ARIA guideline 2001 Allergic Rhinitis and its Impact









")







 response - The onset of sneezing & itching may occur as")



 Link between rhinitis and other conditions")





 - Nasal biopsy - Nasal swab for bacteriology")

 - MAST")
 in 15~35% of")




 - Monoclonal anti-Ig. E Ab (omalizumab ®)")




 CNS: sedation, sleepy, unable to concentrate")
 - α 2 - adrenergic")


 - Monoclonal anti-Ig. E Ab (omalizumab ) -")
: 197 -208")








 Avoid pseudoephedrine in first trimester abortion or gastroschisis")




- Slides: 65
ARIA guideline 2001, Allergic Rhinitis and its Impact on Asthma in collaboration with the WHO To update clinician’s knowledge of allergic rhinitis To highlight the impact of allergic rhinitis on asthma To provide an evidence-based approach to diagnosis To provide an evidence-based approach to treatment To provide a stepwise approach to the management of the disease
2001. 10
Definition Rhinitis: a state of persistent nasal symptoms allergy, infection, structural anomalies in the nose, hormone, drug…. Allergic rhinitis: a symptomatic disorder of the nose, induced after allergen exposure, by an Ig. Emediated inflammation of the nasal membranes 1. Dykewicz. J Allergy Clin Immunol. 2003; 111(suppl): S 520. 2. Bauchau and Durham. Eur Respir J. 2004; 24: 758. 3. Linneberg. BMJ. 2005: 331. 352.
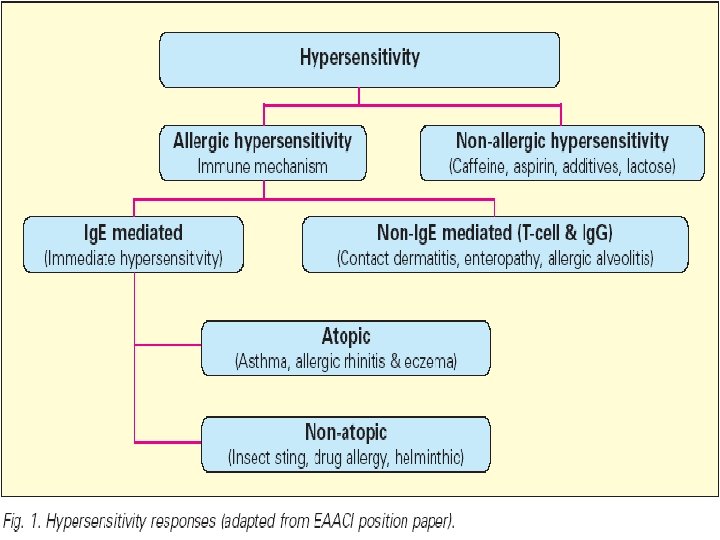
Allergy and Atopy “Allergy“: 1906 von Pirquet Antigens induce changes in reactivity in both: protective immunity and hypersensitivity reactions. apply to the "uncommitted" biologic response, immunity (a beneficial effect) or allergic disease (a harmful effect). Allergy is an acquired potential to develop hypersensitivity reactions to a normally innocuous substance and is mediated by immunological mechanisms (but not exclusively Ig. E).
Allergy and Atopy “Atopy”:Greek atopos, meaning out of place often used to describe Ig. E-mediated diseases. personal or familial (genetic) tendency to produce Ig. E antibodies in response to low doses of allergens, usually proteins, and to develop ‘classic’ allergic diseases such as asthma, rhinoconjunctivitis or eczemal dermatitis. Nonatopic allergic diseases: ★ Ig. E-independent mechanisms: ie. contact dermatitis and hypersensitivity pneumonitis ★ Ig. E responses to bee venom and drugs are not more frequent in atopic families.
Epidemiology Prevalence Overall--10 -25%, and increasing In Taiwan: 20~30% of child Hereditism One parent (+)--29%(~40%) Both parents (+)--47%(~75%) Age 11 -20 y/o
Triggers Allergens Aeroallergens Indoor Mites, dust, animals & insects Outdoor Pollens & moulds Occupational rhinitis Latex allergy
Triggers Pollutants Indoor air pollutants >80% of time indoors Tobacco smoke Outdoor air pollutants Automobile--ozone, oxides of nitrogen & sulphur dioxide
