ARTERIAL ULCERS INTRODUCTION Arterial ulcers also referred to









")




 oral intake of 6. 6 g/day for 2 weeks")


- Slides: 33
ARTERIAL ULCERS
INTRODUCTION Arterial ulcers, also referred to as ischemic ulcers, are caused by poor perfusion(delivery of nutrient-rich blood) to the lower extremities. The overlying skin and tissues are then deprived of oxygen, killing these tissues and causing the area to form an open wound.
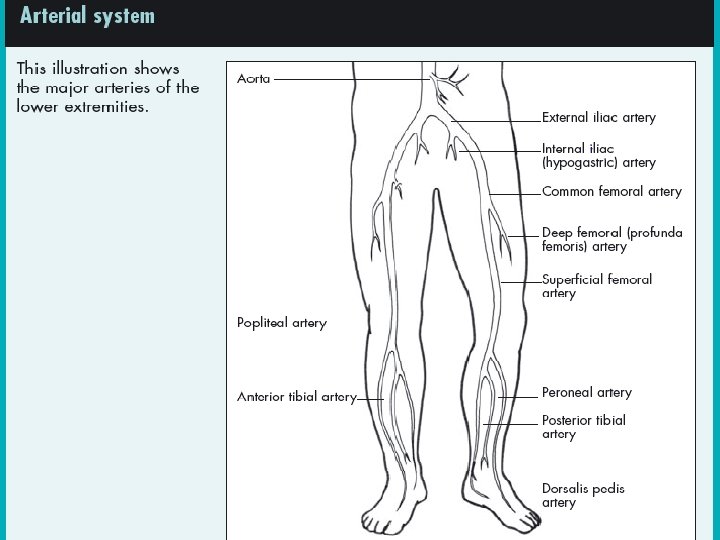
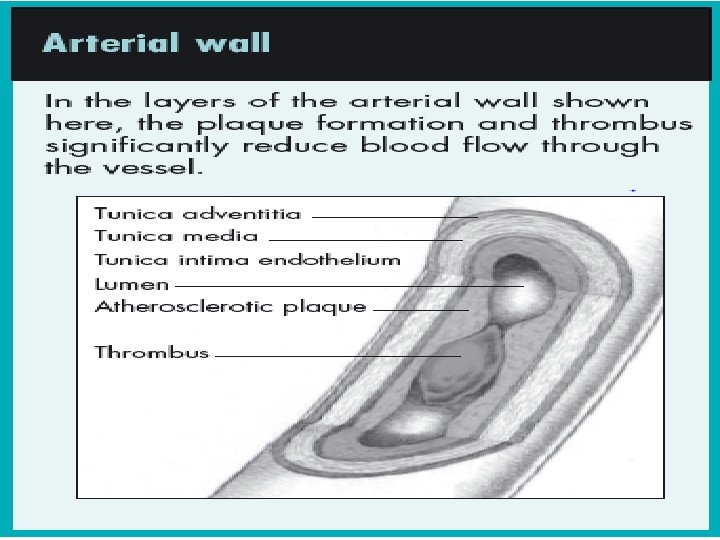
ARTERIAL ULCER PATHOPHYSIOLOGY • Arteries are responsible for carrying nutrient- and oxygen-rich blood to the various tissues in the body. • Ischemia, which refers generally to a restriction in the blood supply, can lead to arterial ulcers when it stems from a narrowing of the artery or damage to the small blood vessels in the extremities. • The reduced blood flow then in turn leads to tissue necrosis and/or ulceration.
RISK FACTORS – Atherosclerosis is the most common cause of lower extremity arterial disease – Diabetes – Tobacco Products – Hyperlipidemia – Advanced Age – Obesity – A Family History of Cardiovascular Disease – Anemia – Arthritis – CVA – Intermittent Claudication – Traumatic Injury to Extremity – Vascular Procedures/Surgeries – Hypertension – Arterial Disease
LOCATION & CAUSE –The location of traumatic ulcers varies depending on the cause, but these wounds are commonly found on the foot or on the anterior tibial area of the lower leg. • Traumatic ulcers may be caused by an acute physical injury, such as blunt trauma (for example, bumping into a piece of furniture or dropping a heavy object on the foot), or by acute or chronic pressure (such as the continual pressure from ill-fitting footwear). • Several other conditions may be responsible for tissue breakdown, including thermal extremes, chemicals, or a localized clot or embolus, which can also lead to decreased cellular nutrition from impaired arterial flow. Regardless of the cause, when ischemia is present, wound healing is inhibited.
