Articular fractures upper extremity moderated interactive session AOTrauma


























 3. Immediate")






- Slides: 35
Articular fractures upper extremity moderated interactive session AOTrauma Advances Course
Learning outcomes • Manage complex elbow dislocations • Evaluate evidence for fixation vs replacement in proximal humeral fractures • List the indications and surgical techniques for distal humeral fractures • Discuss an algorithm for the use of ORIF vs external fixation vs pins in the treatment of distal radial fractures
Is fixation with locked plating the treatment of choice for distal radial fractures in your practice? 1. Never 2. Rarely 3. Occasionally 4. Commonly
Key points from lectures Proximal humerus • ORIF as a first treatment option in all reducible fractures • New MIPO approaches • Hemiarthroplasty for old patients/irreducible fractures/painful avascular necrosis Distal humerus • Requires ORIF using both column fixation? • Posterior approach utilizing an olecranon osteotomy is still recommended. • Predictable outcomes
Key points from lectures Elbow fracture dislocation • Injury pattern tells you what structures are likely to be injured and how • The LCL is more important than the MCL • Keep elbow concentric • Coronoid fractures can be a problem Distal radius fractures, C 3 types • Stable fixation is the key to good outcomes • Patient function improves up to 1 year postoperatively • DASH scores improve over 2 years, but uncommonly returned to baseline
58 -year-old man, motorcycle collision • Isolated injury to right upper extremity • Grade 1 open injury • NV status good
What is the treatment after debridement? 1. Fixation with locking plate 2. Tension band construct 3. Intramedullary nailing 4. Hemiarthroplasty 5. Nonoperative care
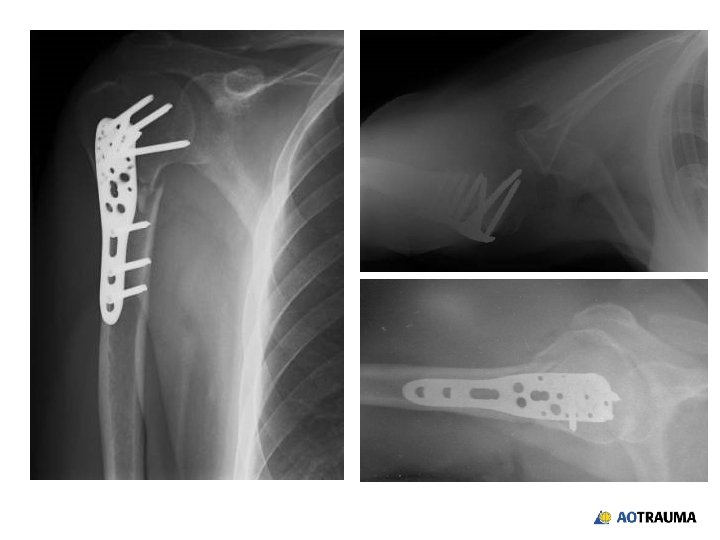
58 -year-old female, pedestrian hit by car • Housewife • Nondominant extremity • Closed isolated injury • Neurovascular status ok
What would your initial step be? 1. X-ray of axial view 2. CT 3. Reduction in ER 4. Reduction in OR
After closed reduction in ER
What treatment options would you offer? 1. ORIF with standard plates 2. ORIF with locked plates 3. Screw fixation 4. Hemiarthroplasty 5. Other
postoperative x-rays
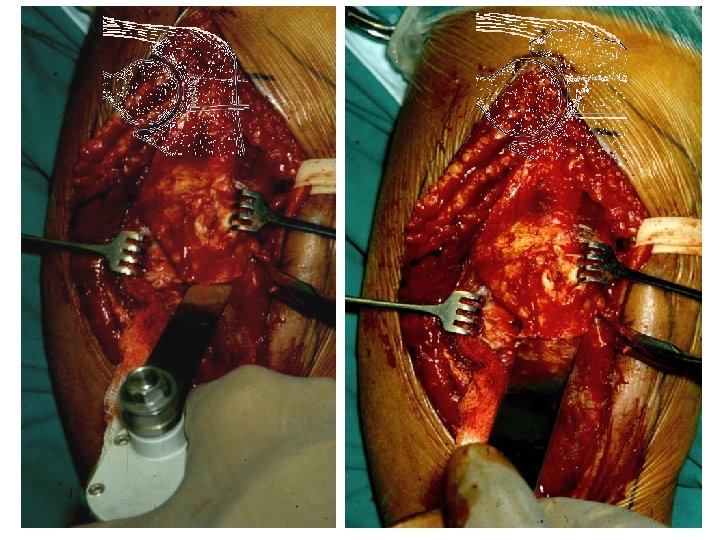
25 -year-old female, fall on the street • Dominant extremity • Closed isolated injury • Neurovascular status ok
What would your surgical approach be? 1. Posterior with olecranon osteotomy 2. Posterior—triceps reflection 3. 2 incisions—medial/lateral 4. Other
What would your choice of implant be? 1. Two conventional plates—parallel 2. One conventional plate—specialty type 3. Two conventional plates—orthogonal 4. Two locking plates—precontoured
Do you prescribe prophylaxis treatment to prevent heterotopic ossification? 1. Always 2. Sometimes or depends 3. Never
Do you transpose the ulnar nerve? 1. Always 2. Sometimes or depends 3. Never
49 -year-old male banker, falls off bike • Fracture dislocation of elbow • Wrist is normal and NV status is ok • Reduction of dislocation reveals elbow pathology
How would you proceed with treatment? 1. Radial head replacement 2. Radial head ORIF 3. Radial head ORIF with coronoid ORIF 4. Radial head ORIF with coronoid ORIF and medial ligament reconstruction 5. Cannot tell and need a CT
Which coronoid fractures should be managed with ORIF? 1. All 2. Large displaced coronoid fractures only 3. Fractures that present with a dislocation 4. Most fractures should be treated if the other stabilizers of the elbow are injured as well
43 -year-old female, fell on the street • Bilateral distal radial fracture • Closed injuries • Neurovascular status ok
left right
Reduction and plaster cast left right
What now? 1. Continuation of conservative treatment 2. Further diagnostic procedures (CT) 3. Immediate surgical treatment 4. Spanning external fixator
Left
Right
What treatment would you offer now? 1. Percutaneous K-wire fixation 2. External fixator for right side and conservative treatment of left side 3. Conventional plates dorsal for left side and palmar for right side 4. Locking dorsal plate for right side and double locking plate for left side 5. Other
6 weeks postoperatively left right
3 months postoperatively
Summary • Anatomical reduction and early ROM is vital for restoration of function • New locking plates can be useful • Attempt ORIF for most displaced fractures of the proximal humerus in healthy patients • Distal humeral fractures require ORIF with both column fixation • Stability is the key to success in managing complex injuries around the elbow—bone and soft tissues • Stable fixation for all of the radial columns injuries will lead to good outcomes