APPROACH TO THE PATENT WTH GLOMERULAR DSEASES Glin

 Knowledge: At the end of this lecture the students")


.")


 l Rickettsiae Connective tissue diseases")

 greater than 50 mg/kg")
 • characterized initially by dramatic increases in glomerular permeability")

 The glomerular basement membrane is normal; the cytoplasm of the")



")

 •")
 • an important lesion found to underly the nephrotic syndrome")













 MGN group common uncommon Immun dis. SLE, DM RA, Hashimoto’s")

 • Hepatitis B • Cancer")




 • MPGN is characterized by diffuse global capillary wall")
 • Combination of asymptomatic hematuria and")

, due")


 With immun deposits Infections –crioglobulinemia - HBV, HCV, Endocarditis,")




 • Most common")









 in Ig. AN, use blood pressure")
 • We suggest not treating with corticosteroids combined")

 • affects primarily children, with peak incidence between the ages")













. •")


treated as dictated by the extrarenal")
 and class IV LN (diffuse LN)— maintenance therapy •")




- Slides: 94
APPROACH TO THE PATİENT WİTH GLOMERULAR DİSEASES Gülçin Kantarcı, MD Professor of Nephrology Department
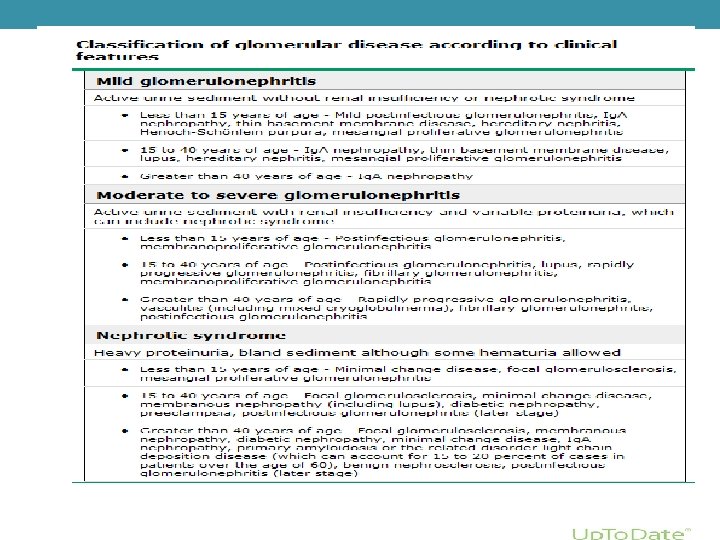
OBJECTIVES (knowledge, skills and attitudes) Knowledge: At the end of this lecture the students 1. Has a good understanding the diagnosis and the differential diagnosis of Glomerular Diseases with their emergent treatment requirements and methods. 2. Has a knowledge about diagnosis methods of Glomerular Diseases. (Laboratuary tests, screening tests, other invasive and non-invasive medical procedures) Skills: 3. Can name the possible diagnosis and make a differential diagnosis of Glomerular Diseases. 4. Can use the diagnosis methods for Glomerular Diseases economically and properly. (Lab. tests, screening tests, other invasive and non-invasive medical procedures) 5. Can interpret the result of these test correctly. 6. Can choose between emergent and non-emergent situations, and give emergent treatment for diseases. Attitudes: 7. Presents a worthy thought, attitude and behavior appropriate for a physician in patient communication.
REFERENCE 1. Current Medical Diagnosis and Treatment, Maxine A. Papadakis, Stephen J. Mc. Phee, Eds. Michael W. Rabow, Associate Ed. http: //accessmedicine. com Chapter 22. Glomerular Diseases 2. Bates' Guide to Physical Examination & History Taking 11 th edition, Bickleys LS, Szilagyi PG; Lippincott Williams and Wilkins¸ 3. Kumar and Clark's Clinical Medicine, 8 th edition; Kumar & Clark, Elsevier 4. Andreoli and Carpenter's Cecil Essentials of Medicine 8 th edition, Andreoli and Carpenter, Elsevier PART 11: RENAL AND GENITOURINARY DISEASES 123: Glomerular Disorders and Nephrotic Syndromes
Glomerulus
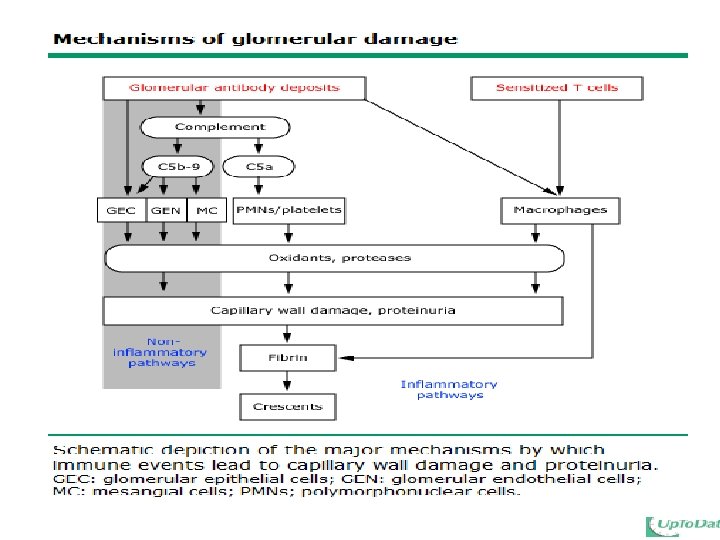
• Most glomerular diseases are immune-mediated, and described as glomerulonephritis (GN).
GLOMERULAR INFLAMMATION AND INJURY
GLOMERULONEPHRITIS Primary GN • Minimal Change Disease • FSGS • Membranous GN • Idiopatic MPGN • Ig. A nephropathy • Proliferatif GN
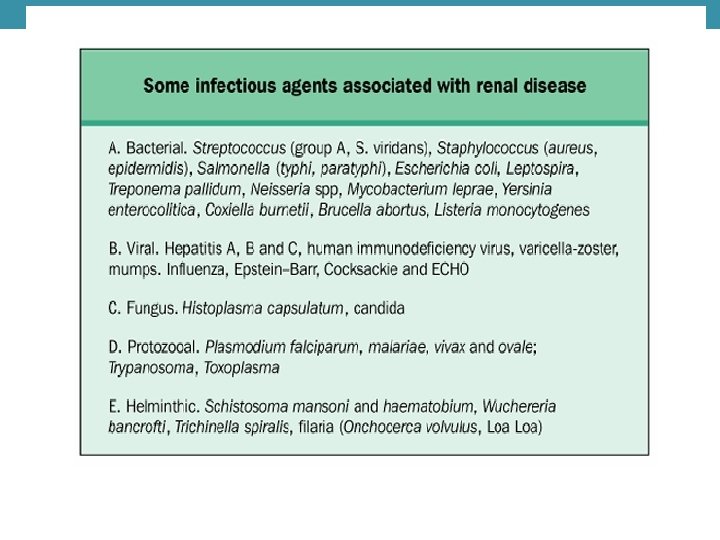
Sekonder GN İnfective l Fungi (Candida albicans, Coccidioides immitis) l Rickettsiae Connective tissue diseases l Henoch-Schönlein purpura l Polyarteritis nodosa l SLE l Wegener’s granulomatosis Glomerular basement membrane diseases l Goodpasture’s syndrome Hematologic dyscrasias l Mixed Ig. G-Ig. M cryoglobulinemia l Serum sickness l Thrombotic thrombocytopenic l purpura–hemolyticuremic syndrome
Viral: l l l l l Coxsackievirus Cytomegalovirus Epstein-Barr virus Hepatitis B virus Hepatitis C virus Herpes zoster virus Measles Mumps Varicella
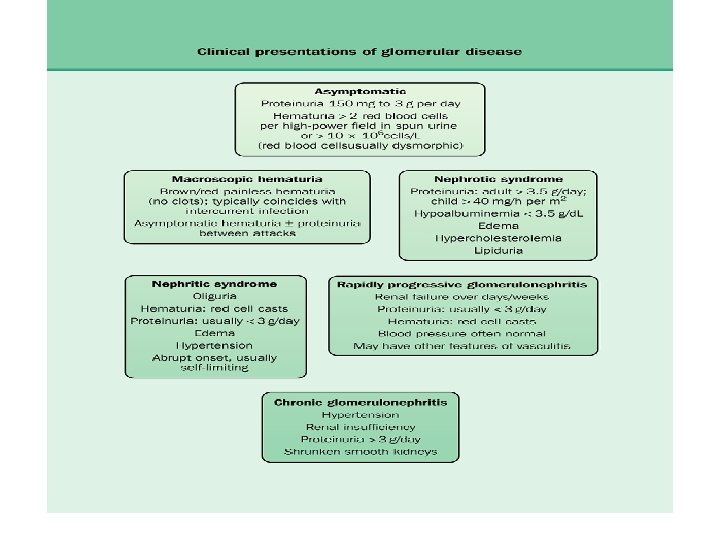
GLOMERULAR DISEASES WITH NEPHROTIC SYNDROME Nephrotic synd: edema, Nephrotic-range proteinuria) greater than 50 mg/kg per day or 40 mg/h/m 2 in children and 3. 5 g/24 h in adults , hyperlipidemia • Minimal change disease (MCD) • Focal Segmental Glomerulosclerosis (FSGS) • Membranous nephropathy (MN)