DIAGNOSING VASCULAR ULCERS • Vascular disease and ulcer etiology can be determined by: • Medical History • History of allergies • physical examination • Pain • Tissue loss • Change in appearance • Sensation
• Patient’s medications • His or her occupation • ABCDE’S Ø A 1 C: Hemoglobin A 1 C Ø B: Blood pressure Ø C: Cholesterol Ø D: Diet and obesity (body mass index above 25) Ø E: Exercise Ø S: Smoking (One cigarette decreases circulation
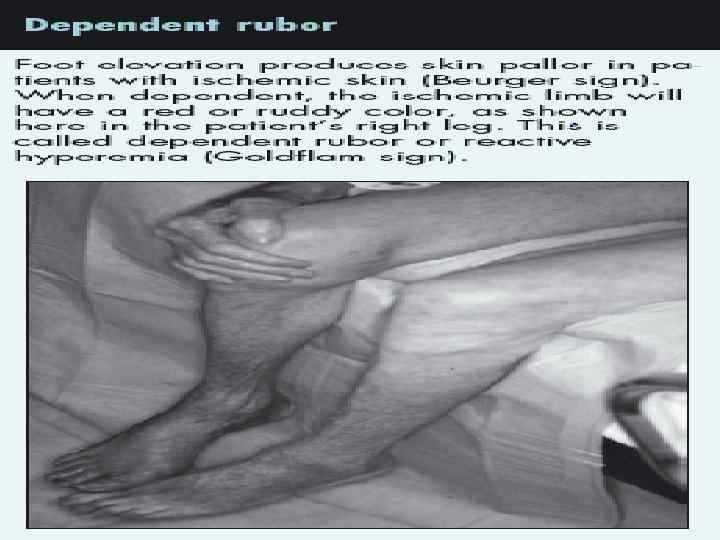
PHYSICAL EXAMINATION • Skin assessment Examining the distal extremities for • taut or shiny • atrophic skin • skin color • comparison with the other foot and toes • pale, progressing to a mottled netlike appearance (livedo reticularis) and subsequently to a dark purple hue, and finally black • Elevating the foot at a 45 -degree angle causes the ischemic limb to become pale
• In dependent position color turns to dark redreactive hyperemia • Loss of hair distally • Nails may lose their luster and become thickened. • Temperature changes • Capillary refill time is determined by compressing the skin-Normal capillary refill time is less than 3 seconds from pallor to normal skin color • The presence or absence of dorsalis pedis or posterior tibial pulses • These arteries can be absent congenitally
