regulate social interaction. n “Marked impairment” = “Gross and Sustained” when compared to age and developmentally appropriate peers. n n Eye gaze n is non-existent or happens only occasionally…May be Autism n Occasionally fails to make eye contact…Does not meet criteria. Facial expression n Facial expressions are inconsistent with peers in similar situation. n Oblivious to facial expression of others. n Study n Participants shown pictures of Mom, stranger, familiar toy, and unfamiliar toy. n Electrical brain activity is different when shown a familiar toy, but not Mom.

+ Failure to develop peer relationships appropriate to developmental level. n FAILURE n May play near others, but not with them. n May be interested in what others are doing, but choose not to join them. n n Watch the group play soccer, but does not try to join in. May be interested in having friends, but lack the skills and understanding necessary to make friends. n May attempt to engage peers in negative ways. n n Spits in peers face and laughs. May be drawn to negative relationships (bullies). n Negative relationships require fewer skills to maintain than positive ones.

+ Marked impairment in spontaneous seeking to share enjoyment, interests, or achievements with other people for example, by a lack of showing, bringing, or pointing out objects of interest. n Spontaneous n May fail to show pride in accomplishments. n n Does not share pride in school work, grades. May not call attention to objects of interest (joint attention). n Shared Gaze n n Does not point out animals. Emotional Reciprocity n Reading and understanding the emotion interaction between people. n If the student finds something funny, does he look to share it with others?

+ Marked impairment in the areas of social or emotional reciprocity. n May not become upset when other children cry. n May not understand that others have feelings. n May fail to understand that others have a perspective different from their own. n May lack “Theory of Mind” n ability to attribute beliefs, desires, emotions, perceptions, and intentions to self and others in order to understand predict behavior.

+ Qualitative impairments in communication including at least 1 of the following areas: Delay in, or total lack of, the development of spoken language not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime. Marked impairment in pragmatics or in the ability to initiate, sustain, or engage in reciprocal conversation with others. Stereotyped and repetitive use of language or idiosyncratic language. Lack of varied spontaneous make-believe play or social imitative play appropriate to developmental level.

+ Communication Mild Verbal Moderate Limited verbal Variety of intent present, but Limited intent for mostly awkward and odd or unusual in concrete, high interest presentation. items/activities. May have mild language delays to precocious language with unusually large vocabularies. Poor flexibility with language. Difficulty sustaining conversation. Echolalia, jargon and pronoun reversals often present. Unusual speech or voice patterns may be present. Severe Non-verbal Rare intent Vocalizing or noises made; may cry, scream or grab to meet need. Understanding and expression No meaningful gestures. limited in content, form and use.

+ Qualitative impairments in communication n Communication is very different n n Verbal and/or Non-verbal communication may be effected. Aspergers Syndrome n Verbal language appears typical or advanced n Social language (Pragmatics) is different.

+ Delay in, or total lack of, the development of spoken language not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime. n May lack communicative intent n The expectation that communication will result in a response n Receptive language may also be effected n “Overly Independent” n n Will go get an object rather than ask for it. Discrepancy between expressive and receptive language. n May use more language (scripting echolalia) than they understand

+ Marked impairment in pragmatics or in the ability to initiate, sustain, or engage in reciprocal conversation with others. n The student may have difficulty maintaining a turn taking conversation n Areas of interest dominate conversation regardless of the cues of others. n Unusual speech tone, rate, and/or pattern may be present.

+ Stereotyped and repetitive use of language or idiosyncratic language. n Echolalia n Immediate n n Delayed n n Repeat what was just said Movie’s and Commercials Echolalia may be functional

+ Lack of varied spontaneous make-believe play or social imitative play appropriate to developmental level. n May not imitate others (playing telephone, brushing hair with imaginary brush) n Very literal play n May not understand that the other individual is pretending…Not “in” on it. n May not understand humor or sarcasm

+ Restricted, repetitive, and stereotyped behaviors including at least 1 of the following areas: Encompassing preoccupation with 1 or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus. Apparently inflexible adherence to specific, nonfunctional routines or rituals. Stereotyped and repetitive motor mannerisms, for example, hand or finger flapping or twisting, or complex whole-body movements. Persistent preoccupation with parts of objects.
. Resistant to redirection from item")
Behavior Mild Moderate Limited or abnormal area of interest(s). Resistant to redirection from item or interest. Prefers specific routines. Prefers specific rituals throughout most activities. Reactions are sometimes unrelated to the objects or events surrounding them. Severe No interest in or inappropriate attachment to certain objects. Insistent on specific rituals/ any change from ritual becomes problematic. Reactions may be quite inhibited or excessive and May show widely different unrelated to the situation; reactions when nothing may grimace, laugh, or has changed. become rigid even though no apparent emotionproducing objects or events are present.