MINIMAL CHANGE DISEASE (MCD) • characterized initially by dramatic increases in glomerular permeability in association with little or no structural abnormalities by light microscopy. • lipoid nephrosis Munk (1913) • MCD is most common in children, In adults, especially in elderlies associated with secondary causes • 70% to 90% of cases of nephrotic syndrome in children younger than age 10 years and 50% of cases in older children. • Minimal change glomerulopathy also causes 10% to 15% of cases of primary nephrotic syndrome in adults. • %15 -20 nephritic features may occur • MCD in children mostly (%80 -90) idiopatic
HISTOPATHOLOGY • The principal target of injury is the podocyte, ***podocytopathies • Light microscopy: lack of definitive alteration in glomerular structure. Lipid droplets in the tubuler cells • Immunofluorescence: also shows no change • Electron mic: fusion of epithelial foot processes
Minimal-change disease (electron microscopy) The glomerular basement membrane is normal; the cytoplasm of the podocytes is vacuolated, with effacement of foot processes and microvilli. Methenamine silver, 2800×.
Laboratory findings of MCD • severe proteinuria. • Microscopic hematuria is seen in fewer than 15% of patients. • Volume contraction may lead to a rise in both the hematocrit and • • hemoglobin. ESR is increased as a consequence of hyperfibrinogenemia as well as hypoalbuminemia. The serum albumin <2 g/d. L and, in more severe cases, <1 g/d. L. Total cholesterol, LDL, and triglyceride levels are increased. Pseudohyponatremia has been observed in the setting of marked hyperlipidemia. Renal function is usually normal, although a minority of patients have substantial AKI. Ig. G levels may be profoundly decreased—a factor that may result in susceptibility to infections. Complement levels are typically normal in patients with minimal change glomerulopathy
Secondary causes of MCD • Drugs -NSAID -penicillin -trimetoprim • Toxins -Mercury -lead -bee stings • Infection -Mononucleosis - HIV - Immunizations • Tumors -Hodgkins lymphoma -other lymhoproliferative dis. , -Carcinoma • Obesity
Specific treatment: corticosteroids • Emprical steroid theraphy for children <10 • In children who have received empirical treatment, a renal biopsy is indicated when there is failure to respond to a 4 - to 6 -week course of prednisone. • oral prednisone be administered as a single daily dose starting at 60 mg/m 2 /day • or 2 mg/kg/day to a maximum 60 mg/day
Clinical course of MCD as related to steroid theraphy • STEROID-SENSITIVE NEPHROTIC SYNDROME (SSNS) - complete remission of proteinuria within 8 -12 weeks with infrequent relapses • FREQUENTLY RELAPSING and STEROID DEPENDENT (FR-SD) -relapses occur during the taper of steroids -relapses occur at rate of twice every 6 months or six times every 18 months -relapses occur within 2 weeks of cessation of theraphy • STEROID-RESISTANT NEPHROTIC SYNDROME (SRNS) -Failure to obtain a remission within 12 weeks
PROGNOSIS • In adults 85 -90 % survival rate • The potential efficacy of therapy must be considered in relation to the natural history of the disease. • Untreated idiopathic MCD was associated with a risk of mortality due to infection and less commonly thromboembolism
complications • Related to persistent NS (peritonitis, ARF, CKD in steroid resistant patients) • Side effect of therapy( stra, cataracts, acne, cushingoid face, hyperglisemia, HT)
FOCAL SEGMENTAL GLOMERULOSCLEROSIS (FSGS) • an important lesion found to underly the nephrotic syndrome in adults and a frequent lesion in children and adolescents • Pathology: a focal process; not all glomeruli are involved, the glomeruli are segmentally sclerotic, and portions of the involved glomeruli may appear normal by light microscopy. • Nonsclerotic glomeruli and segments usually have no staining for immunoglobulins or complement. • The ultrastructural features of FSGS on electron microscopy include focal foot process effacement.