Triggers Aspirin (& NSAIDs)
Classification Seasonal a. some specific season b. usually outdoor allergen: pollen, molds… c. rhinorrhea Perennial a. throughout the year b. usually indoor allergen: house dust, mite… c. nasal obstruction Occupational
Classification Intermittent Symptoms • < 4 days per week • or < 4 weeks Mild • normal sleep • normal daily activities, sport, leisure • normal work and school • no troublesome symptoms Persistent Symptoms • > 4 days per week • and > 4 weeks Moderate-Severe one or more items • abnormal sleep • impairment of daily activities, sport, leisure • problems caused at work or school • troublesome symptoms
Symptoms & signs Symptoms a. rhinorrhea b. nasal obstruction c. nasal itching d. sneezing e. itchy or watery eye f. anosmia, nasal pain, headache
Symptoms & Signs a. Pale bluish turinates, frequently with edema “ hyperemia” --- acute infection or over use of topical medication b. Middle ear involvement: OME, eardrum retraction c. Prolonged mouth breathing (adenoid face) - Elevation of the upper lip - Over-bite - High arched palate
Symptoms & Signs d. Facial signs - “Allergic shiner” - Horizontal creases under the eyes (Dannie-Morgan line) - “Allergic salute” - supratip nasal crease e. Nasal polyposis f. signs of asthma, atopic dermatitis…
Nasal salute Nasal itching Adenoid face Allergic shiners Skoner D, Urbach A, Fireman P. In: Atlas of Pediatric Physical Diagnosis. 3 rd ed. 1997
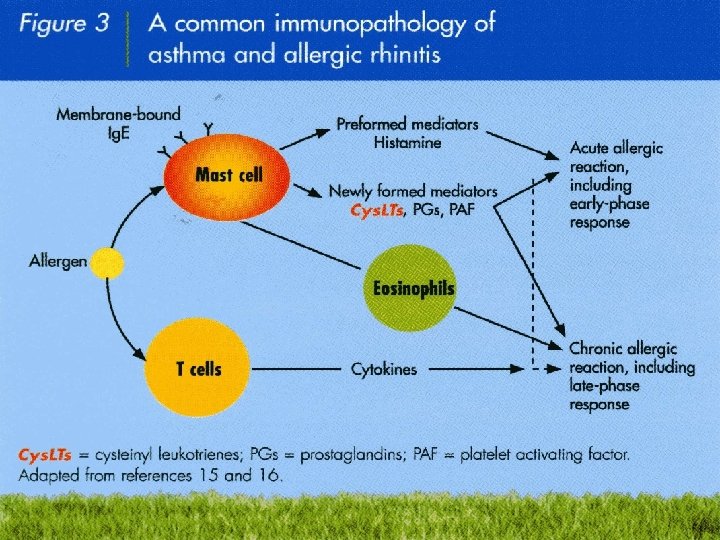
Pathophysiology Ig. E Ab mediated, type I immune response Sensitization Ig. E adhered to mast cells & basophils Preformed (stored) mediators Histamine, kinins, proteases, platelet activating factor, heparin Newly formed mediators Prostaglandin, interleukins, leukotriene, cytokines
Pathogenesis Early-phase (immediate) response - The onset of sneezing & itching may occur as early as ~30 sec, and usually peaks within minutes - Mast cell: the predominant cell - Histamine, leukotriene, prostaglandin, bradykinin, PAF (platelet activating factor) - Itching, sneezing, watery rhinorrhea, vasodilation (nasal congestion)
Pathophysiology Late/delayed phase response 50% 4~12 Hours Priming Eosinophils infiltration TH 2 -type cytokines: IL-4, 5 & GM-CSF Other mediators: IL-8, RANTES, eotaxins & MCPs Nasal blockage, and nasal hyper-reactivity
Allergy is more than histamine
Minimal persistent inflammation
“The united airways concept” (One airway, one disease) Link between rhinitis and other conditions
Co-Morbidities --Asthma p’t--60 -78% allergic rhinitis Allergic rhinitis p’t--19 -38% asthma Bronchial challenge--nasal inflammation Nasal challenge--bronchial inflammation