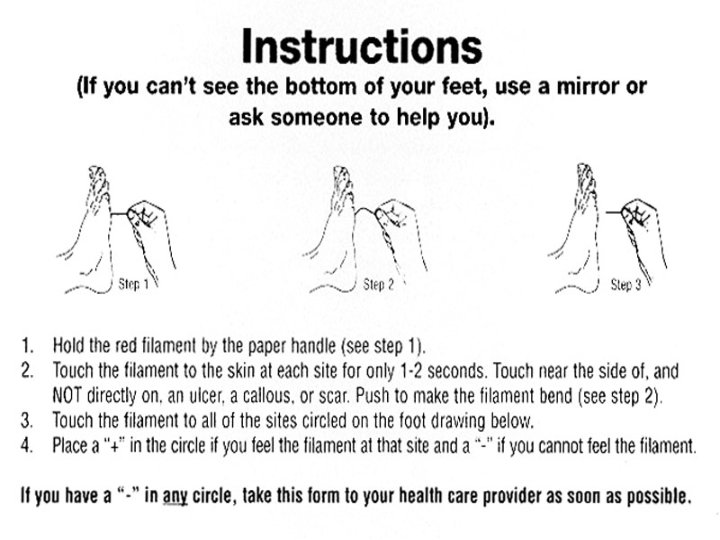
• Increased pain with activity and/or elevation (intermittent claudication, resting, nocturnal and positional) • Test patients with foot or leg ulcers for neuropathy • Lack of sensation • SAM • Semmes-Weinstein monofilament
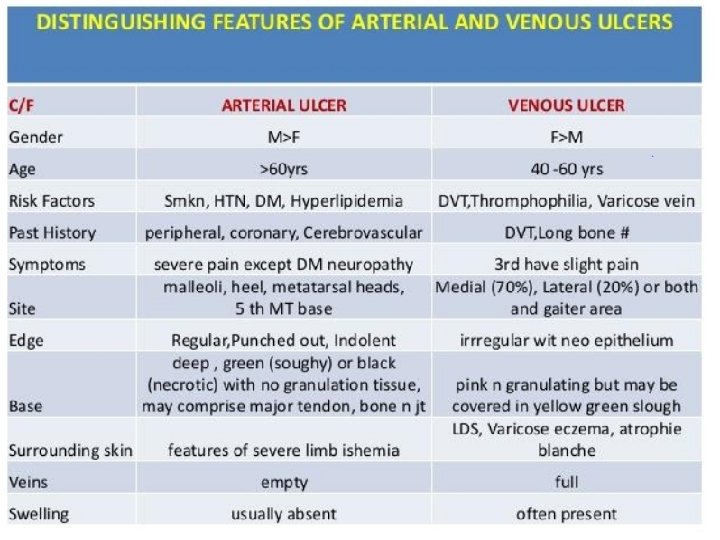
ARTERIAL SIGNS AND SYMPTOMS • • • Pain Rest pain Claudication pain(calf, buttocks, thigh or feet) Initial claudication distance (progressive atherosclerosis disase) Waking at night With neuropathy: May not experience pain Hyperesthesia can not bear light touch of stockings Sensations of burning, stinging, shooting, and stabbing pain (neuropathic pain)
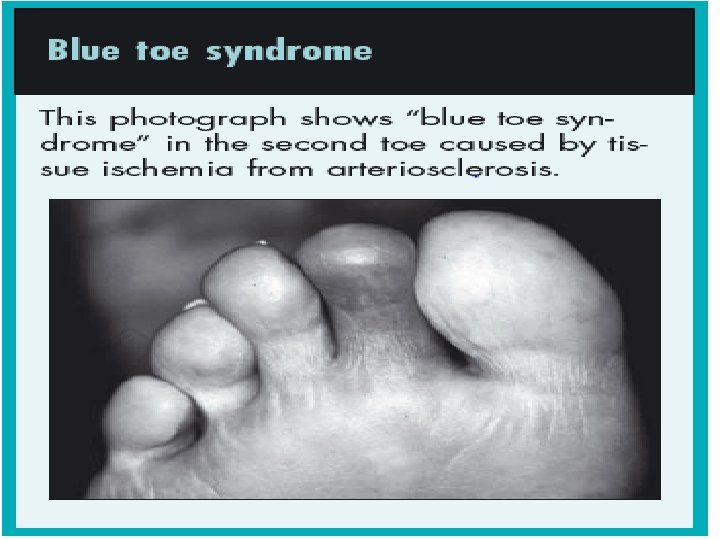
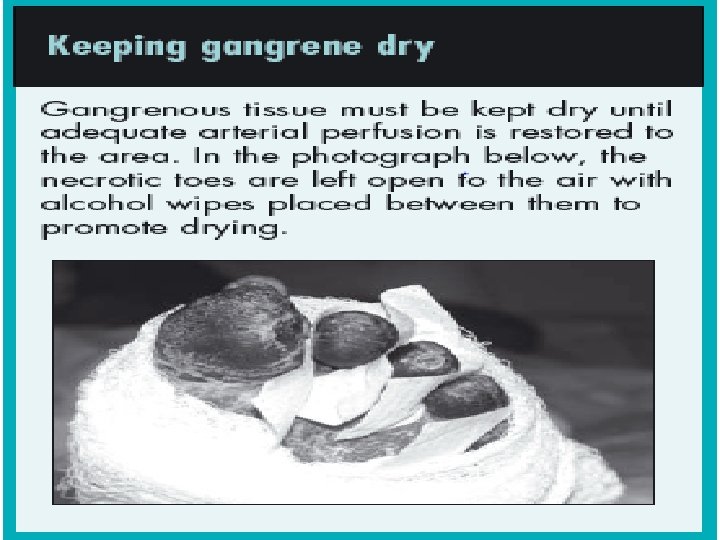
• Ischemic symptoms are exacerbated by nicotine • Gangrenous tissue eventually becomes black, hard, and mummified • “Blue Toe Syndrome” in the second toe caused by tissue ischemia from arteriosclerosis • Arterial ulcers may also be found between the toes, starting as a small, moist, macerated spot on the skin surface extending deep into the bony structure of the foot.