+ Restricted, repetitive, and stereotyped behaviors n Not just occasional n Take up significant time n Performed to the exclusion of more appropriate behaviors

+ Encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus. n This does not mean they like something…. they NEED it. n Talks about ______ all the time. n Has/seeks ______ all the time. n Gets upset when access to ____ is restricted. n Difficult to shift attention away.

+ Apparently inflexible adherence to specific, nonfunctional routines or rituals. n Rigidity in specific behavior patterns n Eat the same foods n Wear the same clothing n Line up toys n Becomes upset when these things are changed n Compulsive behaviors n He doesn’t want to touch door knobs…. . He NEEDS to.

+ Stereotyped and repetitive motor mannerisms, for example, hand or finger flapping or twisting, or complex whole-body movements. n Do not appear to have a function n Happens frequently and repeatedly n May or may not be redirectable n n n Usually temporary May look like n Unusual gait n Unusual body posture n Flapping n Rocking If present, they will be clearly present.

+ Persistent preoccupation with parts of objects. n n Intense focus on the parts of an object to the exclusion of the object. n Only interested in the wheels of cars n Constantly pulls string out of shirts n Spins everything Resistant to redirection

MI Rule 340. 1715 Section Three Determination may include unusual or inconsistent response to sensory stimuli, in combination with subdivisions (a), (b), and (c) of subrule 2 of the rule. Response to sensory stimuli may be considered but is not required.

+ Sensory Profile: Winnie Dunn n Sensory Profile Main Classroom Questionnaire n Sensory Profile Caregiver Questionnaire n Standardized tool to measure sensory processing abilities and their effect on functional performance n 2 tests together provide comprehensive view of performance in different contexts n Scores show patterns to indicate areas of strengths and concerns n Provides team discussion to ID link between sensory processing and performance difficulties

+ 3 Principles behind Model 1. Neuroscience: Neurological Threshold Continuum High Threshold: 7/11 Big Gulp Low Threshold: Dainty Tea Cup 2. Sensory Processing: Behavioral Response/Self Regulation Continuum 3. Sensory Processing Patterns: Degree to which a person misses, detects, obtains, is bothered by sensory input

+ Neurological Threshold n Vertical Axis of Model n Defined: The amount of stimuli required for a neuron or system to respond n Extreme Ends of the Neurological threshold continuum: n High: Habituation: NS recognizes something familiar happened, overtime no longer need to respond. n Low: Sensitization: NS mechanism that enhances reaction to what is perceived as important stimuli n Balance of habituation and sensitization needed for appropriate responses

+ Behavioral Response Continuum: n Horizontal Axis of Model: n Based on interests and tendencies to react to specific tasks n Behavior patterns at both extremes of continuum lead to unsuccessful performance. Acting In Accordance With Threshold: Passive: Disengaged from ongoing events experiences miss Acting to Counteract Threshold: routines Active: Driven to perform rituals, rituals interfere with daily

+ Test Yields 4 Quadrant Scores High Sensory Threshold: Verical Axis CNS response 1. Poor Registration: Lethargic, uninterested, dull Passive Self Regulation: Act in accordance with threshold 2. Sensation Seeking: Fidgety, Active, Excitable Active Self Regulation: Act to counteract threshold Low Sensory Threshold: Vertical Axis 1. Sensitivity to Stimuli: Distractible, Hyperactive Passive Self Regulation: Act in accordance with 1. threshold Sensation Avoiding: Resistant to change, rely on rituals Active Self Regulation: Act to counteract threshold

+ Section Scores n Taken from Questionnaire’s n Reflect sensory responses to sensory experiences n Environment important factor to create complete picture n Some cases structure of school makes it easier to manage than freedom at home n Builds understanding of parameters that make situations easier or more challenging n Dialog can create more affective learning environments: home, school and community