Co-Morbidities --Asthma Mechanism Nasal-bronchial reflex Mouth breathing caused by N-O Pulmonary aspiration of nasal contents Diagnosis Lung function test The reversibility of airflow obstruction
Co-Morbidities --Asthma Medications Both effective--intranasal steroids, antihistamines, antileukotrienes Optimal management of rhinitis may improve coexisting asthma
Diagnosis Routine tests - A typical history - General ENT examination i. Nose: boggy turbinate ii. Ear: OME, eardrum retraction iii. Eye: injected conjunctivitis with watery discharge, allergic shiner iv. Face: adenoid face, supratip nasal crease, Dannie-Morgan fold - Endoscope: rigid, flexible
Diagnosis Allergic test - Skin test - Serum specific Ig. E Nasal cytology - Eosinophilia >20% Nasal challenge - Allergen, aspirin, lysine Radiology - usually unnecessary - X-ray, CT scan
Diagnosis Optional tests (mainly for research) - Nasal biopsy - Nasal swab for bacteriology - Mucociliary function i. Nasal mucociliary clearance, ciliary beat frequency, electronmicroscope ii. Nasal inspiratory peak flow (NIPF), rhinomanometry, acoutic rhinometry iii. Olfaction, nitric oxide measurement iv. Testing for comobidities
Diagnosis Total serum Ig. E test - a poorly predictive tool for allergy screening in rhinitis and should rarely be used as a diagnostic tool - In adult: 60~100 KU/L - 35~50% of allergic rhinitis have normal Ig. E level - 20% of nonatopic individuals have elevated total Ig. E
Diagnosis Specific serum Ig. E - Phadiatop: for inhalation allergen (23 species) - MAST (Multiple Antigen Simultaneous Test) i. Semi-quantitative ii. 35 species - CAP i. CAP-1 ~ CAP-5 ii. 5 items each time “ Titer of serum Ig. E is usually unrelated with symptoms”
Diagnosis Skin test - Scratch test - Prick-puncture test i. (+) in 15~35% of symptom-free persons - Intradermal test i. more sensitive, but less safe ii. Less correlate with symptoms iii. Positive control: histamine iv. Negative control: phenol, N/S, glycerin - Induration (wheal) & surrounding erythema (flare)
Diagnosis Skin test VS specific Ig. E test Advantage i. greater sensitivity ii. rapid result iii. low cost Disadvantage i. inability in extensive eczema ii. multiple needle pricks iii. Influenced by drugs: antihistamine…. iv. maintain the potency of allergen extract v. anaphylaxis
Diagnosis Nasal provocation test - In vivo and intranasal - For more stringent criteria are needed to incriminate the suspected allergen, such as occupational allergy - Non-specific reaction to pepper or other material
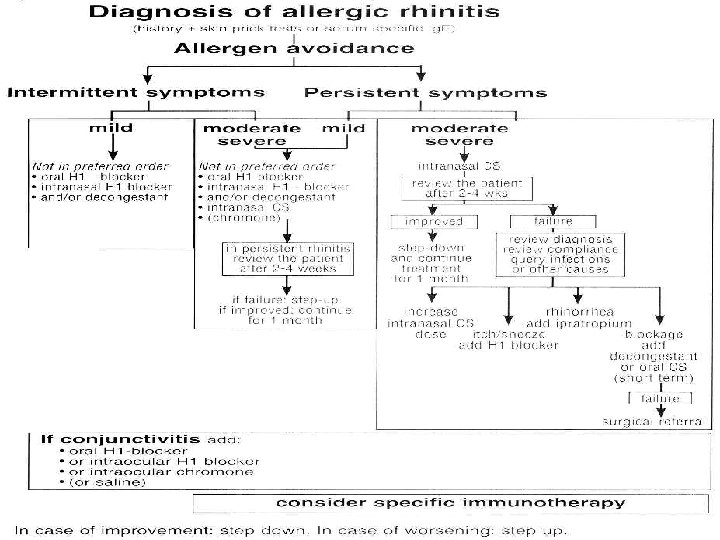
Management Allergen avoidance indicated when possible Pharmacotherapy Safety Effectiveness Easy administration Immunotherapy Cost Effectiveness Specialist prescription May alter the nature course of the disease Patient education Always indicated