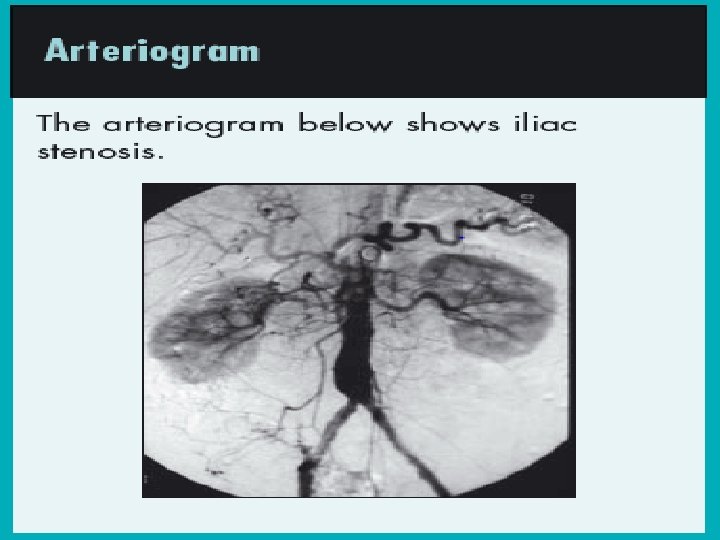
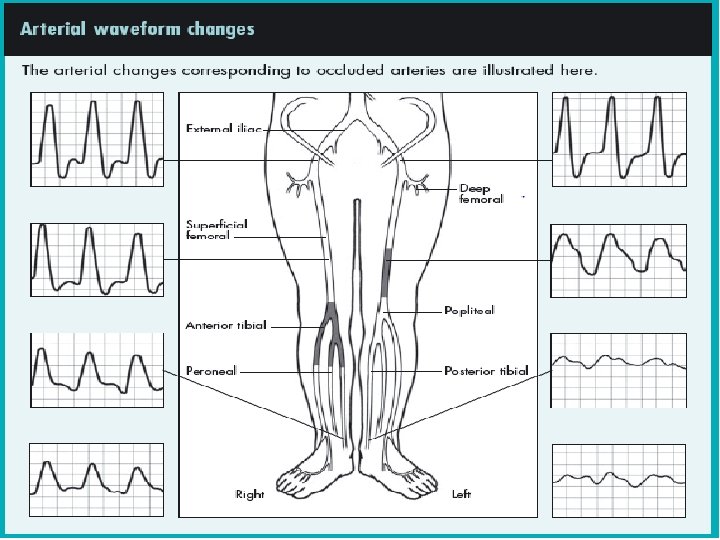
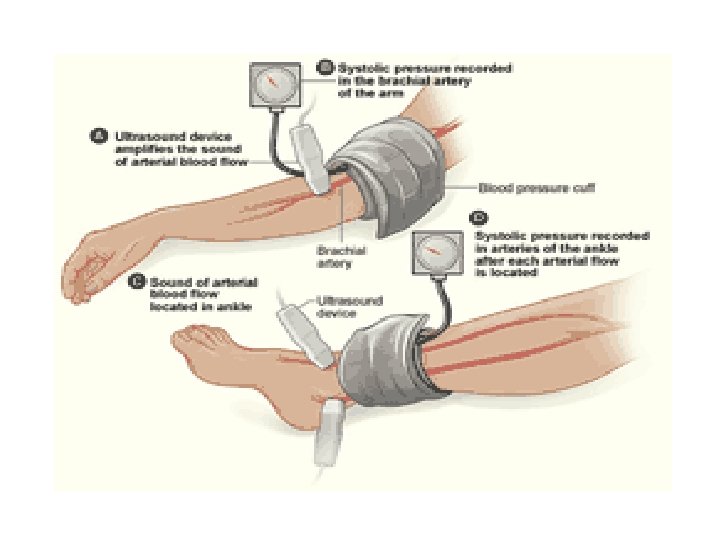
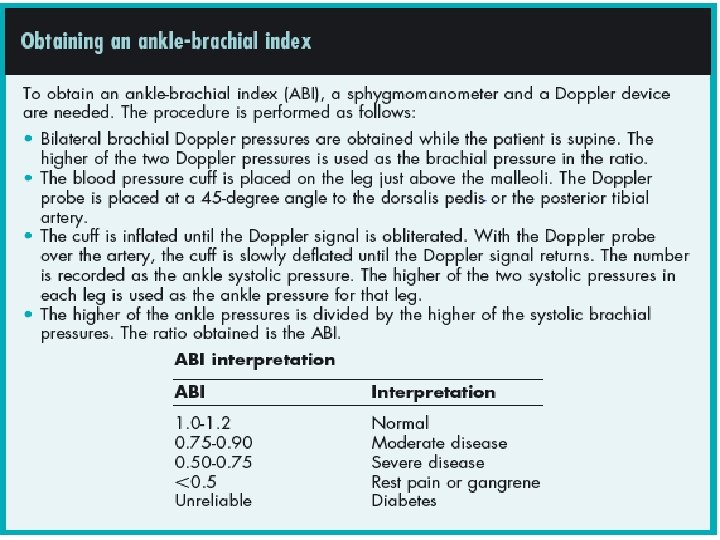
Investigations • Noninvasive vascular testing is divided into direct tests that image the vessel itself and indirect tests that demonstrate changes distal to the diseased vessel • Handheld Doppler ultrasound • Arteriogram • The Ankle Brachial Index (ABI) is the ratio of the blood pressure in the lower legs to the blood pressure in the arms. Compared to the arm, lower blood pressure in the leg is an indication of blocked arteries (peripheral vascular disease or PVD) • Segmental pressure(Pressures obtained at the level of the thigh, above the knee, calf, and ankle are compared with each other and with pressures in the other leg. )
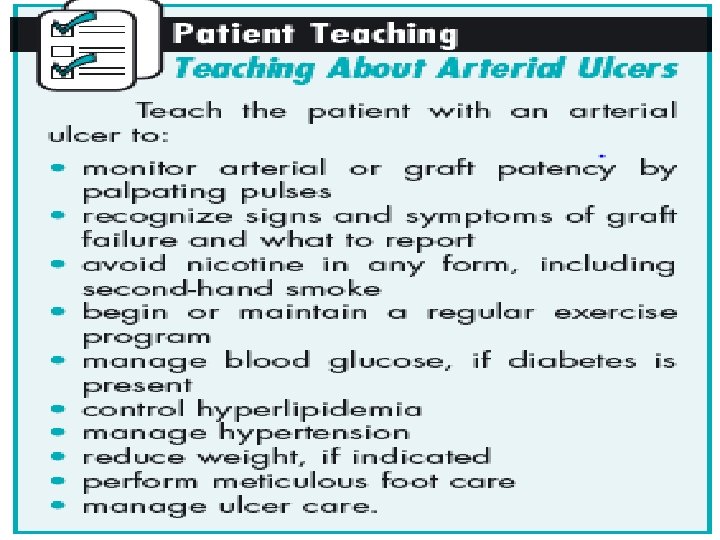
TREATING ARTERIAL ULCERS • • Treat the cause: bypass, stents, or dilation with a consult to a vascular specialist • • Patient-centered concerns: pain, quality of life, and activities of daily living • • Local wound care: • — Healable wound: debridement, moisture balance, and bacterial balance • — Maintenance wound: procedures may be more conservative because of patient or system factors causing the wound to not heal • — Nonhealable wound: requires conservative • debridement, moisture reduction, and bacterial reduction.