FSGS
histologic variants NORMAL Glomerulus Collapsing Classical Tip lesions
Laboratory findings • Hypoproteinemia is common in patients with FSGS and the serum albumin concentration may fall to below 2 g/d. L, especially in patients with the collapsing variant. • Hypogammaglobulinema and hyperlipidemia are typical; serum complement components are generally in the normal range. • Serologic testing for HIV infection should be obtained for all patients with FSGS, especially those with the collapsing pattern.
Clinical manifestations § peripheral edema, § hypoalbuminemia, and § nephrotic range proteinuria. § Patients with FSGS also commonly have hypertension, and many have microscopic hematuria. § The level of kidney function may vary.
The relative frequencies of clinical manifestations : § Nephrotic range proteinuria - 60 to 75 % § Microscopic hematuria - 30 to 50 % § Hypertension - 45 to 65 % § Renal insufficiency - 25 to 50 %
PROGNOSIS OF FGS • Untreated primary FSGS often follows a progressive course to end-stage renal disease (ESRD). • The rate of spontaneous complete remission among patients with nephrotic syndrome is unknown, but is probably less than 10 percent. • Spontaneous remission is more likely to occur among patients with normal kidney function and non-nephrotic proteinuria.
Response to therapy • The strongest prognostic indicator is the degrees of reduction in proteinuria • complete response : <200 to 300 mg/day. • partial response reduction ≥ 50 % • relapse is return of proteinuria to ≥ 3. 5 g/day after a complete or partial remission. • Steroid-dependence relapse while on therapy or requirement for continuation of steroids • Steroid-resistance little or no reduction in proteinuria after 12 to 16 weeks of prednisone therapy
Therapy of MCD & FSGS • Prednisone theraphy: not to exceed 60 mg/day • 50% responding 2 -6 wk • Cyclosporine therapy is the second choice for FSGS
• ACEI may provide a substantial reduction in proteinuria and a long-term renoprotective effect that may be equal to, or greater than, that of immunosuppressive therapy. • Response rates to immunosuppressive therapy in primary FSGS 45% for complete remission, 10% for partial remission, 45% for no response.
Membranous GN • Idiopathic membranous glomerulopathy is the most common cause of nephrotic syndrome in adults (25% of adult cases) and can occur as an idiopathic (primary) or secondary disease. • Secondary membranous glomerulopathy is caused by autoimmune diseases (e. g. , lupus erythematosus, autoimmune thyroiditis), infection (e. g. , hepatitis B, hepatitis C), drugs (e. g. , penicillamine, gold), and malignancies (e. g. , colon cancer, lung cancer).
Membranous GN • In patients over the age of 60, membranous glomerulopathy is associated with a malignancy in 20% to 30% of patients. The peak incidence of membranous glomerulopathy is in the fourth or fifth decade of life. Pathology • The characteristic histologic abnormality in MGN is diffuse global capillary wall thickening and the presence of subepithelial immune complex deposits.
The immun deposits of Ig G and complement components develop on the subepithelial surface of the glomerular capillary wall
spikes Light microscopy in membranous nephropathy, uniform increase in the thickness of the glomerular capillary walls throughout the glomerulus without any increase in glomerular cellularity. Spikes of matrix emanating from the outer surface of the basement membrane indicative of advanced MN are revealed by silver–methenamine stain (× 400).
Conditions associated with (secondary) MGN group common uncommon Immun dis. SLE, DM RA, Hashimoto’s dis. Ankylosing spondylis. Pr. Biliary cirrhosis Infectious HBV HCV, malaria, syphilis Drugs and toxins Gold , NSAIDs Mercury, captopril, formaldehyde Miscellaous Tumors, renal transplant Sarcoidosis, Sickle cell dis.
