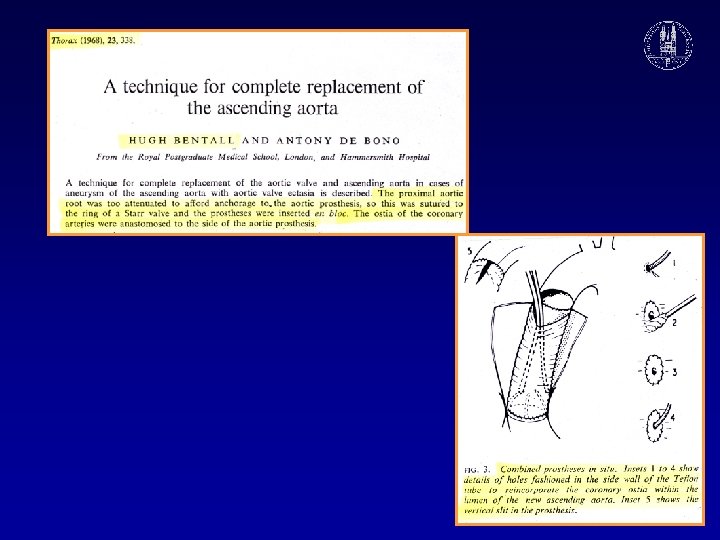
ASCENDING AORTIC ANEURYSM TECHNIQUE MARKO TURINA University Hospital












 and biologic (n = 80")













")
- Slides: 35
ASCENDING AORTIC ANEURYSM: TECHNIQUE MARKO TURINA University Hospital Zurich, Switzerland
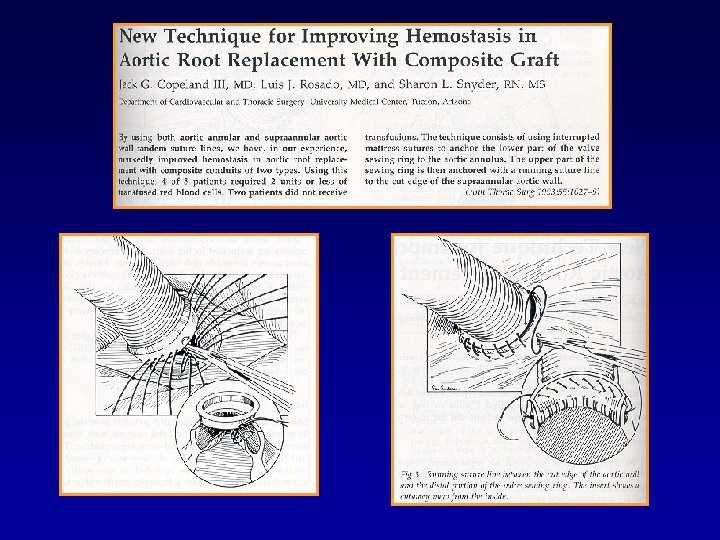
Tension at Coronary Ostia with Graft Inclusion Technique From Crawford: Diseases of the Aorta
GRAFT INCLUSION TECHNIQUE: SUBSTANTIAL SOURCE OF COMPLICATIONS From Crawford: Diseases of the Aorta
Perigraft hematoma after wrap technique
Spurious Aneurysm at the Origin of RCA After Graft Inclusion Technique in Composite Graft
Spurious Aneurysm of the Aortic Root After Composite Graft: Detachment of the Coronary Orifice
COMPOSITE GRAFT IN MARFAN’S DISEASE: False aneurysm at the origin of LMCA BS 25 LA False aneurysm True lumen Aortic valve BS 25 RVOT Composite graft (compressed) Courtesy Prof. Jenni, Echocardiography USZ 35 year old male with Marfan, 9 y. after composite graft repair for acute Type A dissection
FALSE ANEURYSM AT THE ORIGIN OF LMCA AFTER COMPOSITE GRAFT LA BS 25 Aortic valve RVOT True lumen Leakage into the false aneurysm Composite graft
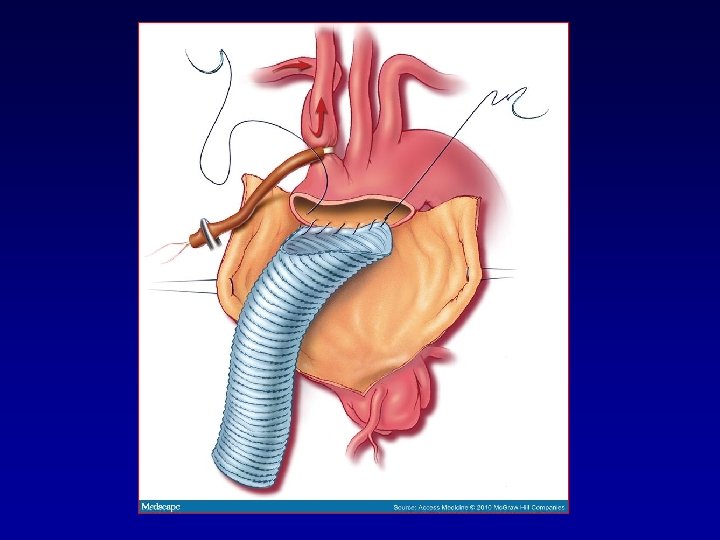