Nutrition – L-Arginine (vasodilator properties) oral intake of 6. 6 g/day for 2 weeks improved symptoms of intermittent claudication – Provide nutritional support with 2, 000 or more calories preoperatively and postoperatively, if possible; this has been benefited patients undergoing amputations Pain Management – Recommend walking to near maximal pain three times per week – Pain medication as indicated
Topical Therapy – Dry uninfected necrotic wound: KEEP DRY – Dry INFECTED wound: Immediate referral for surgical debridement/aggressive antibiotic therapy (Topical antibiotics are typically ineffectivefor arterial wounds) – Open Wounds • Moist wound healing • Non-occlusive dressings (e. g. solid hydrogel) • Aggressive treatment of any infection
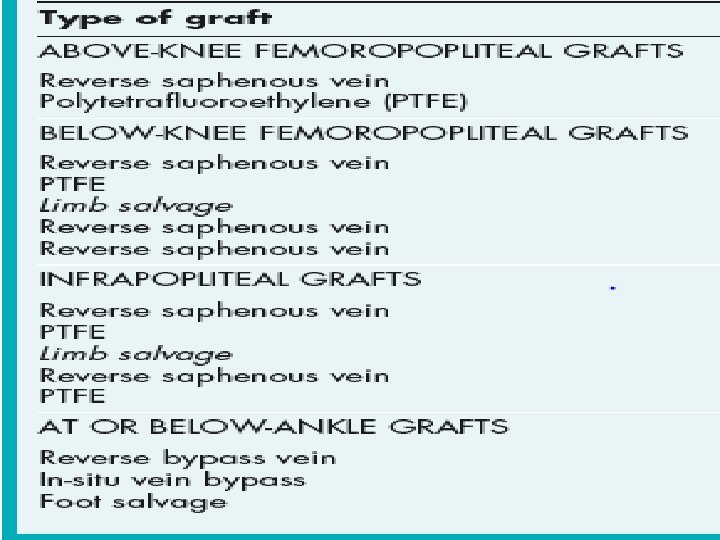
SURGICAL TREATMENT FOR ARTERIAL ULCERS • The treatment of ulceration due to arterial insufficiency depends on the level that the occlusive disease occurs. • Surgeries for arterial insufficiency are generally grouped into three major areas: • • aortoiliac bypass • • femoropopliteal bypass • • distal bypass.