Clinical manifectations • Nephrotic syndrome 80% • Asymtomatic non-nephrotic proteinuria 20% • Proteinuria (5 -15 g/day) • Microscobic hematuria may be seen 50% of adults • Renal vein thrombosis 40% • Renal function usually well preserved at the on set of dis.
Common secondary causes • Membranous lupus nephritis (Class V) • Hepatitis B • Cancer (adults over 50 years incidence of malignancy in MGN 20%) • Renal allografts
Prognosis of pr. MGN • Spontaneous complete remission of proteinuria occurs in 5 to 30 % • Spontaneous partial remission (≤ 2 g of proteinuria per day) occurs in 25 to 40 % • ESRD in untreated patients is § 14 % at 5 years, § 35 % at 10 years, § 41 % at 15 years
Laboratory findings in MGN • Proteinuria is usually more than 3 g of protein per 24 hours and • • • may exceed 10 g/day in 30% of patients. Microscopic hematuria is present in 30% to 50% of patients Renal function is typically preserved at presentation. Hypoalbuminemia is observed if proteinuria is severe. Complement levels are normal; however, the complex of terminal complement components known as C 5 b-9 is found in the urine in some patients. Tests for hepatitis B, hepatitis C, syphilis, and immunologic disorders such as lupus, mixed connective tissue disease, and cryoglobulinemia should be obtained to exclude secondary causes.
Theraphy of MGN • Supportive care including ACEI, lipid-lowering therapy • Corticosteroids • Alkylating agents (chlorambucil or cyclophosphamide), with or without concurrent corticosteroid treatment -Chlorambucil (0. 2 mg/kg/day) or cyclophosphamide, alternating monthly with daily prednisone(0. 5 mg/kg/day), in combination with intravenous pulse methylprednisolone(1 g/day) for the first 3 days of each month • Cyclosporine • The high prevalence of deep vein thrombosis in patients with membranous glomerulopathy (up to 45%) has led to the use of prophylactic anticoagulation for patients with proteinuria greater than 10 g/day
Management of MGN • Adult patients with good prognostic features, with less than 4 g/day proteinuria and normal renal function, should be managed conservatively. • Patients at moderate risk (persistent proteinuria between 4 and 6 g/day after 6 months of conservative therapy and normal renal function) or high risk of progression (persistent proteinuria greater than 8 g/day with or without renal insufficiency) should be considered for immunosuppressive therapy • Individuals who have advanced chronic kidney disease and in whom serum creatinine exceeds 3 to 4 mg/d. L are best treated by supportive care awaiting dialysis and renal transplantation
Membranoproliferative GN (Mesangial Capillary Glomerulonephritis) • MPGN is characterized by diffuse global capillary wall thickening, frequently with a double contoured appearance and either subendothelial deposits (type I MPGN) or deposits within the mesangium and basement membrane (type IIMPGN).
Clinical presentations of MPGN • Nephrotic syndrome (50%) • Combination of asymptomatic hematuria and proteinuria (25%) • Acute nephritic syndrome (25%) • Hypertension is typically mild • renal dysfunction occurs ( 50%)
Classification of MPGN
Histology of MPGN light microscopy: • thickening of the glomerular basement membrane (GBM), due to immune complex deposition and to interposition of the mesangial cell cytoplasm between the GBM and the endothelial cell; • hypercellularity, lobular appearance of the glomerular tuft
lobular appearance of the glomerular tuft increased glomerular cellularity thickening of all capillary walls with double contours, cellular proliferation
TYPES OF MPGN Primary or idiopathic • Type I: mesangiocapillary GN • Type II: dense deposit disease • Type III: an immune complex disease, similar to type 1.