+Goals for Using Sensory Profile n Reliable tool to gather information on sensory processing patterns of student n See how patterns support/interfere with performance in class n Provide theory based team decision making n Appropriate to test anyone n Easy to administer n Provides complete picture across environments

+ Provides Foundation for Intervention Planning 1. Poor Registration: Enhance cues and task features: contrasts, decrease predictability 2. Sensory Seeker: Incorporate needed strategies into their day. They tell you what they need. Ex. , Errand runners, teacher’s helpers, leaders. 3. Sensitivity to Stimuli: Provide structured input vs random; Predictable patterns of visual & auditory input. Firm pressure, linear movement. 4. Sensory Avoider: Honor their need to reduce stimuli. Layer familiar with unfamiliar to habituate.

+ Dr. Dixon n What Quadrant does she fall into n She understands her issues and needs n She is functional (surgeon) n She relies on ritual, structure n She can ask for what she needs n She cannot change who she is, she has adapted to be a very important person who can share her talents with support from peers

MI Rule 340. 1715 Section Four While autism spectrum disorder may exist concurrently with other diagnoses or areas of disability, to be eligible under this rule, there shall not be a primary diagnosis of schizophrenia or emotional impairment.

MI Rule 340. 1715 Section Five A determination of impairment shall be based upon a comprehensive evaluation by a multidisciplinary evaluation team including, at a minimum, • a psychologist or psychiatrist • an authorized provider of speech and language under R 340. 1745(d) • school social worker.

+ Autism is Always. n Autism cannot be turned off. n If the student has Autism, they will have Autism all the time. n When determining eligibility, we must observe in multiple settings. n We should not have to look very hard to see Autism. n We should look very hard to verify that the characteristics that are consistent with an ASD eligibility are not attributable to another source.

+ Medical Diagnosis vs. Educational Eligibility

+ Medical vs. Educational n There IS a difference between a Medical DIAGNOSIS and an educational ELIGIBILITY. n We need to help parents understand the difference Diagnosis • DSM-IV criteria • 6 total • At least 2 social • At least 1 communication • At least 1 behavior Eligibility • DSM-IV criteria • 4 total • 2 social • 1 communication • 1 behavior • Must have an impact on educational performance in • Academic • Behavior • Social

+ Medical vs. Educational n an outside professional diagnosis of autism, aspergers, pdd-nos, or ASD by a psychiatrist or other medical doctor is not required by the state rules. BUT, n must be considered by the MET and the IEPT in determining a student’s eligibility for special education. HOWEVER, n the absence of a medical diagnosis does not mean an educational evaluation is not necessary.

+ Medical vs. Educational Diagnosis n Used for insurance billing Eligibility n Used for educational planning n Intervention n 13 planning (meds, behavioral) n Referral (clinical speech, OT) n 297 IV Disorders in DSM- Eligibility areas available to a MET team.

+ Medical vs. Educational n Asperger’s Disorder - Does not involve major deficits or delays in language or cognitive development. MI ASD rule includes this population n Schizophrenia - includes psychotic symptoms not seen in autistic disorder. It may (infrequently) be co-morbid with autism if there are prominent delusions and hallucinations. n Oppositional Defiant Disorder Unlike autism, this disorder involves deliberate hostile provocation of others and seeking of confrontations. The disorder centers on a disturbed interpretation of power and control in human relationships rather than a more generalized impairment of social under- standing.

+ Medical vs. Educational n When a MET team determines a student’s eligibility they are determining which of the 13 available categories of special education eligibility best describe the educational challenges that the student presents with. n If a MET team determines an eligibility that appears to conflict with a medical diagnosis, the team is not saying that the student is misdiagnosed. n It is possible for a student to have a medical diagnosis of Autism, but not qualify for special education services under the Autism eligibility rule.

+ Helping everyone understand n Start discussing the difference between eligibility and diagnosis when parents sign the REED. n Emphasize Process n REED n n Determine impact on educational performance IEP n Planning supports to help the student make progress. n ASD eligibility does not necessarily warrant a center program placement.

+ Assessment Process

+ School Psychologist
")
+ The Purpose Having team members from different disciplines involved in the evaluation procedure(s) promotes interdisciplinary collaboration, enhancing each MET member’s understanding of the student.

