ARTRITIS Hospital Ramn y Cajal Cristina Abad Nacho

ARTRITIS Hospital Ramón y Cajal Cristina Abad Nacho Gallego José Acosta Isabel García

CONTEXTO CLINICO • ♂ 64 años • Artritis larga evolución. • Ciatalgia + RM lumbar sin causa del dolor • AHORA: ↑ dolor + paralisis sensitivo-motora. • EMG: neuropatía nervio tibial posterior

¿De qué tipo de artritis se trata? 1. Artritis reumatoide 2. Artritis infecciosa 3. Artritis gotosa 4. Artritis por PFC
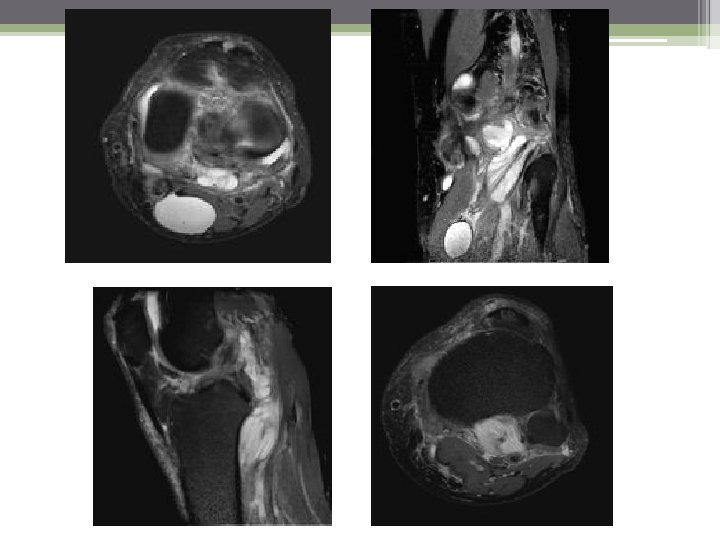

¿PODEMOS DETERMINAR LA CAUSA DE LA CLINICA DEL PACIENTE? 1. Si, se debe a compresión nerviosa por el quiste de Baker 2. Si, se debe a compresión nerviosa por ocupación del arco soleo. 3. Si, se debe a una lesión traumática por los tofos. 4. No, debemos extender el estudio al resto del MI.

CONCLUSIÓN 1. Artritis gotosa: � Espacio articular normal � Cartílago conservado � Tofos y erosiones óseas 2. Formación de quistes articulares 3. Rotura de ganglión y miositis del m. poplíteo 4. Compresión de terbio tibial por aumento de tamaño del m. poplíteo. ARTRITIS GOTOSA QUISTE DE BAKER Y GANGLIONES ROTURA GANGLION MIOSITIS MUSCULO POPLITEO NEURITIS COMPRESIVA NERVIO TIBIAL

BIBLIOGRAFIA • Girish G, Glazebrook KN, Jacobson JA. Advanced imaging in gout. AJR Am J Roentgenol. 2013 Sep; 201(3): 515 -25. • Su H, Li X, Zhao N, Zou H, Jiang L, Zhou Y. Comparing the usefulness of four imaging techniques in the same gouty arthritis patient. Int J Rheum Dis. 2012 Oct; 15(5): e 128 -30. • Dalbeth N, Doyle AJ. Imaging of gout: an overview. Best Pract Res Clin Rheumatol. 2012 Dec; 26(6): 823 -38.
- Slides: 7