Secondary (associated with other diseases) With immun deposits Infections –crioglobulinemia - HBV, HCV, Endocarditis, Malaria, EBV, HIV, mycoplasma Autoimmun diseases -SLE, RA, Sjörgen’s syndrome Dysproteinemia -Light chain deposit dis. , Waldernstrom’s macroglobulinemia, fibrilar Without immun deposits Chronic liver disease -Cirrhosis, α 1 antitripsin deficiency Thrombotic microangiopathies - HUS/TTP, Antiphospholipid antibody Syn, Sickle cell anemia
Laboratory findings • Hematuria is the hallmark of patients presenting with MGPN, • The degree of proteinuria varies widely. • Renal insufficiency occurs in a variable number of cases, but it is the most ominous feature of the acute nephritic syndrome. • Serologic and clinical evidence of cryoglobulinemia, hepatitis C, hepatitis B, osteomyelitis, subacute bacterial endocarditis, or infected ventriculoatrial shunt should be sought in type I MGPN. • C 3 is persistently depressed in approximately 75%to 90%of MPGN patients. • C 3 nephritic factor is found in 60% of cases of type II MPGN.
PROGNOSIS bad prognostic signs: at presentation include • the nephrotic syndrome, • renal insufficiency, • hypertension, • on renal biopsy, crescents good long-term prognosis: asymptomatic hematuria and proteinuria , focal glomerular involvement on renal biopsy.
Theraphy of MPGN • The treatment of type I MPGN is based on the underlying cause of the disease process. MPGN associated with cryoglobulinemia and hepatitis C should be aimed at treating hepatitis C virus infection (interferon/ribavirin), • The treatment of MPGN associated with lupus or with scleroderma should be based on the principles of care of those rheumatologic conditions. • Most recommendations for the treatment of idiopathic type I MPGN are limited to studies in children where low-dose prednisone therapy improves renal survival.
New immunsuppresive regiments • mycophenolate mofetil + corticosteroids (5 grams/day at baseline to 2 and 2. 6 grams/24 hours at 12 and 18 months), Original Article Mycophenolate mofetil treatment for therapy-resistant glomerulopathies SAHIN GM, SAHIN S, KANTARCI G. NEPHROLOGY 2007; 12, 285– 288
GLOMERULAR DISEASES THAT CAUSE NEPHRITIC SYNDROME Ig. A nephropathy (Ig. AN) • Most common lesion found to cause primary glomerulonephritis throughout most developed countries of the world. • Ig. A nephropathy common among Asians and Caucasians, • 2: 1 male to female predominance. • The etiology of Ig. A nephropathy is unknown, but infections and/or genetic characteristics may predispose to the development of kidney disease. • Ig. A nephropathy is often suspected on the basis of the clinical history, but can be confirmed only by kidney biopsy.
Clinical findings Most patients with Ig. AN present with • gross hematuria (single or recurrent), usually following an upper respiratory infection (40– 50%) • microscopic hematuria with or without mild proteinuria incidentally detected on a routine examination. (40%) • Nephritic syndrome (10%) • Malignant hypertension (<5%) • Rarely, patients may develop AKI with or without oliguria, due either to crescentic Ig. AN, or to gross hematuria causing tubular occlusion and/or damage by red cells.
Clinical features of Ig. AN • Episodes of macroscopic hematuria tend to occur with a close temporal relationship to upper respiratory infection, including tonsillitis or pharyngitis. • The timing differs from that for PSGN, which has an interval period of 7 to 14 days between the onset of infection and overt hematuria.
Clinical features of Ig. AN • Systemic symptoms are frequently found, including nonspecific symptoms such as malaise, fatigue, muscle aches and pains, and fever. • Microscopic hematuria and proteinuria persist between episodes of macroscopic hematuria. • Associated hypertension is common