+ Important to Note An outside professional diagnosis of autism, including that from a psychiatrist, is not required by the state rules, but, if provided by the parent, must be considered by the MET and the IEPT in determining a student’s eligibility for special education. Must affect a student’s educational performance in one or more of the following performance areas: n Academic n Behavioral n Social

+ Evaluation Process n Information Gathering including Record Reviews n Interviews (e. g. , Parents, Teachers and Staff) n Interaction with Student within the environment n n Student response to Accommodations and Interventions n n n 12 to 16 weeks of data Observations n Settings n Activities Functional Assessment/Behavior Intervention Plan n n Multiple interactions with various MET members Supporting Data including interventions implemented Formal Assessment n Indirect measures (scales, interviews, standardized tests)
 Standardized tests 1. 3. Adaptive Behavior")
+ Multiple Evaluation Tools (one is not enough) Standardized tests 1. 3. Adaptive Behavior 1. Mullen 1. ABAS II 2. SB-V 2. BASC-2 3. WISC-IV 3. Vineland 4. UNIT 5. Leiter Autism checklists 2. 1. ADI-R 2. CARS 3. GARS-2 *See Attachment C

Special Considerations n Time/Location n Adaptations may be necessary n Observations n Reinforcements

+ Psychological Tools Purpose of Psychological Assessment n Supplement behavior scales/checklists n Strengths and weaknesses n Teaching strategies n Recommendations n Interpretation

Hypothesis Testing There are three keys to the hypothesis testing approach that will better ensure diagnostic integrity: 1. Become familiar with other disorders 2. Utilize expertise about alternatives 3. Design a broad evaluation approach

+ School Social Worker

+ School Social Worker Tools Purpose of Social Work Assessment n Comprehensive Social History n Provide a developmental framework for social relation skills n Observe social interactions across settings, across time, and in a variety of contexts n Address AI vs. EI

+ Social Work Assessment n Interviews with parents, staff, and other adults about the student’s: n n n Medical history, including current health issues, and medications Developmental history Educational progress, including adjustment to school, grades, attendance, peer relations, problems and concerns, and strengths and abilities Community involvement and related concerns and issues Family history for developmental disorders and psychopathology

+ Social Work Assessment n Developmental History n Developmental rates and sequences n Verbal and non-verbal communication n Student’s social interaction with peers and adults n Patterns of play n Areas of interest or expertise n Adaptive skills n Existence of established routines n Existence of repetitive moments or behaviors n Transitions n Idiosyncratic or unusual behavior n Sensory issues n Cognitive and learning style

+ Social Work Assessment n Observations: When we are observing students it is best to do so in a variety of social situations. Look for evidence of: n Attachment n Joint attention n Social awareness and orientation n Imitation n Social reciprocity/turn taking n Social rules n Social play/social skills n Social cognition

+ Social Work Assessment n n Evaluation Tools: In addition to interview and observation, choose tools that address presenting concerns. n Scales n Checklists n Behavior rating scales Consider if assistance is needed when staff and parents are completing these assessment tools.

+ ASD vs. EI n When the evaluating team is differentiating between ASD and EI they will be focused on sorting out these two criteria: n An inability to build or maintain satisfactory interpersonal relationships with peers and teachers. n Inappropriate types of behavior or feelings under normal circumstances.

+ ASD vs. EI n An inability to build or maintain satisfactory interpersonal relationships with peers and teachers. n n Is it more about relationships or about social and communication deficits? Is there a sense that there’s the capacity for truly joining others beyond one’s self interest? A sense that significant change might be possible if external factors could be controlled? Nonverbals, joint attention, seeking shared enjoyment? (Pamela Lemerand, Ph. D. Psychologist)

+ ASD vs. EI n Inappropriate types of behavior or feelings under normal circumstances. n Are the behaviors and feelings secondary to communication deficits and social deficits? n Are they the result of interference in preoccupations or restricted interests? n Are they driven by disruptions to routines, rituals, or rules? n Inflexibility or anxiety vs. fear based behavior? (Pamela Lemerand, Ph. D. Psychologist)