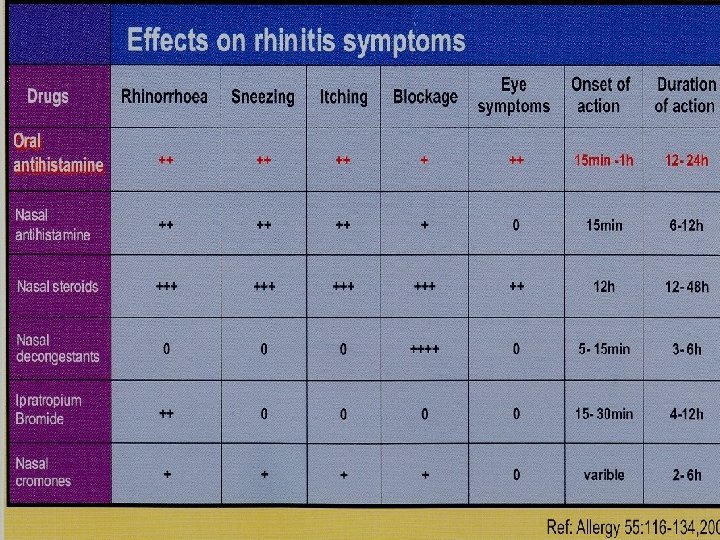
Management Allergen avoidance Oral medication - Anti-histamine - Decongestant - Corticosteroid Intra-nasal spray - Intranasal steroid - Mast cell stabilizer (Cromolyn)(Intal) - Antihistamine: Azelastine - Decongestant - Anticholinergic
Management Immunotherapy Newer agents - Anti-leukotrienes (zafirlukast®) - Monoclonal anti-Ig. E Ab (omalizumab ®) - Zileuton (Zyflo): 5 -Lipoxygenase (LO) inhibitor Surgery - SMT(submucosal turbinectomy) - Inferior turbinate cauterization - Laser, cryotherapy, chemical agent, electrocautery….
Recommendations for Management of Allergic Rhinitis: ARIA Guidelines Mild intermittent Moderate severe intermittent Mild persistent Moderate severe persistent Intranasal steroid Local cromone Second-generation nonsedating H 1 antihistamine Intranasal decongestant (<10 days) or oral decongestant Allergen and irritant avoidance ARIA = Allergic Rhinitis and its Impact on Asthma. Bousquet et al. Allergy. 2002; 57: 841. Bousquet et al. Allergy. 2003; 58: 192. Immunotherapy
Management Allergen avoidance - Encase mattress, hot washing bedding, wooden floor - Pets, toys - Cockroaches - Aeration and heating ducts - HEPA cleaner a. Single avoidance intervention is fail to reduce allergen load b. Reduce allergen load ≠ symptoms relief
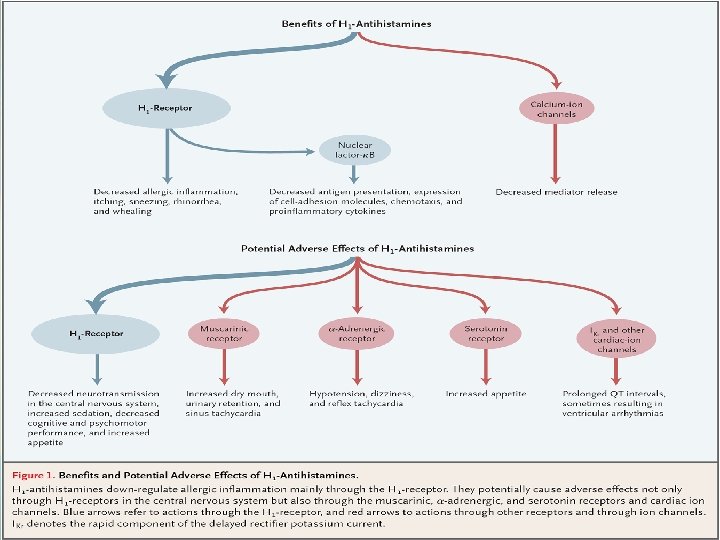
Management Anti-histamine a. 1 st generation Longifene, Homoclomin, Vena b. 2 nd generation: 1 st line agents for allergic rhinitis Loratadine(clarityne®), Cetirizine(Zyrtec®), Fexofenadine(allergra®), Clarinase® (clarityne+Peudo-E) c. Newer agent levocetirizine(Xyzal®), Desloratadine(Aerius®) d. Azelastine(Azela®)nasal spray
“Inverse agonism”
Management --Anti-histamine Side effect: (doparminergic, serotinergic, cholinergic receptor) CNS: sedation, sleepy, unable to concentrate Heart: arrhythmia(Torsades de pointes) Terfenadine, astemizole, especially in combination with macolides or ketoconazole Anti-cholinergic: urinary retention, dryness, precipitation of narrow-angle glaucoma GI upset Intranasal spray: bitter taste: 20% , sedation: 11% Astelin prescribibg information. Montvale, NJ: Med Pointe Pharmaceuticals: 2000.
Management Decongestant - α 1 - adrenergic agonist (phenylephrine) - α 2 - adrenergic agonist (Oxymetazoline, xylometazoline, naphazoline) - Nonadrenaline releaser (ephedrine, peudoephedrine, amphetamine) - Block re-uptake of noradrenaline (coccaine, TCA, phenylpropanolamine)
Management Decongestant - oral - Topical - Pay attention to patients with CV disease, poorly-controlled hypertension, glaucoma, older age, BPH, hyperthyroidism, pregnancy - > 10 days use of topical decongestant tachyphylaxis, rebound congestion (Rhinitis medicamentosa)