Clinical features of Ig. AN • Although Ig. A nephropathy was previously thought to carry a relatively benign prognosis, it is estimated that renal insufficiency may occur in 20% to 30% of patients within 2 decades of the original presentation. • Renal failure typically follows a slowly progressive course, ü a minority of patients with Ig. A nephropathy manifests a fulminant course resulting in a rapid progression to end-stage renal disease.
Ig. A nephropathy may be the glomerular expression of a systemic disease Henoch-Schönlein purpura
poor prognoctic features • Sustained hypertension, • Persistent proteinuria greater than 1 g/day, • Impaired renal function, • Nephrotic syndrome
Laboratory Findings of Ig. AN • microscopic hematuria and dysmorphic erythrocytes • Proteinuria majority of subjects have less than 1 g/day of protein. • There are no specific serologic or laboratory tests diagnostic of Ig. A nephropathy or Henoch-Schönlein purpura. • Although serum Ig. A levels are elevated in up to 50% of patients, the presence of elevated Ig. A in the circulation is not specific for Ig. A nephropathy. • Complement levels such as C 3 and C 4 are typically normal
PATHOLOGY immunofluorescence microscopy • globular deposits of Ig. A (often accompanied by C 3 and Ig. G) in the mesangium and, to a lesser degree, along the glomerular capillary wall. large, globular mesangial Ig. A deposits
Treatment of Ig. AN
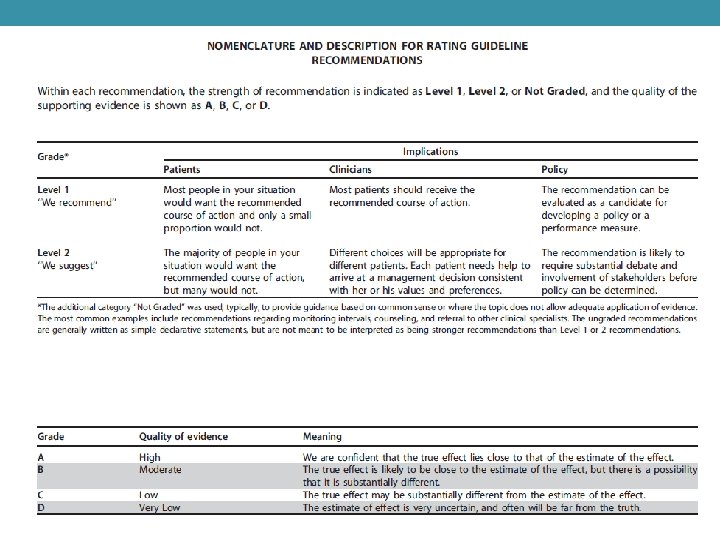
• ACE-I or ARB treatment (1 B) in Ig. AN, use blood pressure treatment goals of 130/80 mm. Hg in patients with proteinuria <1 g/day, and 125/75 mm. Hg when initial proteinuria is >1 g/day • Corticosteroids(2 C)in Ig. AN patients with persistent proteinuria>1 g/day, despite 3– 6 months of optimized supportive care (including ACE-I or ARBs and blood pressure control), and GFR >50 ml/min per 1. 73 m 2, receive a 6 -month course of corticosteroid therapy. • Fish oil in treatment(2 D)of Ig. AN with persistent proteinuria >1 g/d, despite 3– 6 months of optimized supportive care (including ACE-I or ARBs and blood pressure control).
Immunosuppressive agents (cyclophosphamide, azathioprine, MMF, cyclosporine) • We suggest not treating with corticosteroids combined with cyclophosphamide or azathioprine in Ig. AN patients (unless there is crescentic Ig. AN with rapidly deteriorating kidney function (2 D) • We suggest not using immunosuppressive therapy in patients with GFR <30 ml/min per 1. 73 m 2 unless there is crescentic Ig. AN with rapidly deteriorating kidney function
Glomerular Diseases Associated with Infection • GN may occur as a concequence of infections. • Post strep. GN: Patients presenting with features of acute GN recent infection of pharynx or skin with group A b-hemolytic strep. • Diagnosis is suggested by history and urinalysis and confirmed by low complement. Prognosis is excellent. Treatment is supportive
Acute poststreptococcal glomerulonephritis (PSGN) • affects primarily children, with peak incidence between the ages of 2 • • • and 6 years. It may occur as part of an epidemic or sporadic disease, and only rarely do PSGN and rheumatic fever occur concomitantly. A latent period is present (7– 21 days) from the onset of pharyngitis to that of nephritis. The hematuria is microscopic in more than two thirds of cases. Hypertension occurs in more than 75% of patients The clinical manifestations of acute PSGN typically resolve in 1 to 2 weeks as the edema and hypertension disappear after diuresis. Both the hematuria and proteinuria may persist for several months, but are usually resolved within a year.
Laboratory findings • presence of dysmorphic red blood cells or red blood cell casts. • Proteinuria is nearly always present, typically in the subnephrotic range. • Nephrotic-range proteinuria may occur in as many as 20% of patients and is more frequent in adults than in children. • Throat or skin cultures may reveal group A streptococci • elevated ASO titer above 200 units may be found in 90% of patients; • CH 50 and C 3 are reduced