Composite Graft with Open Technique
Composite Graft with Open Technique
Myocardial Protection in Ascending Aortic Surgery Zurich 2003 • Systemic hypothermia 280 C • Begin with retrograde cardioplegia, cross -clamp and arrest with antegrade perfusion directly into coronaries (except in acute Type A). • Continuos retrograde cold oxygenated blood @ 160 C throughout procedure. • Warm reperfusion (“hot shot”)
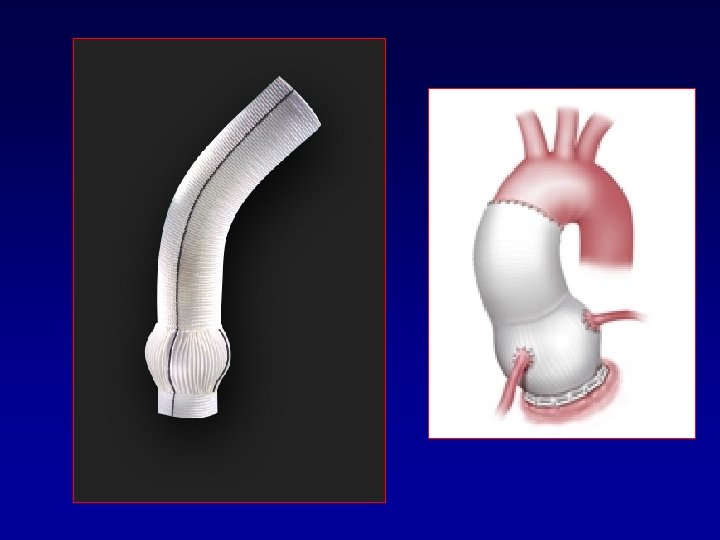
Schematic drawing of mechanical (n = 126 patients; 61%) and biologic (n = 80 patients; 39%) valved composite grafts used for aortic root replacement using a modified Bentall technique Etz C. D. et al. ; Ann Thorac Surg 2007; 84: 1186 -1194 Copyright © 2007 The Society of Thoracic Surgeons
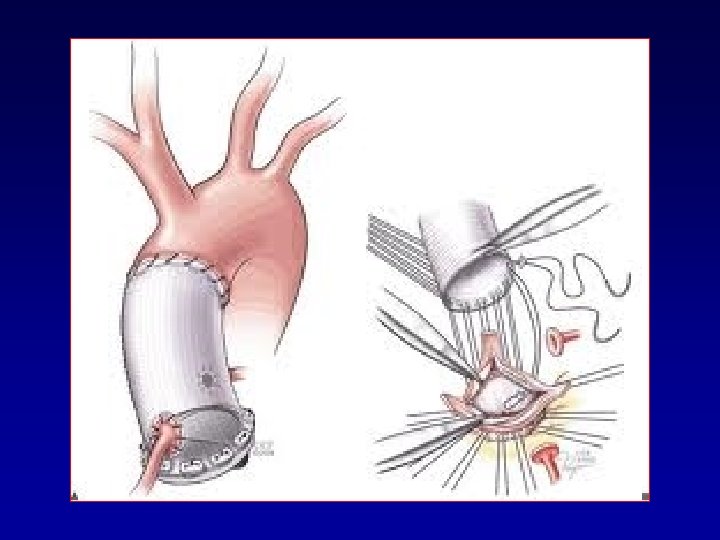
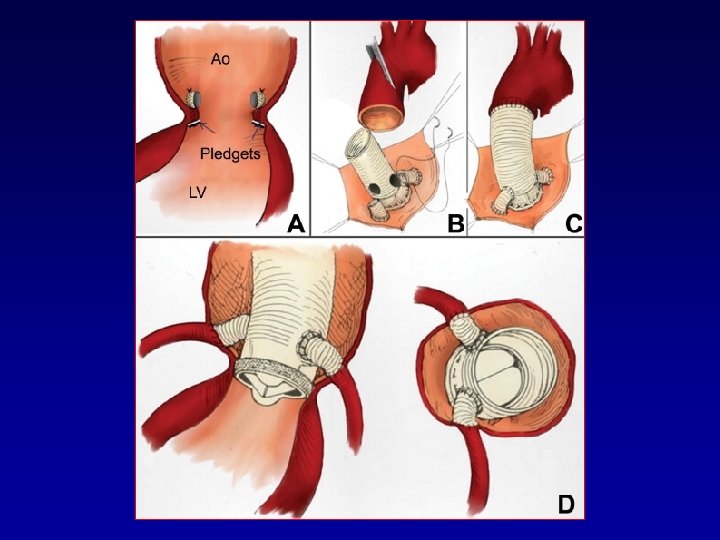
BUTTON TECHNIQUE FOR COMPOSITE GRAFT REPAIR
From Barbeau et al, Ann Thor Surg 1999
Axillary Artery Cannulation: Essential in Arch Procedures and Acute Type A
http: //www. mpoullis. net/bscpb/blank. htm
Bavaria et al. , Ann Thor Surg 2003