Management Steroid -Oral -Intranasal corticosteroids : 1 st line for moderate/severe cases or persistent symptoms and when nasal obstruction is a major concern : Low Bioavailability : Local SE: crusting, dryness, and epistaxis : No Hypothalamic-pituitary-adrenal axis effect : Children growth delay in one report. : Pregnancy: safe for inhaled steroid in asthma woman
Management Newer agents - Anti-leukotrienes (montelukast) - Monoclonal anti-Ig. E Ab (omalizumab ) - Zileuton (Zyflo): 5 -Lipoxygenase (LO) inhibitor
N Eng J Med 1999; 340(3): 197 -208
Management -Immunotherapy Effective Indication Insufficiently controlled by conventional medications Do not wish to be on medications Medications produces undesirable S. E. Not recommended in children <5 y/o
Management --Surgery An adjunctive intervention in a few highly selected patients Relief of nasal obstruction
Management -- Others Homeopathy, herbalism, acupuncture No scientific & clinical evidence
Allergic rhinitis in special conditions Pediatrics Pregnancy Elderly patients
Allergies begin in children Evolution of sensitisation to grass pollen between the ages of 0 and 6 years % sensitised Evolution of sensitisation to house dust mite between the ages of 0 and 6 years % sensitised 15 25 20 10 15 10 5 5 0 1 2 3 5 6 Age (years) Bergmann RL et al. Clin Exp Allergy 1998; 28: 965 -70. 0 1 2 3 Age (years) 5 6
“Allergic march”
Children Allergic rhinitis: unusual < 2 y/o Allergy tests can be done at any age Medications Few medications have been tested in children < 2 y/o Avoid oral and intramuscular steroids in young children Intranasal steroid, intranasal Cromolyn
Pregnancy Nasal obstruction may be aggravated Most medications cross the placenta FDA Pregnant Category: B: Cetirizine, loratadine, vena (Diphenhydramine) Budesonide nasal spray Cromolyn intranasal spray Immunotherapy: may be continued if initiated before pregnancy Initiating IT during pregnancy is not advised
Pregnancy 1 ST line: intranasal Cromolyn(Intal) Avoid pseudoephedrine in first trimester abortion or gastroschisis
Aging Change in connective tissue and vasculature of the nose A less common cause in subjects >65 y/o Atrophic rhinitis is common Medications cause rhinitis (reserpine, guanethidine, phentolamine, methyldopa, prazosin, chlorpromazine or ACE inhibitors)
Aging 2 nd-generation antihistamine: 1 st choice Topical anticholinergic For isolated rhinorrhea (ipratropium bromide nasal spray) Specific S. E. Decongestants Drugs with anticholinergic activity, or sedative effect
Cost per year in Taiwan 1 st 2 nd Intranas antihista al steroid antihistamin mine e Montelu Omaluzi Zileuton kast mab (Zyflo) (Singula (Xolair) NT 730 NT 16000 NT 20005000 NT 36004000 NT 400000 NT 70000