Diffuse proliferative GN
Treatment of acute PSGN • Supportive therapy may require the use of loop diuretics such as furosemide to ameliorate volume expansion and hypertension
RAPIDLY PROGRESSIVE GLOMERULONEPHRITIS AND CRESCENTIC GLOMERULONEPHRITIS • Immune Complex–Mediated Crescentic GN (e. g. , MPGN, PSGN, or Ig. A nephropathy) • Anti–Glomerular Basement Membrane GN • 10% to 20% of crescentic GN • This disease is characterized by circulating antibodies to the GBM and deposition of Ig. G or rarely Ig. A along the GBM. Anti-GBM disease occurs as a renal-limited disease (anti-GBM glomerulonephritis) and as a pulmonary-renal vasculitic syndrome (Goodpasture syndrome). • Pauci-Immune Crescentic Glomerulonephritis
Renal and Systemic Vasculitis
Pauci-Immune Crescentic Glomerulonephritis • The characteristic feature of pauci -immune crescentic glomerulonephritis is a focal necrotizing and crescentic glomerulonephritis in association with a circulating ANCA. • Pauci-immune crescentic glomerulonephritis is usually a component of a systemic small vessel vasculitis, Segmental glomerular necrosis and crescent formation in a patient with ANCA–associated small vessel vasculitis. The fibrinoid material is red. The uninvolved segments appear normal.
ANCA-associated syndromes • Microscopic polyangiitis • Wegener granulomatosis • Churg-Strauss syndrome
• The presence of arteritis in a biopsy specimen with pauci- immune crescentic glomerulonephritis indicates that the glomerulonephritis is a component of a more widespread vasculitis, such as microscopic polyangiitis, • Wegener granulomatosis, or the Churg-Strauss syndrome. • The pathogenesis of pauci-immune crescentic glomerulonephritis is currently not fully understood. • Many patients have a circulating ANCA, it has not been conclusively proved that ANCA are involved in the pathogenesis of pauci-immune small vessel vasculitis or glomerulonephritis.
Laboratory Findings • Approximately 80% to 90% of patients with pauci-immune necrotizing and crescentic glomerulonephritis will have a circulating ANCA. • By indirect fluorescence microscopy on alcohol fixed neutrophils, ANCA yields two patterns of staining: • perinuclear (P-ANCA) • cytoplasmic (C-ANCA)
• 60 -70 % patients with pauci-immune necrotizing crescentic glomerulonephritis without clinical evidence of Systemic vasculitis will have MPO-ANCA or P-ANCA, • approximately 30% will have PR 3 -ANCA or C-ANCA. • Urinalysis findings include hematuria with dysmorphic red blood cells, with or without red blood cell casts, and proteinuria. • Serum creatinine usually is elevated at the time of diagnosis and rising • Serum complement component levels are typically within normal limits.
Fibrillary immunotactoid glomerulopathy • characterized by patterned deposits seen by electron microscopy. • Most renal pathologists distinguish fibrillary glomerulonephritis from immunotactoid glomerulopathy based on the presence of fibrils of approximately 20 -nm diameter in the former and larger 30 - to 40 -nm diameter microtubular structures • The etiology and pathogenesis of fibrillary glomerulonephritis and immunotactoid glomerulopathy are not known, but both conditions have been associated with lymphoproliferative diseases.
Clinical features • less than 1% of native renal biopsies. • Patients typically present with a mixture of the nephrotic and nephritic syndrome features. • Proteinuria is typically in the nephrotic range. • Renal insufficiency, hematuria, and hypertension are common at the time of presentation. • 40% to 50% of patients develop end-stage renal disease within 6 years of presentation
Secondary Glomerular Diseases - SLE - Antiphospholipid antibody syndrome - Polyarteritis nodosa - Churg-Strauss syndrome - Glomerular involvement in other vasculitides (temporal arteritis, takayasu disease) - Sjögren syndrome, sarcoidosis, amyloidosis, monoclonal immunoglobulin deposition disease