+ Experienced teachers say: EI AI Can small talk or chat in depth; reciprocal Limited or scripted; not very reciprocal; poor initiation School is a source of angst; problems everywhere School can be a safe haven with structure and supports May have cultural subgroup A loner When angry-language ability is often heightened When angry, language is the first to go Immature/Regressive Can be “little professor” On good days, can have significant insight into emotions of self/others Very little insight into emotions of self/others; repeats what he has been told (Pamela Lemerand, Ph. D. Psychologist)
")
+ Speech - Language Pathologist (TSLI / CCC)

+ Speech and Language Evaluation Procedures: n Review School Records n Review Medical History n Developmental history n Parent Interview n Observation n Formal Testing

+ Records Review n Classroom performance n Behavioral issues n Speech and Language Records

+ Medical History Review n Special Attention to Hearing and Speech Issues n Chronic Ear Infections n Neurologically based speech disorder n Motor based speech disorder n Rett’s Syndrome- overwhelmingly in females, regression in social, cognitive, and psychomotor development after an early period of development. The social regression along with the appearance of repetitive behaviors increases the change of misdiagnosis. (Genetic testing for mutated gene)

+ Developmental History n Emphasis on Speech and Language Development n Family history for developmental disorder, psychopathology, speech, and language disorders n Regression of Skills n *Special Note* - Comparent developmental history with normal development. n Parents are aware of ASD characteristics – information is not always accurate n Psychological Testing Results – where is the student functionally?

+ Parent Interview n Follow-up on questions asked in developmental history n Eating, sleeping, use of toys, peer interaction, sibling interaction n Cultural norms – eye contact, getting attention, answering questions n What do the parents do to re-direct or change behavior

+ Observation!!! n Classroom Behavior n Small Group Behavior n Interaction with Peers n Interaction with Staff/Adults n One-on-One Interaction

+ Formal Testing n Expressive One Word Picture Vocabulary Test n Receptive One Word Picture Vocabulary Test n Peabody Picture Vocabulary Test n Preschool Language Scale n The Nonspeech Test for Receptive/Expressive Language n Autism Spectrum Disorder (ASD) Communication Profile (Attachment H) n ADOS n Clinical Evaluation of Language Fundamentals n Pragmatic Profile

+ * It is important to note that a child can have a severe deficit in the areas of expressive, receptive, and/or pragmatic language and still not have Autism Spectrum Disorder*

+ It is necessary to evaluate each of the areas listed in the Social Interaction and Communication sections. Communication impairment alone does not differentiate between ASD and CI versus CI alone. Pamela Lemerand Ph. D
 n Marked impairment in the use")
+ Social Interaction: (Two of the following areas) n Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures and gestures to regulate social interaction n Failure to develop peer relationships appropriate to developmental level n Marked impairment in spontaneous seeking to share enjoyment, interests, or achievements with other people for example, by lack of showing, bringing, or pointing out objects of interest * Children with autism may see adults, not as partners for social interaction, but rather as tools to help them get what they want.
 n Delay in, or total lack of,")
+ Communication: (One of the following areas) n Delay in, or total lack of, the development of spoken language not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime n Marked impairment in pragmatics or in the ability to initiate, sustain, or engage in reciprocal conversation with others n Stereotyped and repetitive use of language or idiosyncratic language n Lack of varied spontaneous make-believe play or social imitative play appropriate to developmental level

+ It is important to meet as a team to discuss the evaluation results. n There is a lot of overlap between the disciplines n It is a team decision n Each member of the team is responsible for checking the appropriate boxes on the MET n Not every box has to be checked n Differential diagnosis n Discussion

+ Interpretation 1. Guiding principle: consider ASD diagnosis in addition to alternative diagnoses (differential diagnosis). 2. Determine how diagnosis impacts educational performance. 3. Determine how diagnosis impacts educational programming (accommodations→placement)

+ Least Restrictive Environment Considerations

Special Education is not a Place + n Special Education is a support n Special Education is a service

+ LRE Factors The setting in which the student…. . n can make progress on educational goals with appropriate supports and services. n is as close as possible in setting and geography to the classroom the student would attend if they did not have a disability. n has access to general education curriculum, extra curricular activities, and any other program that non-disabled peers have access to. LRE is a continuum of services and should not be effected by the “availability” of programs.