Hemiarch Bentall Procedure Subclavian/Innominate Artery Perfusion Technique • • Monitor left and right radial, and femoral artery pressure. Cannulation of subclavian/innominate artery. Cool patient to 280 C. Cross clamp innominate and left carotid, block left subclavian artery with balloon, perfuse upper body with 10 ml/kg, and administer antegrade and retrograde CPL. • Perform distal anastomosis first, clamp the graft and resume body perfusion. • Perfrom proximal part of the operation (valve and coronaries). • Re-anastomose proximal and distal graft segment.
CABROL’S TECHNIQUE FOR DECOMPRESSION OF PERIGRAFT SPACE J Thorac Cardiovasc Surg 81: 309 -315, 1981
CABROL’S ORIGINAL DESCRIPTION OF CORONARY ANASTOMOSIS J Thorac Cardiovasc Surg 81: 309 -315, 1981
Modifications of Button Technique Hilgenberg et al, Ann Thor Surg 1996 Pratali et al, Tex Heart Inst J 2000
Completion Bentall procedure Malekan R. et al. ; Ann Thorac Surg 2011; 92: 362 -363
Two common errors in ascending aortic surgery: • Timid resection of aneurysm (instead of going into arch) • Use too long graft (they all lengthen and distend with time, some up to 20 – 30 % of diameter)
Keep you graft short, it expands and lengthens with time! Ha H I et al. Radiographics 2007; 27: 989 -1004 © 2007 by Radiological Society of North America
Potential Source of Recurrencies: Distal Anastomosis in Ascending Aorta (Instead in Arch)