Lupus nephritis • Renal involvement is common in idiopathic systemic lupus erythematosus (SLE). • An abnormal urinalysis with or without an elevated plasma creatinine is present in a large proportion of patients at the time of diagnosis, and may eventually develop in more than 75 % of cases.
EPIDEMIOLOGY • The prevalence of clinically evident renal disease in patients with SLE ranges from 40 to 75 percent. • Most renal abnormalities emerge soon after diagnosis (commonly within the first 6 to 36 months)
PATHOGENESIS • The pattern of glomerular injury seen in systemic lupus erythematosus (and in other immune complex-mediated glomerular diseases) is primarily related to the site of formation of the immune deposits, which are primarily due to anti-DNA.
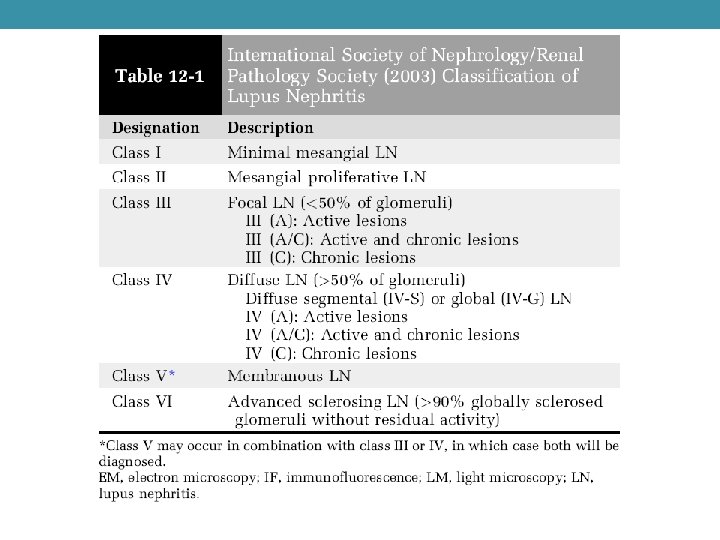
Treatment of LN • Class I LN (minimal-mesangial LN)treated as dictated by the extrarenal clinical manifestations of lupus. (2 D) • Class II LN (mesangial-proliferative LN) and proteinuria <1 g/d as dictated by the extrarenal clinical manifestations of lupus. (2 D) • Class II LN with proteinuria >3 g/d be treated with corticosteroids or CNIs as described for MCD (2 D) • Class III LN (focal LN) and class IV LN (diffuse LN)—initial therapy with corticosteroids (1 A), combined with either cyclophosphamide (1 B) or MMF (1 B). • If patients have worsening LN (rising SCr, worsening proteinuria) during the first 3 months of treatment, a change be made to an alternative recommended initial therapy, or a repeat kidney biopsy be performed to guide further treatment. (2 D)
Class III LN (focal LN) and class IV LN (diffuse LN)— maintenance therapy • after initial therapy is complete, patients with class III and IV LN receive maintenance therapy with azathioprine (1. 5– 2. 5 mg/kg/d) or MMF (1– 2 g/d in divided doses), and low-dose oralcorticosteroids (1 B) • CNIs with low-dose corticosteroids be used for maintenance therapy in patients who are intolerant of MMF and azathioprine. (2 C) • After complete remission is achieved, maintenance therapy be continued for at least 1 year before consideration is given to tapering the immunosuppression. (2 D)
class V LN • We recommend that patients with class V LN, normal kidney function, and non–nephrotic-range proteinuria be treated with antiproteinuric and antihypertensive medications, and only receive corticosteroids and immunosuppressives as dictated by the extrarenal manifestations of systemic lupus. (2 D) • We suggest that patients with pure class V LN and persistent nephrotic proteinuria be treated with corticosteroids plus an additional immunosuppressive agent: cyclophosphamide (2 C), or CNI (2 C), or MMF(2 D), or azathioprine (2 D).
C 1 q Nephropathy • C 1 q nephropathy refers to a disorder in which mesangial proliferation is associated with mesangial deposits on electron microscopy and prominent C 1 q deposits on immunofluorescence microscopy. • C 1 q nephropathy has been thought to be a subgroup of primary focal segmental glomerular sclerosis
• reports describe different symptoms, histopathologies, therapeutic responses and prognoses, suggesting that C 1 q nephropathy may be a combination of several disease groups rather than a single disease entity. • C 1 q nephropathy may be associated with either MCD, FSG, or proliferative glomerulonephritis. Criteria: predominant C 1 q deposits on immunofluorescence microscopy and no clinical evidence of systemic lupus erythematosus.
SUGGESTED READING Goldman's Cecile Medicine 24 th edition Elsevier Goldman L, Schafer AI Case files Internal Medicine 5 th edition Mc Graw Hill LANGE Toy Patlan The Cleveland Clinic Intensive Review of Internal Medicine 5 th edition Lippincott Williams Stoller JK, Michota FA, and Wilkins Mandell BF