LRE FLOWCHART Center-Based ASD program separate facility Center-Based ASD program general education building Placement/services in local special education programs (resource room, categorical classroom, etc…) 1 -3 hrs. of services is the first step for all special education services beyond the level of speech and language services (Services may be provided directly, indirectly, or consultatively) Ex. Push in or pull out for tests etc…, check in/checkout systems, planners and other services that support students in the general education environment Support in general education environment Consider in district / out of district ASD consultant services with special education supervisor/director approval

+ Remember: n Additional services may mean a more restrictive environment n Prior to adding services to a student’s IEP there MUST be collaboration among the team members Team Members: n Parent n School Psychologist n School Social Worker n Speech Pathologist n General/ Special Education Teachers

+ Center Program Referral Process

+ Center Program Referral Process 1. The Director of Special Education or designee must be notified to initiate the placement process for a referral to all Center Based Programs. 2. Team members will gather data into a referral packet a. Current Teacher Report identifying rationale for considering a change in program/placement b. Current REED, IEP, Progress Report, MET Summary Report and supporting evaluation documents, and report cards c. PLUS………

+…. Referral to Center-Based Program = proposed change in LRE … so n A minimum of 12 – 16 weeks of data in the current setting on behavior, academics, IEP goals and all research based interventions implemented. n A written description of how instruction was differentiated (in both GE and SE) with samples provided for progress portfolio. n FBA, BIP, and supporting data including a written description of all research based interventions used. n n Consider ASD consultant service with special education director/supervisor approval A written description of what academic/social research based interventions were used and a summary of individual progress. n Completion of the “Student Profile” Consider age of student and other environmental influences

+ Center Program Referral Process cont. . 3. LEA Special Education Administrator/Center Program Administrator contacts parent to inform of need for consultation and planning from outreach ASD Teacher Consultant (if not already involved). 4. LEA Special Education Administrator/Center Program Administrator contacts parent to inform of the need for change in placement and to schedule a meeting to discuss information. 5. LEA/Center Program Administrator will submit referral packet to appropriate Center Program/LEA.

+ Center Program Referral Process cont. . 6. Observation of student by LEA /other recommended program staff 7. Team meeting with LEA and current program staff 8. Visitation to recommended program by parents, resident district, student if appropriate. 9. Convene IEP Team Meeting if change in placement is determined (including severity of behavior and disruption of learning environment if applicable).

+ Exit & Transition Process

+ Exit Criteria Prior to convening an IEPT to move a student from a center program to the resident district, the team must meet to discuss the data and possible placements. Team members may include: student parent(s) of student sending classroom teacher(s) sending support staff LEA director/supervisor receiving school students receiving building staff receiving classroom teacher(s) receiving support staff receiving principal

+. . . Exiting a Center-based program = a proposed change in LRE … so n A minimum of 12 – 16 weeks of data in the current setting on behavior, academics, IEP goals and all research based interventions implemented. n A written description of how instruction was differentiated (in both GE and SE) with samples provided for progress portfolio. n FBA, BIP, and supporting data including a written description of all research based interventions used. n n Consider ASD consultant service with special education director/supervisor approval A written description of what academic/social research based interventions were used and a summary of individual progress. n Completion of the “Student Profile” Consider age of student and other environmental influences

+ Transition Process The intention of an ASD center-based programs is to prepare the student to transition to a less restrictive environment. This process requires: 1. A written transition plan (outlining strengths and challenges) 2. 6 -8 week’s worth of data (including what interventions were used, for how long, and data showing the progress) 3. Placement is an IEP Team decision. n Students do not automatically transition from an ASD center-based program into their resident district’s categorical programs. n Placement decisions are based on the student’s present level of functioning not their eligibility. 4. Placement that includes an individual paraprofessional is not considered best practice and preference will be given to a general education placement with special education supports.

+ Questions/ Concerns Thank You!
 - mellasg@wy. k 12. mi. us")
+ ASD Guidelines Training Committee Gail Mellas (Chair) - mellasg@wy. k 12. mi. us Darnella Delfine –darnella. delfine@lpps. info Lauren Feigel – feigell@wy. k 12. mi. us Patricia Gallagher –gallagp@taylor. k 12. mi. us Rachel Johnson – johnsora@wy. k 12. mi. us
- Slides: 101